Sjogren’s syndrome (SS) is a chronic autoimmune disorder which is characterized by lymphocyte-mediated destruction of exocrine glands, which produces the classical symptoms of dry eyes and dry mouth, which is referred to as primary SS or the Sicca complex. When it is associated with another autoimmune disease such as rheumatoid arthritis or lupus erythematosus, the condition is termed as secondary SS. One of the known major complications in patients with Sjogren’s syndrome is the occurrence of Non-Hodgkin’s lymphoma of B cell type. It is not uncommon for malignant lymphomas to occur in head and neck region at nodal and sometimes, extranodal sites. However, only rarely may they involve the oral cavity primarily. This case report describes a rare occurrence of isolated extranodal lymphomas in the upper and lower lips of a patient, which clinically resembled a mucocele, and eventually was diagnosed as lymphoma which was associated with Sjogren’s syndrome, thereby stressing the importance which was played by an oral diagnostician.
Sjogren’s syndrome, Non-Hodgkin’s lymphoma, Isolated extranodal lymphoma, Lips
Case Report
A 62-year-old female patient reported to the Department of Oral medicine and Radiology with chief complaint of loose fitting upper and lower dentures. The patient also reported of having noticed a persistent swelling in her lower lip since 6 months. On eliciting her history, it was revealed that the swelling had gradually increased in size over the past 6 months and that it had been relatively asymptomatic. There was no history of trauma, lip biting, decrease in size of the swelling, secondary changes which were associated with the swelling or similar swellings which were noticed in other parts of the body. Her medical history revealed that the patient was a known hypertensive since 15 years and that she was on medication. Patient also gave a history of consulting various doctors for the complaint of pain in her knee joints since 8-10 years. Her personal history was unremarkable, except for her sleep pattern, which was disturbed and she had been taking anti anxiety medications since 6 months. On general physical examination, patient’s blood pressure was found to be elevated. There was no history of weight loss or any other constitutional symptoms.
On local examination, a spherical solitary swelling [Table/Fig-1] . which measured approximately 1cm x 1.3 cm in size, was noticed on the right side of lower labial mucosa, with normal appearing overlying mucosa. The swelling was nontender and firm in consistency. Another swelling (of which the patient was not aware) was seen, which measured 0.8cm x 1cm in size, over the upper right side of labial mucosa, which involved the mucobuccal fold. The colour of the overlying mucosa was a bluish hue [Table/Fig-2] . The swelling was non-tender and rubbery in consistency. Other findings included, no pooling of saliva in the floor of the mouth, which coincided with Challacombe Clinical Oral Dryness Scale 4 and a <0.5ml unstimulated salivary flow rate. A provisional diagnosis of a fibrosed mucocele in relation to upper and lower lip was given. Traumatic fibroma, lipoma and benign minor salivary gland tumour were considered as differential diagnosis.
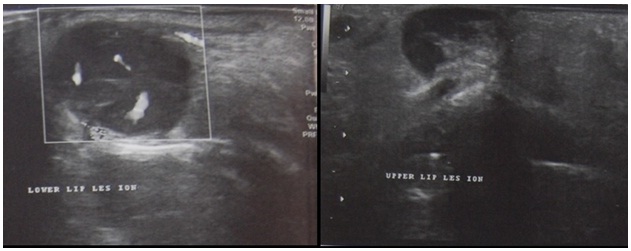
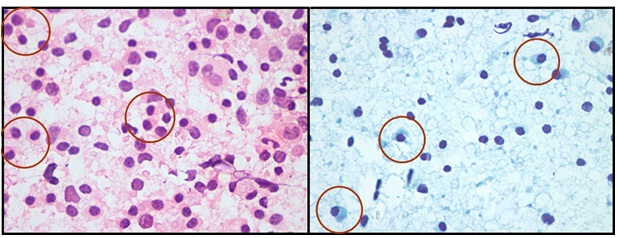
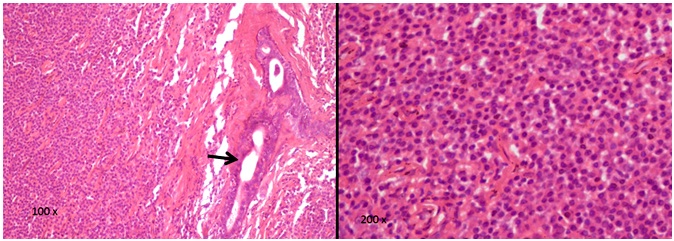
Diascopic examination of swelling of upper lip was performed, to rule out a vascular lesion. Blood investigations revealed that all the parameters were within normal limits, except for Erythrocyte Sedimentation Ratio (ESR), which was found to be 82mm/hr. Ultrasonography of upper and lower lips revealed hypoechoic lesions with minimum vascularity [Table/Fig-3] . Fine Needle Aspiration Cytology revealed a smear which comprised of lymphoid and plasmacytoid cells in a proteinaceous background [Table/Fig-4] . It was decided to excise the lesions, as they were found to interfere with patient’s dentures. Sections from the lesions, which were stained with Haematoxylin and Eosin, revealed dense monotonous sheets of lymphoid cell infiltration with loss of salivary acinar architecture and few retained ducts which were a characteristic feature of labial minor salivary glands of patients who were affected by SS [Table/Fig-5] . Hence, a further work up for Sjogren’s syndrome was performed. Antinuclear Antibody (ANA) profile [Table/Fig-6] and Rheumatoid factor (RF) assessments were done. Strong positivity for SSA, SSB and Ro 52 antigens were found. Positivity for RF, Schirmer’s tear test with a wetness score of <3 mm for eyes and xerostomia with an unstimulated salivary flow rate of 0.3 ml/ 15 minutes were suggestive of secondary Sjogren’s syndrome, according to the International Consensus Criteria for Sjogren’s syndrome. Thus, swellings which clinically resembled mucocele turned out to be lymphomas, which in turn, led us to the diagnosis of secondary Sjogren’s syndrome.
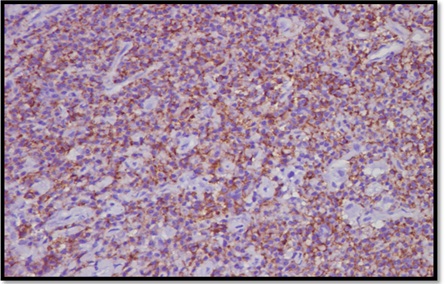
Immunohistochemistry was done for the exact typing of the lymphoid lesion. The lymphoid cells were immunohistochemically reactive to CD20+, CD3+ (focal positivity), CD138+, Bcl-2+ (positive in scattered cells), CD56-, CD10- and Ki67 (<10%), which thus confirmed the diagnosis of Non-Hodgkin’s lymphoma. [Table/Fig-7] . In view of positivity to CD 20 and strong positivity to CD 138 (plasmacytoid differentiation), a tentative diagnosis of an extranodal, marginal zone, B-cell lymphoma was given. A multidisciplinary approach, including medical oncologist, radio oncologist, and rheumatologist, was undertaken. Chest X- ray, USG of abdomen, endoscopy, were advised, followed by PET scan, to rule out any dissemined disease. After it was confirmed as an isolated NHL; a primary extranodal variant with no dissemination elsewhere in the body, it was decided to not instigate any further treatment in this patient, taking into consideration the patient’s quality of life and psychological well being. The patient has been kept under close observation and clinically, patient is in good health.
Swelling in the lower lip

Swelling in the upper lip

Ultrasonography of upper and lower lip swellings showing hypoechoic lesions with minimum vascularity
Fine Needle Aspiration Cytology showing lymphoid cells and plasmacytoid cells (encircled ) in a proteinaceous background
H& E stained sections under 100X ( arrow indicates minor salivary gland duct) and 200X showing sheets of monotonous lymphoid cells
ANA profile report showing strong positivity for antibodies to SS-A , Ro-52 and SS-B antigens Sample dilution 1:101
| Antigen | Antibody Positive/ Negative | Intensity |
| RNP/Sm | Negative | 0 |
| Sm | Negative | 0 |
| SS-A | Strong positive | +++ |
| Ro-52 | Strong positive | +++ |
| SS-B | Strong positive | +++ |
| Scl-70 | Negative | 0 |
| PM-Scl | Negative | 0 |
| Jo-1 | Negative | 0 |
| Centromere B | Negative | 0 |
| PCNA | Negative | 0 |
| dsDNA | Negative | 0 |
| Nucleosomes | Borderline | (+) |
| Histones | Borderline | (+) |
| Ribosomal-P-Protein | Negative | 0 |
| AMA-M2 | Negative | 0 |
| Control | Positive | +++ |
Immunohistochemistry showing CD 138 positivity indicating plasmacytoid differentiation
Discussion
Most lymphomas affecting the head and neck region are NHLs of B cell lineage[1] . Only 2 % of primary extranodal NHLs occur in the oral cavity [1] . The risk of lymphomas developing in patients with SS has been estimated to be 44 times more as compared to that seen in normal population[2] . The trigger factors for SS have been associated with genetic, environmental and hormonal factors, which in turn, induce immune dysregulation and loss of tolerance.
The incidences of lymphomas seen in various studies done in patients with SS, have been found to be 4.3% and 5-10 % [3] . Lymphoid proliferation of the salivary glands include a spectrum of disorders which range from an indolent benign myoepithelial/ lymphoepithelial sialadenitis (MESA) to overt low and high grade B cell lymphoma (MALT) [4] . Most cases of non-Hodgkin’s lymphomas which arise in salivary glands are of B-cell lineage, including low-grade B-cell lymphomas of mucosa-associated lymphoid tissue (MALT), which are also called as extranodal marginal zone B-cell lymphoma, diffuse large B-cell lymphomas and follicular lymphomas [5] . Other types of lymphomas have also been reported in SS, which include immunoblastic, lymphoplasmacytic and centroblastic/centrocytic lymphomas [2] . Localized NHLs of the head and neck are treated with radiotherapy alone or in combination with chemotherapy [6] .Surgery is used mainly to establish the diagnosis or for the removal of localized small lesions.
In a population based review which was conducted by Epstein et al., of 361 cases of malignant lymphomas which affected oral cavity, which were identified in the Tumour Registry between 1969 and 1998, the occurrence of malignant lymphoma by site was found to be 3 cases in lip region [7] . Sunaba et al., Yin et al., and Leong et al., have reported 1 case each with lip involvement in their studies [8-10] . In another study which was conducted by Padhi et al., in Indian population, a 5 year retrospective analysis done of 68 cases with primary extranodal lymphomas revealed only 2 patients with oral cavity involvement [11] .
Reports on MALT lymphomas in salivary glands of patients with SS are relatively less, with vast majority involving parotid and submaxillary glands, and a very rare involvement of labial minor salivary glands. Speight et al., reported 4 cases and van Mello et al., reported 3 cases of MALT lymphomas (1 case with preexisting lymphoma) in lower labial mucosa in patients with Sjogren’s syndrome [12,13] . None of these cases which were reported in SS patients with MALT lymphomas in labial mucosa presented as lip swellings and all of them were diagnosed after undergoing minor salivary gland biopsies.
In this case, nontender swellings in upper and lower lips, which mimicked fibrosed mucoceles, would have been misdiagnosed, lest a thorough systematic investigation was not performed. Hence, asymptomatic swellings seen in the orofacial region should be screened for underlying systemic diseases and biopsied, and if still in doubt, immunohistochemistry must be performed. Also, the cause of xerostomia in elderly patients, especially females who are on medications for various diseases, should not be ignored and underdiagnosed, unless Sjogren’s syndrome is ruled out, the reason being that xerostomia may not be a major complaint in all of the cases, unless it is elicited during history recording.
Conclusion
Only limited literature is available on cases with primary extranodal variants of lymphoma which occur in two different places in the lips, as was seen in our case. As oral diagnosticians, we play a very important role in early diagnosis and treatment of oral lesions. Hence, it is imperative to evaluate every simple looking lesion, as they may be indistinguishable from lesions which are life threatening.
[1]. GH Shah, SK Panwar, PP Chaturvedi, SN Kane, Isolated primary extranodal lymphoma of the oral cavity: a series of 15 cases and review of literature from a tertiary care center in India.Ind J Med Paed Onco. 2011 32(2):76-81. [Google Scholar]
[2]. RC Jordan, PM Speight, Lymphoma in Sjögren’s syndrome: From histopathology to molecular pathologyOral Surg Oral Med Oral Pathol Oral Radiol, Endo 1996 81(3):308-20. [Google Scholar]
[3]. A Keszler, LI Adler, MS Gandolfo, PA Masquijo Bisio, AC Smith, Vollenweider CF, et al. MALT lymphoma in labial salivary gland biopsy from Sjögren syndrome: importance of follow-up in early detectionOral Surg Oral Med Oral Pathol Oral Radiol 2013 115(3):e28-33. [Google Scholar]
[4]. PG Quintana, SB Kapadia, DW Bahler, JT Johnson, SH Swerdlow, Salivary gland lymphoid infiltrates associated with lymphoepithelial lesions: a clinicopathologic, immunophenotypic, and genotypic studyHum Pathol 1997 28(7):850-61. [Google Scholar]
[5]. A Faur, E Lazar, M Cornianu, A Dema, C Lazureanu, A Muresan, Primary malignant non-Hodgkin’s lymphomas of salivary glands.Rom J Morphol Embryol. 2009 50(4):693-9. [Google Scholar]
[6]. CD Ruijs, AW Dekker, ML van Kempen-Harteveld, J van Baarlen, GJ Hordijk, Treatment of localized non-Hodgkin’s lymphomas of the head and neck.Treatment of localized non-Hodgkin’s lymphomas of the head and neck. 1994 74(2):703-7. [Google Scholar]
[7]. JB Epstein, JD Epstein, ND Le, M Gorsky, Characteristics of oral and paraoral malignant lymphoma: a population-based review of 361 casesOral Pathol Oral Radiol Endod. 2001 Nov 92(5):519-25. [Google Scholar]
[8]. K Sunaba, H Shibuya, N Okada, T Amagasa, S Enomoto, S Kishimoto, Radiotherapy for primary localized (stage I and II) non-Hodgkin’s lymphoma of the oral cavityInt J Radiat Oncol Biol Phys. 2000 47:179-83. [Google Scholar]
[9]. H Yin, N Okada, M Takagi, Comparison of apoptosis and apoptosis-related gene products between extranodal oral B-cell lymphoma and maxillofacial nodal B-cell lymphoma.J Oral Pathol Med 2001 30:141-47. [Google Scholar]
[10]. IT Leong, BJ Fernandes, D Mock, Epstein-Barr virus detection in non-Hodgkin’s lymphoma of the oral cavity: an immunocytochemical and in situ hybridization study.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001 92:184-93. [Google Scholar]
[11]. S Padhi, TR Paul, S Challa, AK Prayaga, S Rajappa, D Raghunadharao, Primary extra nodal non Hodgkin lymphoma: a 5 year retrospective analysisAsian Pac J Cancer Prev 2012 13(10):4889-95. [Google Scholar]
[12]. PM Speight, R Jordan, P Colloby, H Nandha, JH Pringle, Early detection of lymphomas in Sjögren’s syndrome by in situ hybridization for kappa and lambda light chain mRNA in labial salivary glands.Eur J Cancer B Oral Oncol. 1994 30B:244-7. [Google Scholar]
[13]. NM Van Mello, SR Pillemer, PP Tak, V.B Sankar, Cell MALT lymphoma diagnosed by labial minor salivary gland biopsy in patients screened for Sjögren’s syndrome.Ann Rheum Dis. 2005 64:471-3. [Google Scholar]