Calcified Vocal Cord Nodule – A Unique Case Report
S Sundarapandian1, Revathy V Suresh2
1Assistant Professor, Department of Ear, Nose and Throat, Sree Balaji Medical Colllege and Hospital, Chennai, Tamil Nadu, India.
2Senior P.G Resident, Department of Ear, Nose and Throat, Sree Balaji Medical Colllege and Hospital, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. S. Sundara Pandian, No:7, CLC Works Road, Chromepet-44, Chennai, Tamil Nadu, India.
Phone: 9043331545,
E-mail: drsundarapandian@gmail.com
Vocal cord nodules are benign neoplastic lesions which occur due to submucosal oedema and haemorrhage, leading to fibrosis and hyalinization. Calcification in vocal cord nodules has not been reported so far in literature. It is thought to be a laryngeal counterpart of idiopathic calcinosis cutis. Here, we are reporting a case of a 38-year-old male patient who presented with a change in voice, which had a duration of one month. Laryngoscopic examination revealed a globular, yellowish white, sessile mass which arose from anterior commissure region of right vocal cord. Micro laryngeal excision was done. Histopathological examination was suggestive of a calcified nodule in vocal cord.
Calcification, Idiopathic calcinosis cutis
Case Report
A 38-year-old male patient presented to the Out-Patients Department (OPD) with complaints of change in voice and dry cough of one month’s duration. They were not associated with throat pain, dysphagia, post-nasal drips or any respiratory difficulty. The ear and nose examinations were normal. On doing indirect laryngoscopy and video laryngoscopic examinations, it was found that there was a globular, yellowish white, sessile mass which was about 1cm in diameter, which arose from the anterior commissure of right vocal cord, which did not move during respiration. Rest of vocal cord, larynx, and hypopharnyx were found to be normal. He was managed with complete voice rest and antibiotics for one week, with no improvement of symptoms. Therefore, patient was planned for Micro Laryngeal Excision and Biopsy.
Under general anaesthesia, patient was under taken for micro laryngeal excision and biopsy. A hard, greyish white mass was excised from right vocal cord, from near the anterior commisure, by using micro laryngeal scissors. Care was taken to maintain the mucosal integrity of vocal cord and mass was sent for a histopathological examination [Table/Fig-1].
On haematoxylin eosin staining, the microscopic section showed stratified, squamous epithelium overlying stroma, which contained sub epidermal collection of calcium deposits which were seen in dark blue stains. Post-operatively, serum free calcium, parathormone and calcitonin levels were studied and they were found to be normal. Patient was followed up for a period of 6 months. He was symptom free and laryngoscopic examination revealed normal vocal cords [Table/Fig-2].
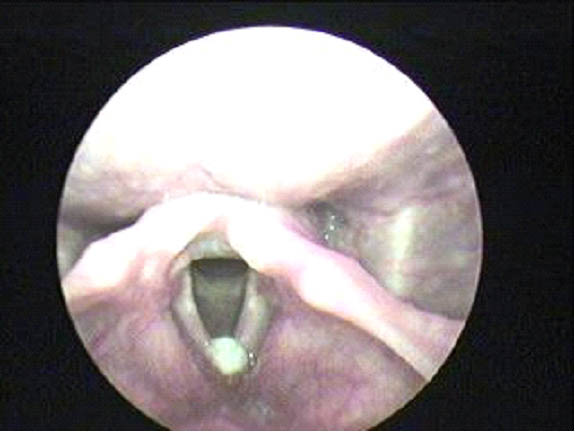
Video Layngoscopic Picture. Video laryngoscopic picture showed 1 cm diameter globular dirty white sessile mass seen arising from the anterior commisure area of right vocal cord not moving during respiration and rest of the vocal cord appears normal
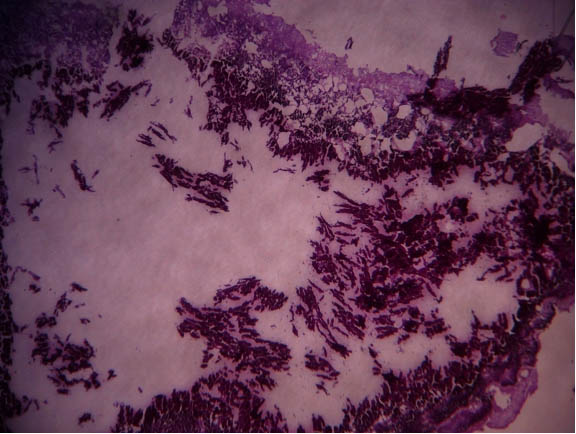
Histopathological Slide. Histopathological report showing stratified squamous epithelium overlying stroma which contains specs of calcium crystals suggestive of calcified vocal cord nodule
Discussion
Vocal cord nodules are more commonly found in young women and in people who routinely stress their vocal cords (singers, auctioneers, hecklers). Vocal cord nodules are initially oedematous, with a myxoid stroma, but they will become fibrotic with time. Vascular proliferation may be seen with dilated vessels, granulation tissue and haemorrhage [1] . In our case , patient was a carpenter by occupation and there was no history of vocal abuse.
The subepidermal calcified nodule, also known as cutaneous calculi, is a form of idiopathic calcinosis that affects children [2] . It occurs in facial skin usually and has no relationship with connective tissue disease or with any abnormality in calcium and phosphorous metabolisms. The oral cavity is very rarely affected by calcinosis cutis of any type. Two cases of calcified nodules were reported, one in gingiva of a 1-year-old girl and the other in the tongue of 5year old boy [2] . In our case, the patient was 38-year-old at the time of presentation and the site of involvement was vocal cord.
The sub epidermal calcified nodule presents as an asymptomatic, solitary, yellow-white or erythematous filiform tumour. The most common location is on the head and neck regions of male children [3] and a asymptomatic sub epidermal calcified nodule in a child’s sole has also been reported [4] .
Calcified nodules have been reported in thyroid, lung, abdomen and brain. In our case, patient presented with a calcified nodule in vocal cord, but no reference regarding calcification of vocal cord nodule has been reported in literature so far. Calcification of soft tissue can be caused by vitamin K2 deficiency or by poor calcium absorption, due to a high calcium or vitamin D ratio. This can occur with or without a mineral imbalance. Abnormalities in calcium-phosphate balance develop early in the course of chronic kidney disease [5] .
A variety of factors can cause this condition; the most common cause is dystrophic calcification which occurs in soft tissue as a response to injury, inflammation, infection, tumours, diseases of connective tissue, hypocalcaemia, hyperphosphataemia. The causes and histiogenesis of these deposits have not been fully established, but the most favoured theory is that calcium is deposited in a preexisting lesion. The treatment of choice is surgical removal, with a histopathologic examination [2] .
In idiopathic cutaneous calcinosis, histopathologic examination reveals a focal papillary dermal collection of dark blue –staining, large amorphous deposits and or small calcified globules which are surrounded by a lymphohistiocytic infilterate [3] .The causes of histiogenesis of these deposits have not been fully established, but most favoured theory is that calcium is deposited on a pre-existing lesion. In our case, on histopathological examination, the section showed stratified, squamous epithelium overlying stroma, which contained sub-epidermal collection of calcium deposits which were seen in dark blue stains.
Due to the rarity of its site, we consider this case to be unique and special attention should be given to calcification of vocal cord nodules among other benign neoplastic lesions of vocal cord.
Conclusion
This case has been reported because there is no substantial literature which has revealed calcification which occurred in vocal cord. Therefore, our case is unique in showing an unusual site of involvement.
A calcified vocal cord nodule has to be considered as a differential diagnosis for benign neoplastic lesions of vocal cord.
[1]. LDR Thomspon, LDR. Endocrine Pathology: Foundations in Diagnostic Pathology 2006; Philadelphia PAElsevier:9-13. [Google Scholar]
[2]. K Samir, Mofty El-, Cruz Daniel Santa, Mucosal Calcified nodule – The oral counterpart of the subepidermal calcified nodule, Oral SurgeryOral Medicine, Oral Pathology. [Google Scholar]
[3]. LA Juzych, CA Nordby, Subepidermal calcified nodulePeditric Dermatol 2001 18(3):238-40. [Google Scholar]
[4]. Lee Young Wool, Kim Byung Chul, Park Eun Joo, In Hoo KwonInternational Journal of Dermatology. 2012 5(3):316-20. [Google Scholar]
[5]. D Elbohy, M El-Hamamsy, M El-Sharkawy, Ranitidine and Omeprazole effect on Serum Phosphorous in Haemodialysis,International Journal of Pharma and Biosciences 2011 2(4):0975-6299. [Google Scholar]