Ehlers Danlos syndrome (EDS) is a hereditary collagen disorder which primarily manifests in the skin and joints. Clinically, it is characterized by hyperelasticity of skin and joint hypermobility. This article has described a rare condition seen in a 10-year-old boy who was diagnosed with EDS, based on the clinical, radiographic and histological findings.
Case Report
A 10-year-old boy reported to our college with chief complaint of inability in chewing caused by missing teeth since past 2 years. The patient presented with missing deciduous teeth, and he reported premature exfoliation of posterior deciduous teeth within five years, except primary canines. The primary concern was of unerupted permanent teeth, except for the first permanent molars, which displayed delayed eruption. Medical history revealed cerebral fever (at age of 4 years) and hernia 15 days post birth. The family history revealed that the patient’s paternal grandfather had highly flexible joints. However, nothing extraordinary was reported / recalled, with respect to any of the existing and deceased family members. Considering the little family information which was available, no conclusions could be drawn to ascertain any genetic pattern.
Extraoral examination revealed:
A mesomorphic body structure with a dolichocephalic head.
A leproprosopic face with orbital hypertelorism.
A wide nasal bridge with a depressed bulb of nose and stretched external nares.
The skin over the extremities was loose and easily stretchable.
The patient appeared to be shy and non-conversant, especially because of his unaesthetic appearance.
The patient’s score was eight on the Beighton scale (scores which are ≥ than 5 describe hypermobility) as was assessed by the joint mobility test which was suggested by Beighton et al., by using a protractor [1], [Table/Fig-1,2and3].
Intraoral examination and evaluation revealed
Macroglossia.
Positive Gorlin’s sign [Table/Fig-4].
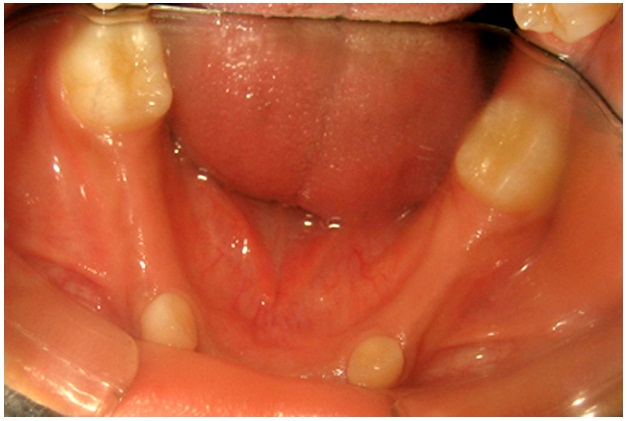
The edentulous gingiva appeared to be comparatively thick and fibrous.
Teeth which were present in the oral cavity were 16, 26, 36, 46, 53, 63, 73 and 83.
Grade II mobile 53, 63, 73, 83 [Table/Fig-5,6].
A noticeable loss of vertical dimension
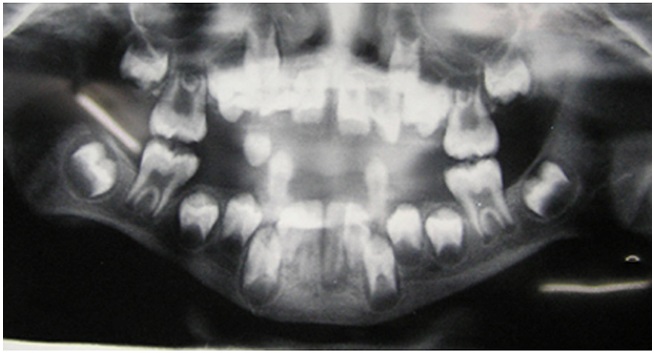
A maxillary occlusal radiograph was taken to rule out the presence of any supernumerary teeth. An orthopantomograph (OPG) revealed the presence of all the remaining unerupted permanent teeth [Table/Fig-7].
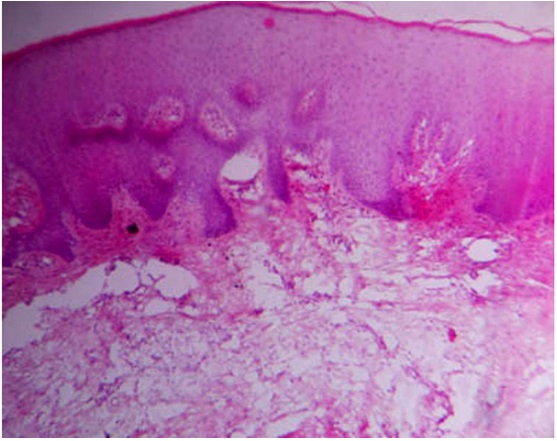
Biopsies of the gingival tissues which overlay the unerupted 13, 12, 11, 21, 22, 23 were obtained and they were sent for a histopathologic examination. The histological sections of the tissues were stained with Haematoxylin and Eosin, which showed hyperplastic keratinized epithelium with dense, fibrotic connective tissue, with numerous plump fibroblasts and blood vessels [Table/Fig-8].
On the basis of the classic clinical and histopathologic findings, the patient was diagnosed with Ehlers Danlos Syndrome Type III [Table/Fig-9] , [1].
A treatment plan was formed and it consisted of a) Extraction of the deciduous teeth b) Use of a removable partial denture prosthesis (RPD) for restoring form, function and aesthetics subsequently [Table/Fig-10].
Discussion
Ehlers Danlos syndrome is a rare connective tissue syndrome that mainly affects the skin and the joints. EDS is a rare type of disorder of the connective tissue that affects the collagen metabolism in which deficiency and /or disordered deposition of collagen takes place [2]. One of the first descriptions given was of a young Spaniard who could stretch the skin which overlay his right pectoral muscle, over to the left angle of his mandible [3]. The skin and joint manifestations of this syndrome have been studied; however, only little emphasis has been laid on the oral manifestations of this syndrome [4-6].
Pommeau-Delille and Soussie christened this condition as Ehlers-Danlos syndrome [7]. Ehlers, first described this syndrome as one with hyperplastic skin and a strong tendency to get bruised. Danlos, found a pseudo-tumour of a molluscoid or fibrous type. This syndrome affects [1] in 5,000 people [8], it is inherited as an autosomal dominant trait and it may also be associated with X chromosome [2]. Depending on which type of collagen is affected, the disorder has a wide range of expressivity [9] and there are many phenotypes. A new classification which was based on cause wasdeveloped, which described 6 types of EDS [9].
Out of the known six types, only 4 types of EDS, namely types IV, VI, VII and X can be confirmed by doing biochemical and molecular tests [7]. As 19 types of collagen are found in the human body, it is especially difficult to establish a precise diagnosis [10]. Despite bleeding disorders being associated with EDS, blood investigations are not of much diagnostic value, as no correlation has been found between the findings and the various types of EDS [7]. A few of the EDS types can be confirmed by genetic testing, after the clinical criteria are met. However, many cases may still remain ambiguous and they do not fit in any of the well-described subtypes [11].
The characteristic features [7-9] of this syndrome are
Hypermobility of the joints.
Hyperelasticity, fragility and softness of the skin.
Deficient healing of wounds.
Ecchymosis caused by minor traumas.
Besides the cutaneous and articular anomalies, the patients may show cardiovascular complications (such as aneurysms and mitral valve prolapse), gastrointestinal complications (hernias and gastrointestinal diverticulosis), and ocular defects [2].
The oral manifestations of EDS include the following:
The mucous membrane is fragile, which may bleed on instrumentation and which sutures cannot hold [7].
Dentinal aberrations like pulp stones, short and deformed roots.
A high incidence of caries in the deciduous teeth [9].
Spontaneous fractures of teeth have been reported.
Early onset of generalized periodontitis is one of the most significant oral manifestations of the syndrome [1,12].
Hyperelasticity, fragility and softness of the skin.
A supple tongue. Approximately 50% of those with this syndrome can touch the end of their noses with their tongue (Gorlin’s sign), as compared to 8-10% in the normal population who can do this [7].
Hyper mobility of the TMJ, with increased incidence of dysfunction may be seen in some cases.
In this patient, the connective tissue hyperplasia which was manifested in the gingiva, resulted in its thickening, which must have prevented the eruption of the permanent teeth and resulted in the chief complaint of the patient. The classic clinical findings, along with histopathologic findings, confirmed the diagnosis. The removal of the deciduous teeth prematurely, was primarily guided by the unusual mobility which presented and the prosthodontic rehabilitation of the patient was aimed at rapidly addressing the chief complaint. The patient was periodically recalled for two years for the post insertion adjustments of the prosthesis. The permanent teeth did not show any signs of erruption during this period of follow up.
Beighton’s Scale for Assessment of Joint Hypermobility
| S.No. | Characteristic | Maximum Score |
| 1 | Passive dorsiflexion of each little finger beyond 90 ° | 02 (01 for each side) |
| 2 | Passive apposition of each thumb to the flexor aspect of the forearm. | 02 (01 for each side) |
| 3 | Hyperextension of each elbow beyond 10° | 02 (01 for each side) |
| 4 | Hyperextension of each knee beyond 10° | 02 (01 for each side) |
| 5 | Forward flexion of the trunk, with knees straight, so that the palms of the hands rested easily on the floor. | 01 |
Patient showing Gorlin’s sign positive

Hypermobility of little finger - positive

Hypermobility of knees - positive

Intraoral photograph of the maxillary arch (one week post extraction of 53 and 63)

Intraoral photograph of the mandibular arch showing presence of 36, 46, 73 and 83
OPG of the patient showing multiple impacted permanent teeth
Histopathologic appearance of the gingival tissues showing hyperkeratinised epithelium along with dense connective tissue
Removable partial denture inserted into the patient

Classification of EDS Types
| Type | Clinical Characteristics |
| I and II (Classic) | Marked skin hyperextensibility, widened atrophic scars and joint hypermobility. Molluscoid pseudo tumours (calcified haematomas) and periodontitis has been reported. |
| III (Hypermobility Type) | Joint hypermobility is the dominant clinical manifestation. The hyperextensibility and/or smooth velvety skin and bruising tendencies are present but variable in severity. Periodontitis has been reported. |
| IV (Vascular Type) | The skin is thin and translucent with visible veins. The facial characteristics are large eyes, thin nose, lobeless ears, short stature, thin scalp hair and also evident is a decrease in subcutaneous tissue of face and extremities. Easy bruising manifested by spontaneous ecchymosis. Arterial / intestinal / uterine fragility or ruptures are common. |
| V | It has been described in a single family, is a rare variant and the molecular basis remains unknown. |
| VI (Kyphoscoliosis Type) | Generalized joint laxity, severe muscle hypotonia and scoliosis at birth. Tissue fragility, atrophic scars, easy bruising and marfanoid habitus (Marfan-like features), micro cornea and radiologically considerable osteopenia. |
| VII A and B (Arthrochalasia Type) | Congenital hip dislocation, generalized joint hypermobility with recurrent subluxations, skin hyperextensibility with easy bruising, tissue fragility including atrophic scars; muscle hypotonia; kyphoscoliosis and radiologically mild osteopenia. |
| VII C (Dermatosparaxis Type) | Severe skin fragility and substantial bruising. Normal wound healing and the scars formation. Skin texture is soft and doughy. The redundancy of facial skin results in an appearance resembling cutis laxa. Large hernias (umbilical, inguinal) may be seen. The oral findings are alterations on the teeth and severe periodontitis. |
| VIII | Similar to the classical type except that it also presents periodontal friability. This is a rare type of EDS and its existence as an autonomous entity is uncertain. |
Conclusion
Ehlers-Danlos Syndrome is an autosomal dominant hereditary connective tissue disorder with skin and joint manifestations. This condition is also known to have oral manifestations that clinicians must be aware of, for making correct diagnoses of such patients and for proper treatment planning.
[1]. C Badauy, S Gomes, M Filho, J Chies, Ehlers-Danlos Syndrome (EDS) type IV.Review of the literatureClin Oral Invest 2007 11:183-7. [Google Scholar]
[2]. O Ferreira, A Capelozza, R Yaedú, A Costa, Odontogenic keratocyst and multiple supernumerary teeth in patients with Ehler- Danlos syndrome – A case report and review of the literature.Quintessence Int. 2008 39:251-256. [Google Scholar]
[3]. Fm Pope, Ehlers-Danlos syndrome.Baillieres Clin Rheumatol. 1991 5:321-49. [Google Scholar]
[4]. RR Welbury, Ehlers-Danlos syndrome: historical review, report of two cases in one family and treatment needs.ASDC J Dent Child. 1989 56:220-4. [Google Scholar]
[5]. T Ooshima, K Abe, H Kohno, A Izumanitani, Oral manifestations of Ehlers-Danlos syndrome type VII: histological examination of a primary tooth.Pediatr Dent. 1990 12:102-6. [Google Scholar]
[6]. S Reichert, D Riemann, B Palschka, HK Machulla, Early onset periodontitis in a patient with Ehlers-Danlos syndrome type III.Quintessence Int. 1999 30:785-90. [Google Scholar]
[7]. Létourneau Pérusse Buithieu Oral manifestations of Ehler Dunlos Syndrome.J Can Dent Assoc. 2001 67:330-4. [Google Scholar]
[8]. C Hagberg, B Burglund, L Korpe, J Norender, Ehlers–Danlos Syndrome (EDS) focusing on oral symptoms: a questionnaire study.Orthod Craniofacial Res. 2004 7:178-85. [Google Scholar]
[9]. G Klingberg, C Hagberg, J Noren, S Nietzsche, Aspects on dental hard tissues in primary teeth from patients with Ehlers–Danlos syndrome.International Journal of Paediatric Dentistry. 2009 19:282-90. [Google Scholar]
[10]. KI Kivirikko, Collagens and their abnormalities in a wide spectrum of diseases.Ann Med. 1993 25:113-26. [Google Scholar]
[11]. A Karaa, J Stoler, Case Report, Ehlers Danlos Syndrome: an unusual presentation you need to know about.Case Rep Pediatr. 2013 52:764-59. [Google Scholar]
[12]. Jr Hartsfield JK, BG Kousseff, J Noren, S Nietzsche, Phenotypic overlap of Ehlers-Danlos syndrome type IV and VIII.Am J Med Genet 1990 37:465-70. [Google Scholar]