Prosthetic Management of A Masticatory Muscle Disorder with Customized Occlusal Splint
Pavankumar R. Koralakunte1
1Assistant Professor, Department of Maxillofacial Prosthodontics, Bapuji Dental College and Hospital, Davangere-577004, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pavankumar R. Koralakunte Assistant Professor, Department of Maxillofacial Prosthodontics, Bapuji Dental College and Hospital, Davangere-577004, Karnataka, India.
Phone: +919886000211, Fax Number: 91-8192-220578,
E-mail:pavan_dent@yahoo.co.in
Occlusal splints of various types and designs are used in the diagnosis and treatment of different masticatory muscle and TMJ disorders. These appliances or devices provide a relatively simple, reversible and non-invasive form of treatment management. Treating such a disorder is really challenging for both dental and medical specialists and often it is difficult to diagnose as the presenting symptoms can be variable. The present article thus describes a case report on fabrication of simplified customized occlusal splint emphasizing the importance of medico-dental team approach for successful management with occlusal splint therapy.
Occlusal splint, Occlusal device, Occlusal appliance, Occlusal dysfunction, Masticatory muscle disorder, Temporomandibular joint (TMJ) disorder
Case Report
A 23-year-old female reported to the Department of Maxillofacial Prosthodontics, Bapuji Dental College and Hospital with pain on both sides of the mandibular jaw. The patient gave history of pain and headache which is severe early in the morning and that is continuous throughout the day since three months.
Investigations were carried out in Department of oral medicine and radiology under specialist intervention:
Muscle Examination Masticatory muscles such as masseter and temporalis were examined clinically by palpation method where as medial pterygoid and lateral pterygoid were examined by functional manipulation method revealing tenderness and spasm of masseter and temporalis muscles.
Pain Management Transcutaneous electric nerve stimulation (TENS) therapy for pain management was advised where the patient had temporary relief for certain period of time but later the pain recurred back due to hyperactivity of the muscles.
Radiographic ExaminationOPG, Intraoral periapical radiographs (IOPA) of entire teeth showed no evidence of any dental infection or problem.TMJ radiographs also revealed no signs of deformity of TMJ’s and its relation to glenoid fossae.
Diagnosis
On extraoral and intraoral examination, positive findings such as the tenderness of masseter muscle on both sides upon palpation, attrition of the occlusal surfaces of posterior teeth and the patient clenching her teeth repeatedly without her knowledge was noticed on observation. After ruling out, previous family and medical history of any suspected TMJ disorder such as inflammatory TMJ, deformity of articular disc, derangement of condyle etc. The case was diagnosed as masticatory muscle disorder presenting with myospasm and myofascial pain due to parafunctional habit of constantly clenching her teeth due to her occupational work related stress.
A treatment plan was formulated for fabrication of maxillary occlusal splint to meet the need of the patient for decreasing the hyperactivity of masticatory muscles. The treatment procedure was explained in detail to the patient along with a signed consent form approved by the institutional ethical committee on human research.
Procedure
Clinical Steps 1:An impression of both the maxillary and mandibular arches were made with irreversible hydrocolloid material and poured with type III dental stone to obtain diagnostic casts to be mounted using type II dental plaster in a semi adjustable articulator following a face bow transfer and centric relation bite record [1,2]. A preexisting record of centric relation and centric occlusion of the patient need to be made before treatment to avoid change in occlusion after therapy [3].
Laboratory Steps:The face bow record helps in mounting of the maxillary cast were as the centric relation bite record help in mounting of the mandibular cast in relation to the maxillary cast in the articulator [Table/Fig-1] . This relates exactly to that of the patient’s existing jaw occlusion relation. After mounting, the maxillary cast was detached from the articulator to do surveying procedure using a dental surveyor in order to determine the height of contour of the teeth and reattached back. The vertical height of the articulator with mounted casts was increased by 1mm and locked in this new incisal guide position to provide interocclusal space between the posterior teeth [2]. The undercuts were blocked out around the maxillary teeth below the survey line by adapting a continuous rope of hard wax around the arch exposing about 2mm on buccal surface and 3-4mm on palatal surface [Table/Fig-2] . The mandibular teeth were blocked out completely except the buccal centric (functional) cusp tips that protruded through the occlusal surface [Table/Fig-3] [1]. Trial check for any interference between the maxillary and mandibular blocked out wax was eliminated by closing the articulator. A layer of separating media was applied on the maxillary teeth up to the block out, followed by dispensing of self cure clear acrylic polymer-monomer slowly by sprinkle on method to get adequate thickness of the splint [Table/Fig-4] [1,4]. In between, the articulator was closed often to ensure firm seating of the incisal guide pin on the incisal guide table. Once the self cure acrylic had set, the acrylic splint was removed carefully from the maxillary cast, finished and polished in a regular manner. Rechecking of finished and polished occlusal acrylic splint was done by closing the articulator to verify whether the mandibular centric (functional) cusp tips made contact with the occlusal surface of the splint [1,2,4,5].
Clinical Step 2:Insertion of customized self cure clear acrylic maxillary occlusal splint was completed with minor intraoral adjustments [Table/Fig-5] . Post-insertion instructions were given and the follow-up visits revealed total satisfactory results with reduced symptoms in the patient. The recommended protocol after insertion of the splint is that the patient need to visit the prosthodontist for adjustments at 24 hrs, 3 days, 7 days, 14 days, 21 days and 1 month intervals [6].
The patient was educated about the condition and was instructed her to join yoga or meditation as behaviour modification therapy to decrease stress along with the use of occlusal splint.
Discussion
An occlusal splint is a removable device usually made of hard acrylic that fits over the occlusal and incisal surface of the teeth in one arch, creating precise occlusal contact with the teeth of opposing arch. It is commonly referred to as occlusal appliance, inter occlusal appliance, bite guard, night guard, intraoral orthotic, orthopaedic device, deprogrammer device [7].
In the presented article, full coverage stabilization type of occlusal splint was fabricated which was made of hard clear self cure acrylic resin. The design was made in such a way that the splint covered up to the height of contour of the teeth resulting in more esthetically pleasing and proper fit as compared to other designs that normally cover all the teeth surfaces and sometimes even marginal gingiva eventually causing irritation to the gingival tissues. Eventhough there are different designs of occlusal splint fabrication that vary according to patient’s clinical condition, the prime function of occlusal splint remains unaffected with the design [8].
Most case reports in the literature [1,2,4,5].related to various types of Temporo Mandibular Disorder management have not mentioned the importance of inter and multidisciplinary approaches where teamwork play an important role in the overall treatment success. In the presented article, the case was diagnosed and treated via interdisciplinary approach as it was a simple case of masticatory muscle disorder.
The principle on which most occlusal splints function is to alter an occlusion without interfering with complete seating of the condyles in centric relation [9]. Theories of splint action are:
Occlusal disengagement theory.
vertical dimension theory.
Maxillomandibular realignment theory.
TMJ repositioning theory.
Cognitive awareness theory [10].
The main advantage of occlusal splint therapy is that they cannot cause effects that are in violation of mechanical laws. Thus, an occlusal splint does not unload the condyles as the muscles of mastication act posterior to the splint [11].
Advantages of the technique presented in the article are:
The splint fabrication was completed within 30 minutes after diagnostic mounting in the articulator.
Ease of construction.
Minimal trimming and finishing required.
Splint can be fabricated without distortion of the cast.
Little intraoral adjustment required.
Only one set of diagnostic casts serve for both occlusal analysis and splint construction [1,12].
Diagnostic mounting on Hanau Wide Vue Articulator

Maxillary block out on buccal, palatal and interproximal aspects

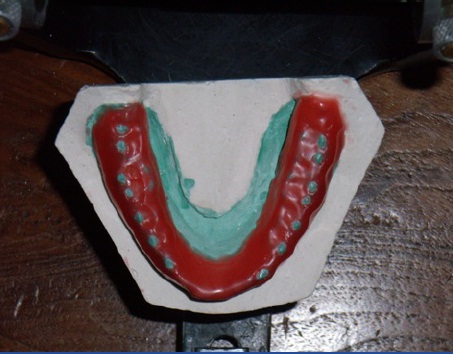
Mandibular block out covers teeth entirely except protruding buccal cusps tips
Self cure acrylic resin splint after fabrication on maxillary diagnostic cast

Final insertion of finished and polished occlusal splint in the patient

Conclusion
A proper and thorough case history, examination and diagnosis are extremely important in managing the Temporo mandibular disorder as the signs and symptoms are multifactorial. The management often involves either interdisciplinary or multidisciplinary approach depending upon the type and severity of the disorder. The occlusal splint along with pharmacotherapy and behavior modification therapy are effective in overall treatment management.
[1]. TF Lundeen, Occlusal splint fabrication.J Prosthet Dent. 1979 42:588-91. [Google Scholar]
[2]. M Choi, J Holden, F Tung, An alternative technique for fabrication of an occlusal device.J Prosthodont. 2008 17:423-26. [Google Scholar]
[3]. RJM Gray, SJ Davies, Occlusal splints and Temporomandibular disorders: Why,When, How?Dent Update. 2001 28:194-99. [Google Scholar]
[4]. CA Kass, JN Tregaskes, Occlusal splint fabrication.J Prosthet Dent. 1978 40:461-63. [Google Scholar]
[5]. JE Haddix, HO Heymann, A simplified technique for occlusal splint fabrication.J Prosthet Dent. 1987 57:249-51. [Google Scholar]
[6]. TJ Dylina, The basics of occlusal splint therapy.Dent Today. 2002 15:82-87. [Google Scholar]
[7]. JP Okeson, JP. Occlusal appliance therapy. Management of temporomandibular disorders and occlusion. Mosby Elsevier. 2008 6th Edition:468-522. [Google Scholar]
[8]. A Jokstad, A Mo, BS Krogstad, Clinical comparison between two different splint designs for temporomandibular disorder therapy.Acta Odontol Scand. 2005 63:218-26. [Google Scholar]
[9]. PE Dawson, Occlusal splints. Functional Occlusion – From TMJ to smile design.Mosby Elsevier. 2007 52:379-92. [Google Scholar]
[10]. GT Clark, PJ Sheridan, A critical evaluation of orthopedic interocclusal appliance therapy: design, theory, and overall effectiveness.J Am Dent Assoc. 1984 108:359-64. [Google Scholar]
[11]. RG Despande, S Mhatre, TMJ disorders and occlusal splint therapy –A Review.International Journal of dental Clinics. 2010 2:22-29. [Google Scholar]
[12]. HF Adams, Fabrication of a maxillary occlusal treatment splintJ Prosthet Dent. 1979 42:106-11. [Google Scholar]