Traumatic dental injuries are the most disruptive and distressing emergencies which are presented in the dental practice. Dental trauma has a severe impact on social and psychological well being of a patient. The dentist is often the first health professional who examines such patients who have sustained significant injuries. A majority of fractures and displacements result from simple fall, accidents which occur during sports activities or childish pranks, that may alter the facial appearance from an attractive to an unattractive profile, leaving patients in pain and discomfort [1]. Fractures of coronal portion of anteriors are more common form of dental trauma that mainly affect children and adolescents [2]. Coronal fractures of permanent incisors account for 18-22% of all dental traumas, among which 96% involve maxillary central incisors [3].
Several factors influence the management of coronal tooth fractures, such as biological width violation, endodontic involvement, pattern of fracture, presence or absence of fractured fragment, restorability of tooth, occlusion and aesthetics [2]. Hence, the primary goal of dental professionals must be the preservation of dental tissue, re-establishment of the natural aesthetics of traumatized teeth and maintenance of the integrity of the dental arch. Overtime, numerous techniques have been developed for the reconstruction of fractured teeth, such as resin crowns, steel crowns, orthodontic bands, ceramic crowns and resin composite restorations with and without pins [4]. Veneers and ceramic crowns tend to sacrifice healthy tooth structure too much and they raise the problem of aesthetic matching with adjacent non restored teeth [5]. Considering the treatment modalities for uncomplicated crown fractures, fragment reattachment is also a preferred technique among clinicians. Tooth fragment reattachment offers conservative, aesthetic, cost effective and less time consuming restorations of fractured teeth as compared to those offered by composite or full coverage crowns [2]. Hence, present study was undertaken to evaluate the strengths of reattached fracture fragments by using different techniques.
Materials and Methodology
Materials used
One bottle adhesive system (3M Single Bond), A dual cure resin cement (3M Rely X), Composite Resin Universal Resolution A2 shade (3M Z-100), Light Emitting Diode (LED) and Instron Universal Testing Machine.
Methodology
The present in vitro study was aimed at evaluating the fracture strength recoveries of reattached anterior tooth fragments by using different reattachment techniques. The tooth preparation was done in Department of Conservative Dentistry and Endodontics, Bapuji Dental College, Davangere, Karnataka and lab testing was done at BIET Engineering College, Davangere, Karnataka,India. The study was done between August and October 2004. Forty human permanent central incisor teeth which were free from cracks or other structural defects were selected for the study. The forty teeth were equally divided into four test groups. These teeth were selected under optical magnification (X2). They were disinfected and stored in 0.9% saline solution.
The test basically consisted of three procedures [6].
1) Method of obtaining fragment.
2) Restoration of the fractured teeth.
3) Fracture of the restored teeth.
Method for obtaining fragments
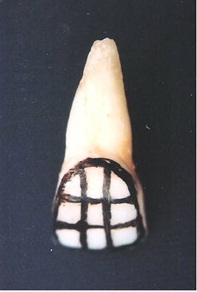
The buccal surface of each tooth was divided into transversal and longitudinal third parts [Table/Fig-1]. Shows the area (point) for application of the perpendicular load for causing fracture of teeth.
Area of load application,
The roots of the teeth were confined to a special device (holder) and adapted in a Universal Testing Machine [Table/Fig-2]. The load was applied to each tooth in a buccal – to – lingual direction by using a small stainless steel ball (2 mm2) which was inserted at the end of a pin which was held in the cross head of the Universal Testing Machine at a cross head speed of 0.6 mm/minutes. The force which was required to fracture the tooth was recorded.
Specimens Confined in a Special Device (Holder) in Universal Testing Machine,

Restoration of the Fractured Teeth by using different reattachment techniques
Both the fragment and the remaining fractured tooth surface were kept in 0.9% saline solution until the restoration procedure was performed. The material which was used was one bottle of adhesive, dual cure resin cement and composite resin which were applied by following the manufacturer’s instructions. The adhesive system was applied to both the fragment and the remnant. However, the adhesive was not immediately light- cured, in order to avoid any interference with the fit between the parts which had to be bonded.
After that, the resin cement was applied, the fragments were reattached and they were light cured for 40 seconds (both buccal and lingual surfaces). The fragment and the remaining fracture tooth surface were restored by using different reattachment techniques, such as;
1) Simple reattachment.
2) External chamfer.
3) Over contour.
4) Internal dentinal groove.
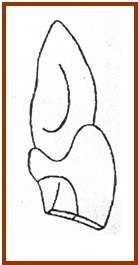
Technique I: Simple re-attachment
No additional preparation was made – fractured fragments were only bonded [Table/Fig-3].
Technique 2: External chamfer
After re-attachment of fractured tooth fragments, a 1.0 mm depth chamfer was placed in the fracture line, in the buccal surface, by using a diamond round bur [Table/Fig-4].

Technique 3: Over contour
Prior to performing the re-attachments of fractured tooth fragments, preparation was done in the buccal surface by using a cylindrical diamond finishing bur. The preparation extended 2.5 mm coronally and apically from the fracture line, with a depth of 0.3 mm. The increment of resin composite was used to restore the buccal surface after applying the adhesive system. This created a slightly over contoured tooth surface.
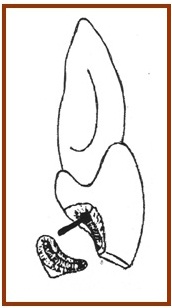
Technique 4 : Internal dentinal groove
Prior to performing the re-attachment of fractured tooth fragments, an internal groove (1 mm deep and 1 mm wide) was placed within the fragment and the remaining tooth by using a carbide bur with a water coolent and a high speed hand piece. The adhesive system was applied to each surface. Prior to light curing, a resin composite was placed within the groove. The fragment was reattached and the excess composite was removed. Each surface was then light cured for 40 seconds [Table/Fig-5].
Fracturing of the restored teeth after reattachment techniques
The specimens were loaded in the same pre-determined area which was used in procedure, to obtain fragments. The force which was required to detach each fragment was recorded in KgF. The fracture strengths of all sound teeth were averaged. For each tooth, the fracture strength was expressed as a percentage of the load which was required to fracture the sound tooth (strength recovery). This resulted in establishment of a relationship between the fracture strength of an intact tooth and those which were obtained after restoration procedures which were done for all groups. One way ANOVA and Tukey’s test (α = 0.05) were used to evaluate differences among the techniques for each method of obtaining fragment. A comparison of the fracture strength relatively of similar technique under the different methodologies, was evaluated by using Student’s t-test (α = 0.05).
Results
The mean force (Standard deviation) which was required to fracture sound teeth was 22.12 ± 4.1 KgF. The mean fracture resistance (KgF) and standard deviation of sound and restored teeth and the fracture strength recovery (%) of each group was calculated [Table/Fig-6]. Technique 1 (Bonded only) and Technique 2 (External Chamfer) showed similar fracture strength recoveries (p>0.05). However, these values were lower than those which were obtained by using Technique 3 (Over contour) and Technique 4 (Internal groove). Technique 1 (Bonded only) and Technique 2 (External Chamfer) showed fracture strength recoveries of 44.3% and 60.6% respectively. But Technique 3 (Over contour) and Technique 4 (Internal Dentinal Groove) showed excellent fracture strength recoveries of 86.8% and 89.8% respectively, which were much superior than those obtained by Technique 1 (Bonded only) and Technique 2 (External Chamfer).
Mean Fracture Strength (KgF) recovery and Standard Deviation in experimental Groups
| Fracture |
|---|
| Reattachment Techniques | Mean | ± SD | % (*) |
| 1. Bonded only | 9.8 | 3.7 | 44.3 |
| 2. External Chamfer | 13.4 | 4.8 | 60.6 |
| 3. Over contour | 19.2 | 3.4 | 86.8 |
| 4. Internal groove | 19.8 | 2.2 | 89.5 |
*Fracture strength recovery was calculated based on the mean and standard deviation of the fracture strength of sound teeth
Discussion
The incidences of dental trauma have increased in number among children and teenagers. Success in identification and management of traumatic fractures can be predicted through a thorough patient examination and treatment planning. For uncomplicated crown fractures, “Reattachment of fractured tooth fragments” is one of the treatment options [7]. Various techniques and designs have been proposed for reattachments of fractured tooth fragments, like bevel designs, chamfers, dentin and enamel grooves, and resin composite materials [1,2].
Reis et al., concluded that a simple reattachment with no further preparation of the fragment or tooth could restore only 37.1% of the intact tooth’s fracture resistance, but that a buccal chamfer recovered 60.6% of that fracture resistance and bonding, with an over contour and placement of an internal groove restores fracture strengths of 97.2 and 90.5% respectively, which were similar to those seen in our study [1].
Badami et al., showed that neither the bevel nor the material which was used to obtain the original fracture resistance of the tooth, but that rather the resistance of the fracture segment could be directly proportional to the surface area of adhesion. They observed highest fracture resistance on using chemically cured composite, followed by light cured cement and bonding agent (showed the least resistance) [8]. Several researchers concluded that flowable composite not only reinforced the tooth, but that it also helped in achieving a higher bond strength [3].
Reis et al., showed that chamfer group showed a higher fracture strength recovery (67.9%) than bonded group (41.1%), which was in accordance with findings of our study [9]. Loguercio et al., concluded that over-contour and internal dentinal groove technique showed highest fracture strengths as compared to those obatined by bonded, chamfer and resin composite buildups for fractured fragment reattachments, which was in accordance with findings of our study [6]. Bhargava et al., showed that a combination of nano-composite and chamfer preparation had the highest mean fracture strength [10]. Similarly, Kovacs et al., observed that use of both material and techniques in combination could affect bond strength [5]. Bruschi-Alonso et al., concluded that no technique or material, when it was used individually, was capable of achieving the mechanical strength of sound teeth, and they observed that circumferential chamfer was superior to direct bonding [11].
Clinical considerations for reattachments of tooth fragments
Following principles have been proposed, based upon the possibility of bonding of the fractured anterior fragments [12]. The first step was to try-in the number of tooth fragments, to determine the fit of the parts and to determine whether there were any missing parts of the tooth. The ideal indication existed when the fracture was a clear section with a single tooth fragment, in a suitable condition.
Fragment preparation [
13]
The first step consisted of cleaning and disinfection of the different fragments by using mechanical and chemical techniques. Polishing pate, NaOCl, and alcohol (70%) have been suggested to remove protein coating from the fragments. The second step aims at the reconstruction of the dental crown, through assembling of the fragments, in order to check the fit and to note any missing parts.
Periodontal Assessment [
13]
Gentle probing around the periodontal tissues of the fractured tooth under local anaesthesia is recommended. It helps in determining the level of the tooth fracture, as well as the presence of any vertical root fracture. If the fracture line is supragingival, the procedure for reattachment will be straight forward. However, when the fracture site is subgingival or intraosseous, orthodontic extrusion of the apical portion, for restoration with a post-retained crown, instead of reattachment, may be necessary.
Endodontic Assessment
In addition to clinical examination for pulpal exposure, the vitality of the pulp and status of apex maturation should be analyzed by doing vitality tests and checking periapical radiographs.
Provided that minimal damage to the fragment has occurred, simple disinfection of the tooth and its fragment with 0.12% chlorhexidine solution before opposition is effective. If multiple fragments are present, it may be necessary to assemble the pieces with resin composite, prior to trail in the mouth. Following cleaning of the fractured tooth and fragment, reattachment can be done. Several studies have shown that over contour and internal dentinal groove reattachment technique showed excellent performances as compared to the other techniques which were tested. Studies have shown that the sole use of an adhesive system or combination materials with better mechanical properties, such as flowable resins, resin cements and resin composites had led to similar results when the fragment was reattached and this required no additional preparation [9]. However, despite the statistical similarity, there was a trend towards improving fracture strength when the adhesive system was combined with a resin composite, which was most likely caused by the improved mechanical properties of this material as compared to those of the others which were used [14].
Fragment reattachment is advantageous, since it conserves dental tissue, is colour matched with natural tooth, maintains original tooth contour, reduces chair side time and as it is an economical procedure. Whereas, it has some disadvantages such lesser than ideal aesthetics, if the tooth fragment is allowed to dehydrate, if colour of the bonded fragment changes, continuous monitoring is necessary, if it has unknown longevity and if there are chances of separation of the repair caused by progressive breakdown of the bonded junction.
With use of available newer materials, in conjunction with appropriate techniques, aesthetics, with long term durable restoration of fractured fragment reattachment can be achieved. Reattachment of fractured fragment is a conservative approach which can be used for restorinh function and aesthetics of fractured tooth. Whereas, further research is needed to test the long term success of reattachment of a fractured fragment.
Conclusion
This in vitro study concluded that over contour and internal dentinal groove reattachment technique showed excellent performances as compared to the other techniques which were tested. Reattachment of fractured fragment is faster, easier, and cost effective. Highest strength can be achieved by using a combination of techniques and bonding materials. Hence, reattachment of fractured fragments can be a preferred technique.
*Fracture strength recovery was calculated based on the mean and standard deviation of the fracture strength of sound teeth