Endodontic Management of a Mandibular Central Incisor with Type IV Canal Pattern: A Case Report
Sunandan Mittal1, Tarun Kumar2, Jyotika Sharma3, Shifali Mittal4, Tarun Ahuja5
1Professor and Head, Department of Conservative Dentistry and Endodontics, Dasmesh Institute of Research and Dental Sciences, Faridkot, Punjab, India.
2Professor, Department of Conservative Dentistry and Endodontics, Dasmesh Institute of Research and Dental Sciences, Faridkot, Punjab, India.
3Post Graduate Student, Department of Conservative Dentistry and Endodontics, Dasmesh Institute of Research and Dental Sciences, Faridkot, Punjab, India.
4Post Graduate Student, Department of Conservative Dentistry and Endodontics, Dasmesh Institute of Research and Dental Sciences, Faridkot, Punjab, India.
5Professor and Head, Maharana Pratap Dental College, Department of Conservative Dentistry and Endodontics, Gwalior, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sunandan Mittal, Dasmesh Institute of Research and Dental Sciences, Faridkot – Punjab, India.
Phone: 91-1636-223983, +91-9814049751,
E-mail: dr.sunandanmittal@yahoo.in
The success of endodontic treatment requires the knowledge of tooth morphology and its variations. Mandibular incisor’s anatomy presents a challenge when an endodontic access is made, because of its small size and high prevalence of two canals. We are describing a Weine’s Type IV root canal configuration that was detected in a mandibular central incisor, which was demonstrated by a radiographic examination. This article also focuses on the successful endodontic treatment of a mandibular central incisor with a single canal at the pulp chamber, which divided into two distinct and separate canals (buccolingual) at the middle third of the root.
Mandibular incisors, Type IV canal pattern, Endodontic treatment
Case Report
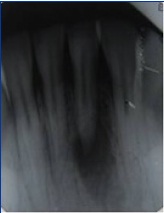
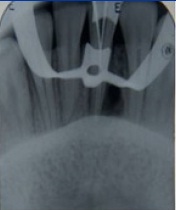
A 19-year-old male patient reported to the Department of Conservative Dentistry and Endodontics with dull pain and pus discharge in the front lower left tooth region, of one month’s duration. The medical history was non-contributory, but the patient had experienced a traumatic injury to the anterior mandibular region about eight years back, and there was a history of periodic tooth discomfort on biting. The clinical examination revealed dull pain on percussion wrt (with respect to) #31, pus discharge from the sinus which was below 31 and no response to thermal sensitivity tests #31. 32 and 41 responded normally to thermal sensitivity tests. A pre-operative radiographic examination revealed a large periapical radiolucent area wrt #31 [Table/Fig-1]. The left mandibular central incisor (31) showed a radiolucent canal that stopped abruptly in the middle third of the root, which indicated a multicanal morphology. Some amount of horizontal bone loss was seen in the whole anterior teeth region, but clinically, no mobility was seen. The diagnosis which was made was a ‘Chronic Periapical Abscess’. An endodontic treatment was indicated. The periodontal prognosis of the tooth was estimated to be good. An access opening was made and a lot of pus discharge was encountered. Hence, an open dressing was given and the patient was recalled after 2 days. At this visit, a careful exploration of the canal orifice and root canal revealed Weine’s Type IV morphology of root canals, i.e one canal left the chamber and divided into two separate and distinct canals (buccolingually, in this case). The working length was estimated by using an apex locator and it was also confirmed radiographically, to determine the anatomic relationship of the root canal of 31 [Table/Fig-2]. The biomechanical preparation of 31 was done and the tooth was given closed dressing with calcium hydroxide.
In such a type of canal variation, generally, preferred technique of obturation is thermoplasticized gutta percha. But in this case, it was decided to perform a lateral condensation technique, because the pulp chamber was wide and negotiation of both the canals was possible. After a week, the tooth was obturated with gutta percha and endomethasone by using a lateral condensation technique [Table/Fig-3,4]. After six months of follow up, radiographs showed the initiation of healing of periapical lesion [Table/Fig-5]. Hence, a surgical intervention was not considered this time, as the patient was asymptomatic.
Discussion
One of the main goals of a nonsurgical, endodontic treatment is the elimination of infections from root canal system and prevention of its reinfection. For obtaining consistently high levels of success in endodontic treatment an understanding of root canal morphology is required. Thus, it is necessary for clinicians to have knowledge, not only on the dental anatomy of teeth, but also on its variations [1].
It is generally accepted that many mandibular incisors have 2 canals, which may merge into 1 canal before reaching the apex [2-5]. In rare cases, separate foramina may form. In a radiographic study done on 364 specimens, Benjamin and Dowson [5] reported that 41.4% of the mandibular incisors that they studied had 2 separate canals; among these, only 1.3% had 2 separate foramina. In a study done on 1,085 specimens, Miyashita et al., [6] reported that only 3.1% of the samples had separate canals and foramina. In a study done on mandibular incisors, in which a surgical resection method was used to study canal anatomy, Mauger et al., [7] demonstrated that, at the apical 1, 2 and 3 mm levels in the mandibular incisor, the canal was only rarely separated by hard tooth structure and that only 2% of the teeth that they studied had 2 canals at the 1 mm resection level.
The anatomy and morphology of root canal system is complex and the detection of the presence of extra root or root canals dictates the success in endodontic therapy. Undetected canals are the major cause for failure of this treatment [8]. Incomplete removal of all the irritants from the pulp space may increase the possibility of treatment failure [8,9]. According to the endodontic literature, mandibular incisors with two canals are not unusual [2-5]. In most of the cases with two root canals, they merge into a single canal which is short of the apex. According to Weine’s classification, the canals can be classified as:-
Type I- A single canal from the pulp chamber to apex.
Type II- Two canals leaving from the chamber and merging to form a single canal which is short of the apex.
Type III- Two separate and distinct canals from chamber to the apex.
Type IV- One canal leaving the chamber and dividing into two separate and distinct canals.
A careful interpretation of the radiographic features is essential to ensure that the additional root canals are not overlooked. This may necessitate imaging the tooth from different angles, so that the multiple root canals may be distinguished. Nevertheless, manual exploration of the root canal system with an endodontic file or an explorer is a reliable method for identifying the exact configuration of the root canal, especially the number of foramina.
Achieving endodontic success in teeth with a number of canals above that which are normally found, requires a correct diagnosis and a careful clinical radiographic inspection. Morphological variations in pulpal anatomy must be considered before onset of treatment [10].
The most commonly used obturation technique for filling such a type of canal anatomy is thermoplasticized gutta percha. In this case, lateral condensation obturation was performed, because the pulp chamber was wide and negotiation of both the canals was possible.
Working length radiograph
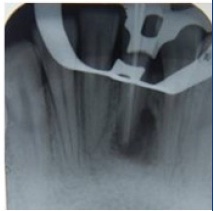
Post-obturation radiograph

6 months follow-up radiograph

Conclusion
Root canal anatomy of mandibular incisors shows a high incidence of complexity, which includes variations in canal configuration, number of canals and presence of an isthmus. A thorough knowledge on root canal anatomy and morphology, proper interpretation of the radiographs, are important for recognizing and treating such cases.
[1]. F Baratto–Filho, LF Fariniuk, EL Ferreira, JD Pecora, AM Cruz–Filho, MD Sousa–Neto, Clinical and macroscopic study of maxillary molars with two palatal roots.Int Endod J. 2002 35(9):796-801. [Google Scholar]
[2]. FJ Vertucci, Root canal anatomy of the mandibular anterior teeth.J Am Dent Assoc. 1974 89(2):369-71. [Google Scholar]
[3]. R Bellizzi, G Hartwell, Clinical investigation of in vivo endodontically treated mandibular anterior teeth.J Endod. 1983 9(6):246-8. [Google Scholar]
[4]. RW Rankine-Willson, P Henry, NH Olsen, JJ Hefferren, The bifurcated root canals in lower anterior teeth.J Am Dent J Am Dent Assoc. 1965 70:1162-5. [Google Scholar]
[5]. KA Benjamin, J Dowson, Incidence of two root canals in human mandibular incisor teeth.Oral Surg Oral Med Oral Pathol. 1974 38(1):122-6. [Google Scholar]
[6]. M Miyashita, E Kasahara, E Yasuda, A Yamamoto, T Sekizawa, Root canal system of the mandibular incisor.J Endod. 1997 23(8):479-84. [Google Scholar]
[7]. MJ Mauger, WG Schindler, 3rd Walker WA, An evaluation of canal morphology at different levels of root resection in mandibular incisors.J Endod. 1998 24(9):607-9. [Google Scholar]
[8]. RR Slowey, Radiographic aids in detection of extra root canals.Oral Surg Oral Med Oral Pathol. 1974 37:762-71. [Google Scholar]
[9]. R Nair, U Sjogren, G Kreg, KE Khanberg, G Sandquist, Intraradicular bacteria and fungi in root filled asymptomatic human teeth with therapy resistant periapical lesion- a long term light and electron microscope follow up study.J Endod 1990 16:580-8. [Google Scholar]
[10]. FAD Gomes, al et, Two root canals in maxillary central incisorRSBO. 2011 8(3):341-4. [Google Scholar]