Solitary Sessile Osteochondroma of Scapula, A Rare Case Report
Yashavantha Kumar C1, Satish Shervegar2, Daksh Gadi3, Rahul P4
1Assistant Professor, Department of Orthopaedics, M S R Medical College, Bangalore, India.
2Professor, Department of Orthopaedics, M S R Medical College, Bangalore, India.
3Junior Resident, Department of Orthopaedics, M S R Medical College, Bangalore, India.
4Assistant Professor, Department of Orthopaedics, M S R Medical College, Bangalore, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR:Dr. Yashavantha Kumar C, Assistant Professor, Department of Orthopaedics, M S R Medical College, Bangalore, India.
Phone: 919663581868,
E-mail:kumyshwanth@gmail.com
Osteochondromas are the most common benign tumours of bone. These are most commonly seen on the metaphysis of a long bone, but they can arise from any bone which is preformed from cartilage. To best of our knowledge, very few cases of osteochondroma scapula have been reported in literature. We hereby report a very rare case of osteochondroma which arose from scapula in a four year old boy, which was treated by excisional biopsy.
Osteochondroma, Sessile, Scapula
Case Vignette
A swelling was noticed over the right scapula of a four year old boy by his parents since the past one year, which showed progress since past 6 months [Table/Fig-1]. On examination, no similar swelling was seen, which arose from else where in the body. Family history was not significant. On examination, a 4x3cm bony swelling which arose from body of left scapula was noticed. The swelling was hard in consistency, it had a smooth surface and it was immobile, but it moved with scapula. Skin over the swelling was normal and there were no neurological deficits. Forward flexion, abduction and extension of shoulder joints were restricted terminally.
Plain radiograph of right shoulder revealed a mushroom shaped, solitary osteochondroma. MRI showed a bony swelling of size, 30x17mm, which arose from the dorsal surface of the body of the scapula. The cartilage cap thickness was 5mm. The cortex and the medullary cavity were continuous with the scapula. There was no associated soft tissue mass or pathological fracture.
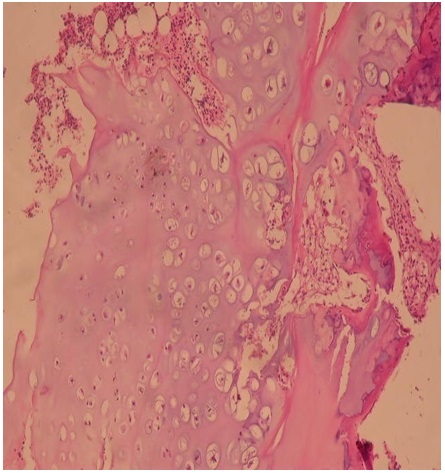
He was taken up for excisional biopsy, as the swelling restricted his shoulder movements and was cosmetically not acceptable [Table/Fig-2]. Under general anaesthesia in prone position, an oblique incision was made and the entire tumour was excised. Histopathological examination concurred with our preoperative diagnosis. There was no evidence of malignant changes. Post- operative period was uneventful and the boy regained appreciable shoulder range of motion with physiotherapy. After six months of follow-up, there was no evidence of recurrence. Histopathological examination showed normal appearing chondrocytes which were covered by hyaline cartilage. There is no evidence of any malignant transformation [Table/Fig-3].
Discussion
Osteochondromas are pseudotumours with developmental malformations around the growth plate [1] . These are seen in children, mostly during rapid skeletal growth and they arise from any bone in the body which is preformed in cartilage. Distal femur, proximal tibia and proximal humerus are the most common sites.
Osteochondromas tend to grow during paediatric age group and this growth can occur till third decade of life. Malignant transformations are extremely rare in children and they are uncommon in adults. Malignant transformation occur when the lesion involves, pelvis and proximal femur. The incidence of malignant degenerations in solitary osteochondromas is 1% and in multiple osteochondromas, it is 5%. A malignant transformation should be suspected when there is a sudden increase in growth in an adult who is more than 30 years of age. In malignant transformations, the cartilage thickness is more than 2cm and these are best evaluated by CT scan or MRI [2-5] .
Osteochondromas are the most common tumours of the scapula, which account for 4.6% of all bone tumours [6] . They are more common on the ventral side of the scapula. Osteochondromas of ventral scapula can lead to various complications like bursa formation, pseudowinging of scapula, snapping syndrome and restricted movements of the shoulder. Excisions of osteochondromas had relieved the symptoms in previously reported cases [7-10] [Table/Fig-4] .
In our case, we planned an excision because the osteochondroma had rapidly increased in size since past six months. The swelling also caused pseudowinging of scapula and terminal restriction of movements. On follow up, pseudowinging of scapula improved and regained full range-of-motion. There was no recurrence of swelling.
Clinical photograph showing swelling arising from scapula

Plain radiograph showing sessile osteochondroma of body of scapula

Histopathological picture of osteochondroma
Review of similar cases of osteochondroma of scapula in literature
| Author | Year | Chief Complaints | Treatment |
| Kristopher et al., | 2010 | Swelling in the axilla, Paresthesias in the arm | Arthroscopic excision |
| Rohit Prakash et al., | 2012 | Swelling and pain in the right upper back, Clunking of shoulder | Excisional biopsy |
| Kyoji Okada et al., | 1999 | Pain and swelling in the shoulder | Excision |
| Aalderink et al., | 2010 | Shoulder pain and winging of scapula | Arthroscopic excision |
| Yoo et al., | 2008 | Swelling in the upper back | excision |
| Our case | 2013 | Swelling and movement restriction | Excisional biopsy |
Conclusion
Osteochondromas of scapula are very rare, benign bone tumours. They can cause pseudowinging of scapula, pain and restriction of shoulder movements. Open or arthroscopic excision of tumours will relieve most of these symptoms.
[1]. JW Milgram, The origins of osteochondromas and enchondromas: a histopathology study.Clin Orthop. 1983 :174-264. [Google Scholar]
[2]. RC Garrison, KK Unni, RA McLeod, al et, Chondrosarcoma arising in osteochondroma.Cancer 1982 49:1890 [Google Scholar]
[3]. P Canella, F Gardini, Exostosis Boriani S., development, evolution and relationship to malignant degeneration. Ital J Orthop Traumatol. 1981 7:289-93. [Google Scholar]
[4]. JK Lee, L Yao, CR Wirth, MR imaging of solitary osteochondromas: report of eight cases.Am J Roentgenol. 1987 149:557 [Google Scholar]
[5]. Rh Lange, TA Lange, BK Rao, Correlative radiographic, scintigraphic, and histological evaluation of exostoses.J Bone Joint Surg Am.t 1984 66:1454 [Google Scholar]
[6]. JF Galate, JM Blue, RW Gaines, Osteochondroma of the scapula.Mo Med. 1995 92:95-97. [Google Scholar]
[7]. LG Danielson, I el-Haddad, Winged scapula due to osteochondroma: Report of 3 children.Acta Orthop Scand. 1989 60:728-29. [Google Scholar]
[8]. K Okada, K Terada, R Sashi, N Hoshi, Large bursa formation associated with osteochondroma of the scapula: a case report and review of the literature.Jpn J Clin Oncol. 1999 29(77):356-60. [Google Scholar]
[9]. MS Mohsen, NK Moosa, P Kumar, Osteochondroma of the scapula associated withwinging and large bursa formation.Med Prin Pract. Surg Am. 1950 32:561-56. [Google Scholar]
[10]. RP Reit, FV Glabbeek, Arthroscopic resection of a symptomatic snapping subscapular osteochondroma.Acta Orthop Belg. 2007 73:252-54. [Google Scholar]