Persistent Mullerian Duct Syndrome with Transverse Testicular Ectopia: Rare Entity
Deepika1, Abhay Kumar2
1 Consultant Surgeon, Department of General Surgery, Kurji Holy Family Hospital, Kurji, Patna, Bihar, and Visiting Consultant, Bihar Institute of Gastroenterology Yogipur, Kankarbagh, Patna, Bihar, India.
2 Consultant Laparoscopic and General Surgeon, Department of Minimal Access Surgery, Bihar Institute of Gastroenterology, Yogipur, Kankarbagh, Patna, Bihar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepika, Consultant Surgeon, Department of General Surgery, Kurji Holy Family Hospital, Kurji, Patna- 800010, Bihar, India.
Phone: 9431044498,
E-mail: deepikadoc@yahoo.com
We are reporting on a 35-year-old male from low socio-economic strata, who presented with a left-sided inguinal hernia. Intraoperatively, a uterus and two fallopian tubes were found in the hernial sac which was adjacent to the two gonads, which received their blood supply partly, along with Mullerian duct remnants (Persitent Mullerian duct Syndrome with Transverse testicular ectopia). The gonads were testes by histological examination, with features of degeneration and fibrosis. Complete excision of the mass was done and mesh hernioplasty was done.The diagnosis of persistent Mullerian duct syndrome with Transverse testicular ectopia was confirmed. Persistent Mullerian duct Syndrome is a rare entity and itís association with Transverse testicular ectopia is even more rare.
Persistent mullerian duct syndrome (PMDS), Inguinal hernia, Hernioplasty, Transverse testicular ectopia
Case Report
A 35-year-old male presented with left inguinal hernia. The hernia was present since his early childhood. There was complaints of some dragging discomfort on left side. During physical examination, complete left inguinal hernia was found. On gentle taxis, it was found to be completely reducible, with an empty scrotal sac. On right side of scrotum, testis was not present. General routine laboratory investigations done were not significant and they revealed only mild eosinophilia, for which he was treated with Hetrazan. Past medical history included excision of Lipoma over back (which was performed in 2001) and primary infertility. Since patient was only concerned with repair of left inguinal hernia and as he belonged to low socio- economic strata, investigations with regards to infertility were not carried out further.
Operative Findings
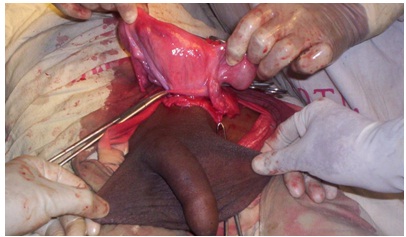
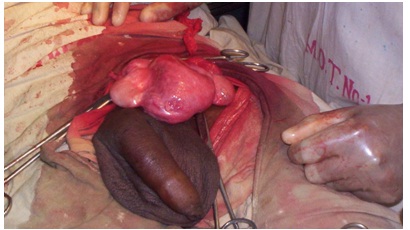
Through left inguinal oblique incision approach, hernia was addressed. On opening of sac, a small sized uterus with fallopian tubes on both sides and testes like structures on both sides of uterus were found [Table/Fig-1,2and3]. Since it was not possible to remove only uterus, after taking separate consent from patient’s attendant, uterus along with testis was removed and prolene mesh hernioplsty was done.

Discussion
Persistent mullerian duct syndrome (PMDS) was first described by Nilson [1]. First description of transverse testicular ectopia was made by Lenhossek in 1886. Jordan described syndrome of transverse testicular ectopia with persistent Mullerian ducts [2].
Persistent mullerian duct syndrome (PMDS) with Transverse testicular Ectopia is a rare entity of internal male pseudohermaphroditism, which is caused by a deficiency of mullerian-inhibiting factor (MIF). Mullerian derivatives (i.e. fallopian tubes, uterus, upper part of the vagina) are present in otherwise normally virilized XY patients, with both the testes to one side [3].
PMDS is a rare condition, with only about 150 cases being described in the literature. In transverse testicular ectopia, the ectopic testis may lie at internal ring, in the scrotum. Since it’s first description was made, more then 100 cases have been reported [4]. Among all reported cases, the oldest and youngest patients were 77 years and 3 days old, respectively [5]. A majority of cases which have been reported, belongs to paediatric and adolescent age groups [6].
PMDS patients are both karyotypically and phenotypically male, with normal development of secondary sex characteristics. In a human foetus, both mullerian and wolffian ducts are present at 7 weeks of gestation. Mullerian ducts and wolffian ducts are the anlagens of the female and male reproductive tracts, respectively. In an XY foetus, the testis differentiates by the end of the 7th gestational week. Sertoli cells begin to secrete MIF, which is responsible for the regression of the mullerian ducts. Normal sex differentiation in males is controlled by testosterone and MIF, both of which are produced by the foetal testes. Testosterone has a direct local effect on the wolffian ducts, including differentiation into the epididymides, vas deferens, and seminal vesicles. Formation of the urogenital sinus and male external genitalia requires in situ conversion of testosterone into dihydrotestosterone. PMDS patients develop both wolffian and mullerian structures due to deficiency of MIF. The gene which is responsible for MIF is localized on the short arm of chromosome 19. An autosomal mode of inheritance for PMDS has been described by gene mapping [7].
In literature, two anatomic varients of PMDS have been described. The most common variant (male form) ( 80% - 90% of cases ) is characterized by -unilateral cryptorchidism with contralateral inguinal hernia. The second anatomic variant (Female form) is rare [8,9].
As in other patients with undescended testes, an increased risk of malignant transformation of gonads has been found in PMDS, with transverse testicular ectopia. Overall, there is approximately an 18% incidence of malignant transformation of gonads in transverse testicular ectopia [10]. It has been found that patients with transverse testicular ectopia also present with some other genitourinary anomalies. Based on these associated anomalies, following classification of transverse testicular ectopia has been described [10].
Type I - Accompanied only by inguinal hernia (40-50%); Type II - Accompanied by persistent Mullerian duct syndrome (30%) Type III -Associated with genitourinary anomalies, other than persistent Mullerian duct, (13-20%): hypospadias, pseudohermaphroditism, seminal vesicle cysts, scrotal abnormalities, common deferent duct, horseshoe kidney. The management of PMDS with transverse testicular ectopia is controversial. Most clinicians recommend that the persistent mullerian derivatives be removed. On the other hand, the vas deferens lies close to the uterus and it may be incorporated into the vaginal wall, so that complete excision of these structures will divide the vas deferens. Surgical techniques for preserving the vas deferens have been described. Mobilization of the gonadal blood vessels may be necessary for completion of the orchiopexies. Repair of the inguinal hernia must be performed, if it is applicable. Orchidectomy should be performed for any testis that cannot be mobilized into a palpable position or if there are possible chances of PMDS turning into a malignancy. Because PMDS may be discovered incidentally during paediatric surgeries done for undescended testes or inguinal hernia, the initial procedure may need to include replacement of the gonads and mullerian structures within the pelvis and repair of the inguinal hernia. After confirmation of the diagnosis of PMDS, a definitive surgery should be performed to remove the corpus of the uterus and fallopian tubes, to enable fixation of the testes in the scrotum. The patient or his family should be completely informed about the diagnosis, the surgical options, and the need of long-term follow-up [11].
The patient in this case was older and orchidopexy was practically not possible, So, complete removal and hernioplasty were done. Patient made a good recovery. This case is unique in terms of the patient’s advanced age at presentation. The older age of presentation may be due to unawareness / non-significant symptoms.
[1]. Nilson O, Hernis uteris inguinalis beim manneActa Chir Scand 1939 83:231-9. [Google Scholar]
[2]. Martin EL, Bennett AH, Cromie WJ, Persistent Müllerian duct syndrome with transverse testicular ectopia and spermatogenesisJ Urol 1992 147:1615-7. [Google Scholar]
[3]. Odi TO, Abdur-Rahman LO, Nasir AA, Persistent Mullerian duct syndrome: A case report and review of the literatureAfr J Paediatr Surg. [serial online] 2010 [cited 2013 Nov 21];7:191-3.http://www.afrjpaedsurg.org/text.asp?2010/7/3/191/70425 [Google Scholar]
[4]. Moslemi MK, Ebadzadeh MR, Al-Mousawi S, Transverse testicular ectopia, a case report and review of literatureGer Med Sci 2011 9Doc15. doi: 10.3205/000138. Epub 2011 Jul 7 [Google Scholar]
[5]. Rasool Naima, Safdar C. Aqeel, Ahmad Asrar, Kanwal Shehla, Boota Mohammad, Transverse testicular ectopia with persistent mullerian duct syndrome: A case reportPakistan Armed Forces Medical Journal June 2012 2http://www.pafmj.org/showdetails.php?id=220&t=c [Google Scholar]
[6]. Akdemir Alp Özgür, Transverse Testicular Ectopia in an Adult Male; A Rare Form of Persistent Mullerian Duct Syndrome: A Case Report . Department of Urology II Clinic of Ankara Numune Education and Research Hospital, Ankara, TurkeyJ Clin Anal Med 2013 4(2):143-5.http://www.jcam.com.tr/files/KATD-627.pdf [Google Scholar]
[7]. Renu Divya, Rao B Ganesh, Ranganath K, Namitha , Persistent mullerian duct syndromeIndian J Radiol Imaging 2010 February 20(1):72-74.doi: 10.4103/0971-3026.59761 [Google Scholar]
[8]. Dekker HM, de Jong IJ, Sanders J, Wolf RF, Persistent mullerian duct syndromeRadiographics 2003 23:309-13.[PubMed] [Google Scholar]
[9]. Clemente A, Macchi V, Berretta M, Morra A, Female form of persistent müllerian duct syndrome: MDCT findingsClin Imaging 2008 32:314-7.[PubMed] [Google Scholar]
[10]. Moslemi , Transverse testicular ectopia, a case report and review of literatureGMS German Medical Science 2011 9ISSN 1612-3174 [Google Scholar]
[11]. Shamim Muhammad, Persistent Mullerian duct syndrome with transverse testicular ectopia presenting in an irreducible recurrent inguinal herniaJournal of Pakistan Medical Association August 2007 57(8):421-3. [Google Scholar]