Comparative Evaluation of Marginal Adaptation of BiodentineTM and Other Commonly Used Root End Filling Materials-An Invitro Study
Ravichandra P.V.1, Harikumar Vemisetty2, Deepthi K.3, Jayaprada Reddy S4, Ramkiran D.5, Jaya Nagendra Krishna M.6, Gita Malathi7
1 Professor and HOD, Department of Conservative Dentistry and Endodontics, Kamineni Institute of Dental Sciences, India.
2 Professor, Department of Conservative Dentistry and Endodontics, Kamineni Institute of Dental Sciences, India.
3 Consulting Endodontist, Vasan Dental Care, India.
4 Professor, Department of Conservative Dentistry and Endodontics, Kamineni Institute of Dental Sciences, India.
5 Senior Lecturer, Department of Conservative Dentistry and Endodontics, Kamineni Institute of Dental Sciences, India.
6 Reader, Department of Conservative Dentistry and Endodontics, Kamineni Institute of Dental Sciences, India.
7 Senior Lecturer, Department of Periodontics, S.V.S Institute of Dental Sciences, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. P.V. Ravi Chandra, Professor and HOD, Department of Conservative Dentistry and Endodontics, Kamineni Institute of Dental Sciences, Sreepuram, Narketpally, Nalgonda, Andhra Pradesh - 508254, India.
Phone: 09849030977,
E-mail: Kamineni.endodontics@gmail.com
Aim: The purpose of this investigation was to evaluate the marginal adaptation of three root-end filling materials Glass ionomer cement, Mineral trioxide aggregate and BiodentineTM.
Methodology: Thirty human single-rooted teeth were resected 3 mm from the apex. Root-end cavities were then prepared using an ultrasonic tip and filled with one of the following materials Glass ionomer cement (GIC), Mineral trioxide aggregate (MTA) and a bioactive cement BiodentineTM. The apical portions of the roots were then sectioned to obtain three 1 mm thick transversal sections. Confocal laser scanning microscopy (CLSM) was used to determine area of gaps and adaptation of the root-end filling materials with the dentin. The Post hoc test, a multiple comparison test was used for statistical data analysis.
Results: Statistical analysis showed lowest marginal gaps (11143.42±967.753m2) and good marginal adaptation with BiodentineTM followed by MTA (22300.97±3068.883m2) and highest marginal gaps with GIC (33388.17±12155.903m2) which were statistically significant (p<0.0001).
Conclusion: A new root end filling material BiodentineTM showed better marginal adaptation than commonly used root end filling materials
Bioactive cement, Confocal laser scanning microscopy, Glass Ionomer cement, Marginal adaptation, Mineral trioxide aggregate
Introduction
The changing concepts in surgical techniques along with newer inventions in equipment, and materials made endodontic surgery a predictable treatment option in cases that have not responded to initial endodontic therapy or when nonsurgical root canal therapy may not be successful. This procedure consists of resecting the apical 3 mm followed by placement of a root end filling material after exposing the root apex of involved tooth [1,2].
The primary objective of root-end fillings is to seal the apical region to avoid bacterial infiltration or their products from the periradicular tissues to root canal system. Johnson explained the potential relation between long-term clinical success and three critical properties for selecting an ideal root-end filling material, namely, biocompatibility, apical sealability, and their physical properties [3].
Despite wide use of Amalgam as a root-end filling material, it has certain drawbacks like non-adhesiveness, microleakage and mercury [4]. This lead to development of several other materials which include modified Zinc oxide eugenol-based cements (Super-EBA® & IRM), Glass ionomer cements (GIC), Calcium hydroxide cements, Gutta-percha, Composite resins and more recently, Mineral trioxide aggregate (MTA). New experimental Ca3SiO5-based restorative cement is introduced into the market under the name of BiodentineTM (Septodont, Saint-Maur-des-Fosses, France) similar to Mineral trioxide aggregate [5,6]. The main component of the powder is a tricalcium silicate, with the addition to the powder of CaCO3 and ZrO2. The liquid is a solution of CaCl2 with a water reducing agent.
Current methods to evaluate the efficacy of apical seal and the degree of adaptation are dye penetration, radioisotopes, bacterial penetration, Scanning electron and Confocal Laser Scanning Microscopy, Electrochemical means and Fluid filtration techniques [7].
In the present study Confocal Laser Scanning Microscopy (CLSM) has been used to analyze the interface between dentin and root-end filling material and to evaluate marginal adaptation. The aim of this study was to evaluate the marginal adaptation of the following materials: GIC, MTA and BiodentineTM.
Materials and Methods
Specimen Selection
In this study, 30 freshly extracted human mandibular premolar teeth that were extracted for periodontal and orthodontic reasons were selected. The teeth were obtained under a protocol approved by the Human Research Ethics Committee. All teeth were initially disinfected by immersion in 5.25% sodium hypochlorite for six hours and followed by storage in sterile saline. Inclusion criteria was single rooted mandibular teeth with single root canal and apical foramen. Radiographs were taken in both mesiodistal and buccolingual direction to rule out any calcifications, resorptions, extra canals and curvature of the root canal. Teeth with any sort of defects like internal and external resorptions, root caries, open apices and previous endodontic therapy were excluded from this study.
Specimen Preparation
Crowns were sectioned above the cemento-enamel junction to standardize the working length of the specimens of about 16 mm. Intracanal tissue was extirpated and cleaning and shaping was done using Nickel Titanium rotary system (ProTaper rotary system Dentsply/Maillefer, Tulsa, OK, USA upto F5). Then the canals were obturated with thermoplastisized Gutta-percha and AH plusTM sealer. Then the teeth were apicected with a fissure bur (Dentsply/Maillefer, Tulsa, OK, USA) under constant water spray. After preparing a 3-mm-deep root-end cavity with an ultrasonic tip with light brushing motion on the resected root end, each cavity was irrigated with normal saline and dried with paper points. The teeth were randomly divided into three groups. In Group 1 (n=10), each cavity was filled with Glass ionomer cement type II (GC UNITED KINGDOM, Coopers Court, Newport Pagnell, UK) and in Group 2 and 3 the cavities were filled with white Mineral trioxide aggregate (ProRoot MTATM, Dentsply- Tulsa Dental, Tulsa, OK, USA) and New experimental Ca3SiO5-based restorative cement (BiodentineTM, Septodont, Saint-Maur-des-Fosses, France) respectively according to manufacturer’s instructions. The samples were stored at 100% humidity at 37°C for one week. Then the samples were immersed in rhodamine B dye for 48 hours and washed under running water to remove the excess dye.
Evaluation of Marginal Adaptation
The prepared samples were cut three 1 mm transverse sections using hard tissue microtome (Leica 1600). Samples were examined under 10X magnification using a CLSM. The rhodamine blue dye stained area was measured using computer software programme (Leica). The dye represented gap area was calculated using the software was taken for analysis. Post hoc test was used to analyze the statistical difference between various groups.
Results
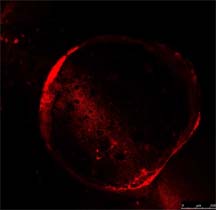
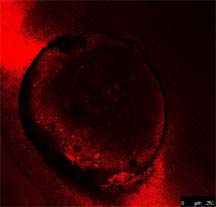
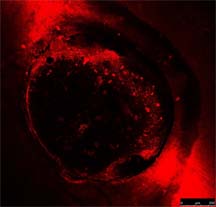
The CLSM examination of the transverse sections of the root end- filled teeth showed marginal gaps at the dentin-filling interface. [Table/Fig-1,2and3] were representative CLSM pictures of root-end cavity filled with GIC, MTA and Biodentine under 10X respectively. Kolmosrov Smirinov test indicated that the data is normal. CLSM analysis of gap area between the dentinal walls and the material used was compared between the groups using one way ANOVA, which showed statistically significant difference (p<0.0001) between all the three groups. Lowest mean gap area of 11143.42±967.75μm2 was found in Biodentine followed by MTA and GIC which had the largest mean gap area of 33388.17±12155.90μm2 and poorest adaptation among the three materials [Table/Fig-4].
Root-end cavity filled with GIC.
Root-end cavity filled with MTA.
Root-end cavity filled with BiodentineTM
Marginal Gap area (μm2) seen under CLSM (10X)
| GIC | MTA | BIODENTINETM |
|---|
| 43,267.66 | 19135.24 | 11,135.26 |
| 34362.44 | 18972.23 | 12176.73 |
| 23234.25 | 23124.62 | 10195.94 |
| 32145.23 | 24126.74 | 11286.29 |
| 25897.32 | 26115.23 | 12146.63 |
| 26783.23 | 25135.11 | 12169.81 |
| 23167.45 | 19955.12 | 10178.32 |
| 29122.49 | 22136.26 | 10035.14 |
| 32456.42 | 26122.81 | 10004.4 |
| 63,445.22 | 18186.32 | 12,105.65 |
| GIC-Glass Ionomer Cement, MTA-Mineral Trioxide Aggregate, SEM-Scanning electron microscope, SD- Standard Deviation |
The inter group comparison by Pairwise Multiple Comparison Procedures was done using Post hoc test, has revealed significant differences between all the three groups when the sections were analyzed (p<0.05).
Discussion
The main aim of root end filling is to prevent the movement of the bacteria and diffusion of bacterial products from the root canal into periapical tissues and vice versa. Gartner and Dorn proposed that an ideal root-end filling material should be easy to manipulate, radiopaque, dimensionally stable, non absorbable, insensitive to moisture, adhesive to dentin, nontoxic, and biocompatible [8]. Many materials have been used for root-end fillings in endodontic surgery. However there is no one material that is universally accepted as the best.
Operating microscopes and ultrasonic instruments have been used in root end filling procedures. The concepts, techniques, and materials for root end filling have been evolving. After eradicating or minimizing the irritants in the root canal system, the root end cavity has to be filled in a practical and convenient way. The choice of a root-end filling material could be governed by biocompatibility, apical sealability, handling properties and long term clinical success [3].
Many studies used dye penetration method for the assessment of marginal adaptation and microleakage. However, traditional dye leakage evaluation has several limitations including dissolution of dye during the process and difficulty in observing the maximum penetration and it has been well documented [9,10].
In the present study, CLSM examination was used to determine the marginal adaptation of root-end filling materials to the surrounding tooth structure. The primary advantage of CLSM is the ability to serially produce thin (0.5 to 1.5 micrometer) optical sections through fluorescent specimens that have a thickness ranging up to 50 micrometers or more. The image series is collected by coordinating incremental changes in the microscope fine focus mechanism (using a stepper motor) with sequential image acquisition at each step. Image information is restricted to a well-defined plane, rather than being complicated by signals arising from remote locations in the specimen. Contrast and definition are dramatically improved over wide field techniques due to the reduction in background fluorescence and improved signal-to-noise. Furthermore, optical sectioning eliminates artifacts that occur during physical sectioning and fluorescent staining of tissue specimens for traditional forms of microscopy [11].
Numerous materials have been suggested as root end filling materials; Gutta-percha, Amalgam, Zinc oxide-eugenol, Cavit, Composite resin, Gold foils, and Glass ionomers etc. [12]. In our study we have used Glass ionomer cement, Mineral trioxide aggregate and BiodentineTM as root end filling materials.
Glass ionomer cement is a material with universal properties. It is a dentin substitute. Its ability to bond chemically to tooth structure provides an excellent marginal seal. Studies have shown that glass ionomer cement possesses antibacterial activity due to slow release of fluoride [13]. However, clinically, the plasticity and stickiness of glass-ionomer cement impede condensation into the root-end cavity, and it is extremely sensitive to moisture [14-17].
Mineral trioxide aggregate was introduced by M. Torabinejad contains tricalcium silicate, tricalcium aluminate, tricalcium oxide, silicate oxide and other mineral oxides forming a hydrophilic powder which sets in presence of water. It shows the formation of calcium-phosphate precipitation at the interface. This interface layer reduces the risk of marginal percolation and gives promising long-term clinical success. It has certain disadvantages like prolonged setting time, difficulty in manipulation and technique sensitivity [18].
New experimental Ca3SiO5-based restorative cement is introduced into the market under the name of BiodentineTM (Septodont, Saint- Maur-des-Fosses, France). It shares both its indications and mode of action with calcium hydroxide, but does not have its drawbacks. BiodentineTM consists of a powder in a capsule and liquid in a pipette. The powder mainly contains tricalcium and dicalcium silicate, the principal component of Portland cement, as well as calcium carbonate. Zirconium dioxide serves as contrast medium. The liquid consists of calcium chloride in aqueous solution with an admixture of polycarboxylate. The powder is mixed with the liquid in a capsule in the triturator for 30 seconds. Once mixed, BiodentineTM sets in about 12 minutes. During the setting of the cement calcium hydroxide is formed. The consistency of BiodentineTM reminds of that of phosphate cement. BiodentineTM is a calcium silicate based material used for crown and root dentin repair treatment, repair of perforations or resorptions, apexification and root-end fillings. The material can also be used in class II fillings as a temporary enamel substitute and as permanent dentine substitute in large carious lesions (Septodont BiodentineTM scientific file, 2010). With the addition of setting accelerators and softeners made its manipulation easy [19]. This Ca3SiO5-based restorative cement has similar sealing ability as glass ionomers but do not require dentine conditioning. The maximum physical properties will be achieved during the first one week after placement. The cement is indicated for resorption repair, apexification, and root end filling. A SEM study conducted on sealing ability of Biodentin, MTA and GIC to dentin concluded that Biodentin exhibited better marginal adaptation to dentin in comparison to MTA and GIC cements and also highlighted the influence of time on marginal adaptation [20].
Although the results of this study show that BiodentineTM provides better adaptation and seal than commonly used root-end filling materials, physical properties as well as in vitro and in vivo biocompatibility tests of this material should be performed.
Conclusion
The results of the present study indicate that this new Ca3SiO5 based cement, BiodentineTM has better marginal adaptation. The better handling properties of this material combined with superior biological, mechanical and physical properties suggest the superiority of BiodentineTM over other root end filling materials.
[1]. Harty FJ, Parkins BJ, Wengraf AM, The success rate of apicoectomy. A retrospective study of 1016 casesBritish Dental Journal 1970 129:407-13. [Google Scholar]
[2]. Altonen M, Mattila K, Follow-up study of apicoectomized molarsInternational Journal of Oral Surgery 1976 5:33-40. [Google Scholar]
[3]. Johnson BR, Considerations in the selection of a root-end filling materialOral Surgery Oral Medicine Oral Pathology Oral Radiolology and Endodontics 1999 87:398-404. [Google Scholar]
[4]. Fogel HM, Peikoff MD, Microleakage of root-end filling materialsJournal of Endodontics 2001 27(7):456-8. [Google Scholar]
[5]. Wang X, Sun H, Chang J, Characterization of Ca3SiO5/CaCl2 composite cement for dental applicationDental Materials 2008 24:74-82. [Google Scholar]
[6]. Wongkornchaowalit N, Lertchirakarn V, Setting time and flowability of accelerated Portland cement mixed with polycarboxylate superplasticizerJ Endod in press 2011 :1-3. [Google Scholar]
[7]. Torabinejad M, Lee SJ, Hong CU, Apical marginal adaptation of orthograde and retrograde root end fillings: a dye leakage and scanning microscopic studyJournal of Endodontics 1994 20:402-7. [Google Scholar]
[8]. Gartner AH, Dom SO, Advances in endodontic surgeryDental Clinics of North America 1992 :357-78. [Google Scholar]
[9]. Wu MK, Wesselink PR, Endodontic leakage studies reconsidered. Part I. Methodology, application and relevanceInternational Endodontic Journal 1993 26:37-43. [Google Scholar]
[10]. Tamse A, Katz A, Kablan F, Comparison of apical leakage shown by four different dyes with two evaluating methodsInternational Endodontic Journal 1998 31:333-37. [Google Scholar]
[11]. Sandison D, Webb W, Background Rejection and Signal-to-Noise Optimization in the Confocal and Alternative Fluorescence MicroscopesApplied Optics 1994 33:603-610. [Google Scholar]
[12]. Gutmann JL, Harrison JW, Surgical endodontics 1991 BostonBlackwell Scientific Publications:230-63. [Google Scholar]
[13]. Inoue S, Yoshimura M, Tinkle JS, Marshall FJ, A 24-week study of the microleakage of four retrofilling materials using a fluid filtration methodJ Endod 1991 Aug 17(8):369-75. [Google Scholar]
[14]. Barkhordar RA, Pelzner RB, Stark MM, Use of glass ionomers as retrofilling materialsOral Surg Oral Med Oral Pathol 1989; Jun 67(6):734-9. [Google Scholar]
[15]. Olson AK, MacPherson MG, Hartwell GR, Weller RN, Kulild JC, An in vitro evaluation of injectable thermoplasticized gutta-percha, glass ionomer, and amalgam when used as retrofilling materialsJ Endod 1990 Aug 16(8):361-4. [Google Scholar]
[16]. Aktener BO, Pehlivan Y, Sealing ability of cermet ionomer cement as a retrograde filling materialInt Endod J 1993 Mar 26(2):137-41. [Google Scholar]
[17]. Pissiotis E, Sapounas G, Spångberg LS, Silver glass ionomer cement as a retrograde filling material: a study in vitroJ Endod 1991 May 17(5):225-9. [Google Scholar]
[18]. Parirokh M, Mahmoud Torabinejad M, Mineral Trioxide Aggregate: A comprehensive literature review-Part I: Chemical, Physical, and antibacterial propertiesJournal of Endodontics 2010 36:16-27. [Google Scholar]
[19]. Wang X, Sun H, Chang J, Characterization of Ca3SiO5/CaCl2 composite cement for dental applicationDent Mater 2008 24:74-82. [Google Scholar]
[20]. Jameel Mohammed Ameen Sulaiman, An in vitro SEM Comparative Study of Dentine-BiodentineTM InterfaceInternational Dental Journal 2013 63(Suppl. 1):1-98.© 2013 [Google Scholar]