Be Careful with an IV Line
Raghunath Prabhu1, Rajgopal Shenoy2, Nitin Thinda3, Anisha Patel4, Sakshi Sadhu5
1 Assistant Professor, Department of Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
2 Professor, Department of Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
3 Intern, Department of Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
4 Intern, Department of Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
5 Intern, Department of Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raghunath Prabhu, Assistant Professor, Department of Surgery, Kasturba Medical College, Manipal University, Manipal, Karnataka-576104, India.
Phone: +919448903817,
E-mail: drraghu81@yahoo.co.in
Obtaining an intravenous (IV) access is a simple procedure which can be done in almost any hospital setting. One of the most dreaded complications of this procedure is an inadvertent intra-arterial cannulation. This can result in an accidental injection of medications intra-arterially, which can potentially lead to life altering consequences. In the hope that these types of events can be prevented, we are presenting a case of a 57-year-old male who underwent bougie dilatation for an oesophageal stricture and was accidentally given medication for pain management intra-arterially through an improperly placed IV line, which resulted in ischaemia, gangrene and subsequent loss of the hand. Those who try to obtain an IV access should always be on the lookout for possible clues that can prevent an inadvertent IA injection, especially if cannulation is in an area where an artery is in close proximity to a vein; these clues include but are not limited to the following: a bright-red flash of blood in the cannula, pulsatile movement of blood in the IV line, and intense pain or burning at the site of injection. These signs, as well as educating the patient on early symptoms of ischaemia, may allow early action to be taken, to prevent irreparable damage. We always have to be careful when we insert an I.V line.
Intravenous access, Intra-arterial cannulation, Intra-arterial injection, Gangrene
Case Report
A 57-year-old male with a past surgical history of a transhiatal oesophagectomy which was done for oesophageal carcinoma, presented with the complaint of dysphagia. Multiple bougie dilatations had already been done in the past, to relieve a stricture. A provisional diagnosis of a recurring stricture oesophagus was made. An upper gastrointestinal endoscopy was obtained and narrowing was observed at the anastomotic site; a diagnosis of a post-operative oesophageal stricture was confirmed and he underwent a bougie dilatation.
Post-operative pain management was achieved by giving an IV injection of Fortwin (pentazocin). During its administration, he complained of a “hot flush sensation” as well as pain in the right hand at the IV line site. Two days later, redness and swelling was noted around the injection site. A right hand arterial Doppler was obtained and it showed radial artery thrombosis with complete occlusion, as well as a monophasic waveform in the proximal half of the ulnar artery, along with a trickle of flow in its distal half. A diagnosis of right arterial thrombosis which was secondary to an inadvertent IA injection was made. A CVTS consult advised that the patient be started on low molecular weight heparin. Despite this, blackish discolouration of the fingertips developed and gangrene ensued, compelling debridement under a brachial plexus block. A repeat Doppler was done, which showed a persistent thrombus in the right radial artery. LMWH was changed to oral Acitrom (nicoumalone), after which he was discharged and was told to return when the dry gangrene showed a clear line of demarcation.
He returned two weeks later, and unfortunately the gangrene had progressed from his fingertips (which were now black and shriveled) to his entire palm, which was blackish and oedematous. Signs which were indicative of an extensive tissue injury were present: a right hand that was cold to touch, absence of sensation at the fingertips and decreased sensation over the palm, and absence of right radial and ulnar arterial pulsations. This quickly progressed to loss of all sensations over the right hand, and a clear line of demarcation was noted [Table/Fig-1,2]. Wrist disarticulation was done eventually. Post-operatively, the amputation stump appeared healthy and he was advised regular follow-ups upon discharge.
The red arrow indicates the site of inadvertent IA injection
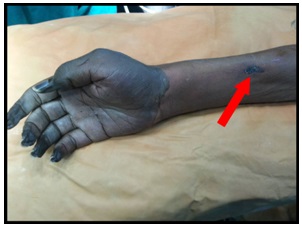
Gangrene of the right palm and fingertips, showing a clear line of demarcation

Discussion
Though the exact incidences of an inadvertent IA cannulation and a subsequent injection are unknown, it has been estimated that the frequencies may range from as low as 1:56000 to as high as 1:3440 [1]. As such, we believe that it is appropriate to increase awareness to prevent and manage similar occurrences in the future. Traditionally, these situations have arisen in the setting of pre-operative anaesthesia, but it is important to note that their incidences are not limited to the operating room. We can see cases in both the non-surgical inpatient settings as well as outside the hospital, since non-iatrogenic accidental IA injections have been reported in illicit drug users and addicts. Early clinical manifestations may offer clues for alerting providers before an irreversible damage has taken place. Early symptoms may include pain and flushing at the time of injection, followed by nail bed pallor and a decreased capillary refill. Without an intervention at this point, the sequelae may progress to skin mottling, paresthaesia, motor weakness, and symptoms of compartment syndrome, which are ultimately followed by necrosis and gangrene [2]. In this patient, the early manifestations were not brought to the attention of hospital staff, soon enough to prevent lasting injury. The exact mechanism by which the damage is done is uncertain and it may differ from drug to drug; thus there is no universally accepted treatment protocol. Various medications which may be of use are classified into three groups: arterial vasodilators, thromboxane inhibitors, and high molecular weight dextrans [3]. In a 1987 study which involved an accidental arterial injection of crushed oral pentazocine in drug abusers, reserpine administration showed promising results by preventing both functional and tissue loss in all those who received this therapy within 15 hours [4]. This was not an option in our patient, as it had already been 48 hours since he was given the therapy; thus, anticoagulants were started, albeit, with no success and therefore, an amputation was the last resort.
Conclusion
Accidental IA injections have produced devastating effects on many patients’ lives. In our case, the patient had survived a major surgery for cancer of the oesophagus and was on regular follow-up. After the IA injection, he had to undergo amputation of the right hand and face lifelong morbidity and dependency. Although the technique of IV cannulation is routinely done by health care professionals, paying attention to details is a must, to avoid IA injections, no matter how experienced one is. Such vigilance has the potential to decrease the incidence of such cases and thus, prevent the morbidity which is associated with unintentional IA injection.
Recommendation
Always be careful when inserting an I.V line. Specific signs of IA cannulation include pulsatile movement of blood in the IV line, intense pain or burning at the site of injection, blood that is bright-red in appearance and cannulation in an area where an artery is in close proximity to a vein. In case of an inadvertent IA injection, follow administration of anticoagulants, arterial vasodilators, and sympatholytics and elevation of the affected extremity.
[1]. Patil MB, Patil SM, Accidental intra-arterial injection of adenosine in a child with supraventricular tachycardiaIran J Pediatr 2013 23(3):368-69. [Google Scholar]
[2]. Sen S, Chini EN, Brown MJ, Complications after unintentional intra-arterial injection of drugs: Risks, outcomes, and management strategiesMayo Clin Proc 2005 80(6):783-95. [Google Scholar]
[3]. Ghouri AF, Mading W, Prabaker K, Accidental intraarterial drug injections via intravascular catheters placed on the dorsum of the handAnesth Analg 2002 95:487-91. [Google Scholar]
[4]. Stueber K, The treatment of intraarterial pentazocine injection injuries with intraarterial reserpineAnn Plast Surg 1987 18(1):41-46. [Google Scholar]