Assessment of Lingual Frenulum Lengths in Skeletal Malocclusion
Swarna Meenakshi1, Nithya Jagannathan2
1 Undergraduate Student, Saveetha Dental College, Saveetha University, Annanagar, Chennai, India.
2 Senior Lecturer, Department of Oral Pathology, Saveetha Dental College, Saveetha University, Annanagar, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nithya Jagannathan, No 1500/3, 16th Main Road, Annanagar, Chennai– 600040, India.
Phone: 9884754910,
E-mail: dr.nithya@ymail.com
Background: The orofacial musculature plays a pivotal role in maintaining a balance in positioning of the teeth and any imbalance which occurs in this , results in malocclusion. Lingual frenum is a soft tissue structure which tethers the ventral surface of the tongue to the floor of the mouth.
Objective: This study was performed to analyze the lingual frenal lengths in skeletal class I, class II and Class III malocclusion and to correlate relationship between both.
Materials and Methods: This study comprised of 30 subjects, with 10 in each group and an impression was made with the maximum mouth opening position and the tip of tongue touching the incisive papilla. The length of the lingual frenum was then measured from the casts. The maximum mouth opening position was also determined by measuring the interincisal distance with the maximum mouth opening position. Statistical analysis was done to analyze the relationship between both.
Results: The lingual frenum was found to be longest in class III malocclusion, with a statistical significant value of p<0.01. The class II and class I malocclusion did not show much difference. The maximum mouth opening position was also increased in class III malocclusion, followed by class II and class I malocclusion, in a descending order.
Conclusion: The lingual frenum exerts erratic forces and a long lingual frenum pushes the mandibular anteriors forwards, resulting in malocclusion. Hence, a relationship between the lingual frenum and malocclusion is essential, so that the erratic forces can be eliminated and excellent results can be achieved, following the correction of malocclusion.
Frenum, Ankyloglossia, Tongue, Malocclusion
Introduction
A coexistence between the genetic factors and the arrangement of soft tissues in the orofacial region has been suggested as the aetiological factor of malocclusion [1–3]. However, the growth and development of the orofacial musculature in malocclusion have to be emphasized, as they serve as unfavourable factors and are regarded as the keys in the management of malocclusion [4]. The teeth and alveolus are sandwiched between the buccal mucosa, lips and the tongue and there exists a balance between these, for maintainence of the position of the dentition. However, tongue is a much powerful organ and any changes which occur in the posture of the tongue musculature could serve as potential factors in causation of malocclusion [5,6]. Lingual frenum is a soft tissue mucosa which extends from the ventral surface of the tongue, in the midline, to the floor of the mouth, which thus secures the motions of the tongue [7]. The frenum is attached to the tip of the tongue in varying degrees and the frenulum length and the thickness exert an influence on the mobility of the tongue [8].
The tongue originates from first, second and third pharyngeal arches at four weeks of intrauterine life and the origin of muscles occurs by the migration from occipital myotomes. Initially, a U-shaped sulcus is formed on either sides of the tongue. This allows the free mobility of tongue, except at the region of attachment of lingual frenum. As the development of the tongue proceeds, the lingual frenulum cells undergo apoptosis and the lingual frenulum retracts away from the tip of the tongue. There could be a disturbance during this stage of programmed cell death, which may lead to a condition which is called ‘Tongue tie’ or ‘Ankyloglossia’. Ankyloglossia is a congenital anomaly, wherein the lingual frenum tethers the floor of the mouth to the ventral surface of the tongue. This results in shortening of the frenulum length, resulting in speech disorders, orthodontic anomalies and breast feeding difficulties [9–12]. The restrictions in the tongue’s mobility often result in forward thrusting of tongue against the anterior body of the mandible, thereby resulting in malocclusion [13]. Also, the posture of tongue varies with malocclusion, it being highest in class II malocclusion, intermediate in class I malocclusion and lowest in class III malocclusion [14].
Several studies have been conducted to evaluate the interaction between position of the tongue and malocclusion. However, a review of literature shows scarcity in the association between the lingual frenum and malocclusion. Hence, this study was performed to assess the relationship between the lingual frenum and dental malocclusion.
Materials and Methods
Patient sampling
The study samples included thirty patients of Saveetha Dental College, Saveetha University, India. Patients with class I, II and III malocclusion, who were placed in age group of 12–16 years, were enrolled in the study. The selection of patients in each group was done by a random sampling method and the study was performed over a period of three months. Patients with previous histories of frenectomies, orthodontic treatments, orthognathic surgeries and TMJ disorders were excluded from our study. The patients were distributed into three groups with ten in each group, based on the malocclusion.
Measurement of median lingual frenum length
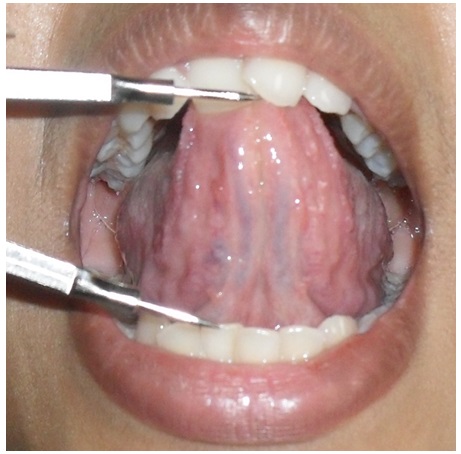
The subjects were instructed to open the mouth to the maximum and elevate the tongue and touch the tip of the tongue on the incisive papilla, while the impression was being made. An irreversible hydrocolloid impression of the mandible was made and prediagnostic casts were made. The vertical distance between the anterosuperior most point of the lingual frenum and the mesioincisal edges of the mandibular central incisor was measured by using vernier calipers. This measurement determined the maximum lingual frenulum length. The values were tabulated and statistical analysis was performed [Table/Fig-1] [15–17].
Determination of Median lingual frenal length in a prediagnostic cast

Maximum mouth opening reduction
The maximum mouth opening reduction was recorded in two steps. The patient was asked to open his/her mouth as wide as possible and the inter-incisal measurement (incisal margin of maxillary central incisor and mandibular central incisor) was determined. The patient was then requested to place the tip of tongue on the incisive papilla and the interincisal distance at this position was recorded again. The difference in the two values gave the reduced amount of maximum mouth opening [Table/Fig-2].
Determination of maximum mouth opening at reduction
Statistical Analysis
The statistical analyzes were carried out by using the statistical software (SPSS for Windows, version 14.0). The median lingual frenulum length and maximum mouth opening reductions of skeletal class I, II, and III malocclusion were compared by doing analysis of variance (ANOVA) test and paired t-test was done to determine the significance in the relationship between the frenum and malocclusion. Pearson’s correlation analysis was performed to determine the relationship between the maximum mouth opening reduction and the median lingual frenum length.
Results
The descriptive statistics of the MLFL and MMOR measurements in the three groups have been tabulated [Table/Fig-3]. MLFL was found be highest in skeletal class III malocclusion, with a value of 5.27 and a standard deviation of 1.02, followed by class II malocclusion. The class I malocclusion subjects had a frenulum length of 3.96 ±1.46, which was much lesser than that of class III malocclusion. Descriptive statistics showed p-value to be less than 0.01, which demonstrated a significance of about 95%, (p<0.01) between class III malocclusion and class I malocclusion. However, the MLFL of class II malocclusion did not show much significance with class I and class III malocclusion. The amount of maximum mouth opening reduction was significantly increased, with an increasing median lingual frenulum length and a p-value of less than 0.1 (p<0.1). The Pearson’s correlation analysis showed a positive correlation between the median lingual frenulum length and the maximum mouth opening reduction.
Frenulum Length in Dental Malocclusion
| Numbers | Class I Malocclusion n=10 | Class II Malocclusion n=10 | Class III Malocclusion n=10 |
|---|
| Mean | SD | Mean | SD | Mean | SD |
|---|
| Median lingual frenulum length | 3.96 | 1.46 | 4.08 | 0.96 | 5.27 | 1.02 |
| Maximum Mouth opening reduction | 14.25 | 4.7 | 16.36 | 3.35 | 20.46 | 5.76 |
Discussion
The inheritance of malocclusion is influenced by genetic and environmental factors, but with a greater emphasis on the influence of environment, in particular, the orofacial tissues [18–21]. The positioning of the soft tissues and the tongue posture has a prime role in determining the positioning of the teeth and it is also a determiner of bone formation. Despite the curious role played by tongue in the development of the structures in the orofacial region, the tongue often remains a rather quiescent organ without any bony skeleton. However, the neuro-muscular complex of tongue is vital in developmental and also in functional processes [22]. Ankyloglossia is a congenital condition which results in tethering of the tongue to the floor of the mouth at various levels. The mobility of tongue is usually restricted, resulting in a forward push of the low postured tongue, due to the pharyngeal musculature [23]. This often results in the growth of the mandible in a prognathic manner, resulting in skeletal class III malocclusion [24].
Though numerous studies have been on the association between soft tissue posture and malocclusion, there has been a scarcity in studies done on the association between the frenulum and skeletal malocclusion. Thus, this study was an attempt which was made to assess the relationship between the lingual frenulum and malocclusion. The present study was based on determination of the lingual frenal lengths and the maximum mouth opening reductions in all the three classes of malocclusion and it thereby determined the association between them. The cybernetic growth of the mandible explains that the anteroinferior growth of the maxilla causes a functional shift in the mandible, leading to an alteration in the posture of the temperomandibular joint. This results in mandibular remodeling or growth [25]. If the maxillary growth is restricted, it could often result in a flattened palate, resulting in a diminished lingual volume. This spatial inadequacy leads to inferior positioning of the tongue, resulting in erratic forces acting on the mandible, leading to mandibular prognathism [26].
The present study demonstrated median lingual frenal length and maximum mouth opening reduction to be significantly increased in class III skeletal malocclusion. This suggested that patients with increased MLFLs were prone to development of skeletal class III malocclusion. An association between ankyloglossia and malocclusion has been described in literature [27]. The findings of present study thus, correlated with those of the previously described studies and they brought about a positive correlation between mandibular prognathism and lingual frenum.
The positioning of the lingual frenum varies from birth until puberty. The lingual frenulum length is often short in newborns and the thickness of the frenum decreases with an increase in age, resulting in a long and narrow tongue [28,29]. The complete growth of the tongue is established at Eight years of age, whereas the mandible has a prepubertal growth spurt. Therefore, until puberty, the tongue is positioned at a lower level, resulting in mandibular prognathism [6]. Therefore, an early diagnosis of mandibular prognathism and its associated tongue tie/ increased medial lingual frenulum length aids in an early correction, thereby promoting better prognosis which follows a treatment.
Conclusion
Lingual frenulum, a soft tissue mass which connects the floor of mouth and the ventral surface of tongue, exerts erratic forces on the mandible, thus influencing the development of mandible from embryonic stages. This leads to a skeletal malocclusion, with the degree being influenced by the different levels of attachment of the frenum on the tongue. The present study measured the frenal length and maximum mouth opening length in various classes of malocclusion. Patients with class III malocclusion were associated with long frenal lengths, which eventually led to exertion of forces on the mandible, resulting in prognathism. Similarly, tongue tie or inhibited motility of tongue results in mandibular retrognathism.
Future Scope
The role of frenal lengths in malocclusion has not been much discussed over the years. Early diagnosis of frenal length enables early correction or it even prevents the chances of skeletal malocclusion. The prognosis of the treatment is also better, following corrections of lingual frenal lengths in skeletal malocclusion.
Limitations
Studies which are being done on the association of lingual frenum and orofacial musculature are still in infantile stages. Further studies should be done, to assess the association of craniofacial morphology with the lingual frenum and malocclusion and they would give us better insight on the extrinsic factors which cause malocclusion.
[1]. Mew JR, Factors influencing mandibular growthAngle Orthod 1986 56:31-48. [Google Scholar]
[2]. Defabianis P, Ankyloglossia and its influence on maxillary and mandibular development. (A seven year follow-up case report)Funct Orthod 2000 17:25-33. [Google Scholar]
[3]. Ruffoli R, Giambelluca MA, Scavuzzo MC, Bonfigli D, Cristofani R, Gabriele M, Ankyloglossia: a morphofunctional investigation in childrenOral Dis 2005 11:170-4. [Google Scholar]
[4]. Alhaddad Salwa Jeragh, Ankyloglossia in a Pseudo-Class III malocclusion: A case reportSmile Dental Journal 2011 6(2):12-16. [Google Scholar]
[5]. Proffit WR, Equilibrium theory revisited: factors influencing position of the teethAngle Orthod 1978 48:175-86. [Google Scholar]
[6]. Proffit WR, Mason RM, Myofunctional therapy for tongue-thrusting: background and recommendationsJ Am Dent Assoc 1975 90:403-11. [Google Scholar]
[7]. LA Kotlow , Oral diagnosis of abnormal Frenum Attachments in neonates and infants: Evaluation and treatment of the maxillary and lingual frenum using the erbium: YAG laserThe Journal of Pediatric Dental Care 2004 10(3):106-12. [Google Scholar]
[8]. Pola Ma José García García, González Manuel, Martín Manuel José, García Gallas, Mercedes, Lestón Juan Seoane, A study of pathology associated with short lingual frenumJournal of Dentistry for Children 2002 69(1):59-62. [Google Scholar]
[9]. Chaubal Tanay V, Dixit Mala Baburaj, Ankyloglossia and its managementJournal of Indian Society of Periodontology 2011 15(3):270-72. [Google Scholar]
[10]. Dyad Ballard Lauer CE, Khoury JC, Ankyloglossia: assessment, incidence, effect of frenuloplasty on the breast feedingPediatrics 2002 110(5):63 [Google Scholar]
[11]. Coryllos Elizabeth, Salloum Alexander C, Genna Catherine Watson, Congenital tongue tie and its impact on breast feedingAmerican Academy of Pediatrics 2004 [Google Scholar]
[12]. Notestine Gregory E, Importance of identification of ankyloglossia as a cause of breast feeding problemsJournal of Human Lactation 1990 6(3):113-15. [Google Scholar]
[13]. Horton CE, Crawford HH, Adamson JE, Ashbell TS, Tongue tieCleft Palate J 1969 6:8-23. [Google Scholar]
[14]. Hopkin GB, Neonatal and adult tongue dimensionsAngle Orthodontics 1967 37:132-3. [Google Scholar]
[15]. Bissasu M, Use of lingual frenum in determining the original vertical position of mandibular anterior teethJ Prosthet Dent 1999 82:177-81. [Google Scholar]
[16]. Prasad KD, Alva H, Use of frenum in determining the original vertical position of teeth.J Oral Health Comm Dent 2013 7(1):44-46. [Google Scholar]
[17]. Srinivasan Bhadrinath, Chitharanjan Arun B, Skeletal and dental characteristics in subjects with ankyloglossiaProgress in Orthodontics 2013 14:44 [Google Scholar]
[18]. Markovic MD, At the crossroads of oral facial geneticsEur J Orthod 1992 14:469-81. [Google Scholar]
[19]. Horowitz EP, Oxbourne RH, de George FC, Cephalometric study of craniofacial variations in adult twinsAngle Orthod 1960 30:1-5. [Google Scholar]
[20]. Defabianis P, Ankyloglossia and its influence on maxillary and mandibular development. (A seven year follow-up case report)Funct Orthod 2000 17:25-33. [Google Scholar]
[21]. Ruffoli R, Giambelluca MA, Scavuzzo MC, Bonfigli D, Cristofani R, Gabriele M, Ankyloglossia: a morphofunctional investigation in childrenOral Dis 2005 11:170-4. [Google Scholar]
[22]. Lee SK, Kim YS, Lim CY, A pathological consideration of ankyloglossia and lingual myoplastyTaehan Chikkwa Uisa Hyophoe Chi 1989 27(3):287-308. [Google Scholar]
[23]. Petit H, Davis W, The role of the tongue in facial developmentJ Pedod 1986 10:199-210. [Google Scholar]
[24]. Horton CE, Crawford HH, Adamson JE, Ashbell TS, Tongue-tieCleft Palate J 1969 6:8-23. [Google Scholar]
[25]. Petrovic A, Experimental and cybernetic approaches to the mechanism of action of functional appliance on mandibular growth. In: McNamara JA Jr, Ribbens KA, editorsMalocclusion and the periodontium. Monograph 15. Craniofacial Growth Series 1984 Ann ArborCenter for Human Growth and Development; University of Michigan [Google Scholar]
[26]. Frankel R, Frankel C, Orofacial orthopedics with the function regulator 1989 BaselKarger:167-8. [Google Scholar]
[27]. So-Jeong Jang, Bong-Kuen Cha, Peter Ngan, Dong-Soon Choi, Suk-Keun Lee, Insan Jang, Relationship between the lingual frenulum and craniofacial morphology in adultsAm J Ortho Dentofac Orthoped 2011 139(4):361-e367. [Google Scholar]
[28]. Kotlow LA, Ankyloglossia (tongue-tie): a diagnostic and treatment quandaryQuintessence Int 1999 30:259-62. [Google Scholar]
[29]. Neville BW, Damm DD, Allen CM, Bouquot JE, Oral and Maxillofacial Pathology 1995 2nd edPhiladelphiaWB Saunders Company:10-1. [Google Scholar]