Chondrosarcoma Arising in an Enchondroma of the Metacarpal Bone - A Case Report
Honnappa Sridhar1, Mysorekar Vijaya2, Wilfred Clement3, Chirukuri Srinivas4
1Assistant Professor, Department of Pathology, M.S. Ramaiah Medical College, India.
2Professor, Department of Pathology, M.S. Ramaiah Medical College, India.
3Assistant Professor, Department of Pathology, M.S. Ramaiah Medical College, India.
4Ex- Assistant Professor, Department of Orthopaedic Oncology,M.S. Ramaiah Medical College, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Honnappa Sridhar, Assistant Professor, Department of Pathology, M.S. Ramaiah Medical College, India.
Phone: 09742341871, 080-23605190,
E-mail: drsridhar24@rediffmail.com
Chondrosarcoma is a rare malignant tumour of proliferating cartilaginous tissue. It may arise as a primary lesion, or occur secondarily at the site of a previous benign lesion such as enchondroma . Primary chondrosarcomas are rare in the hand with a frequency of less than 0.5% to 3.2% of all chondrosarcomas, and are seen involving the phalanges, trapezium and trapezoid. Malignant transformation of a benign solitary enchondroma to secondary chondrosarcoma, especially in the hand, is extremely rare. We report a case, where the patient had developed a painful swelling in the 5th metacarpal bone of the right hand, 15 years back, which was diagnosed as enchondroma. Subsequently the patient presented with a 3-year history of increase in the size of the swelling at the same site, which on radiological and histopathological examination revealed malignant transformation into chondrosarcoma. We also discuss the differential diagnosis of chondrosarcoma. Keeping in mind the possibility of local recurrence and metastasis of chondrosarcoma, a ray amputation of the 4th and 5th digits of the right hand along with the mass was performed retaining the normal functioning of the hand.
Enchondroma, Chondrosarcoma, Metacarpal, Malignant transformation, Amputation
Introduction
Chondrosarcoma is a rare malignant tumour of bone, formed from cartilage. Enchondromas are the most common benign cartilaginous bone tumours arising in the medullary cavity of small bones of the hand. In contrast, chondrosarcomas commonly occur in the pelvis, proximal femur and humerus, but are uncommon in the small bones of the hand. Enchondromas rarely transform into chondrosarcomas. This transformation is seen more often in multiple enchondromatosis than in solitary lesions, but even this event is rare in the hands. Because limited surgical procedures like curettage, tend to lead to a high rate of recurrences, radical excision is recommended even in low-grade chondrosarcomas of the hand. Amputation of the affected finger or metacarpal is the correct surgical treatment. We report an unusual case of chondrosarcoma in the metacarpal bone, arising in a pre-existing enchondroma.
Case Report
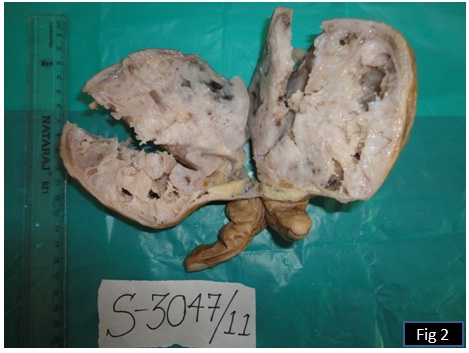
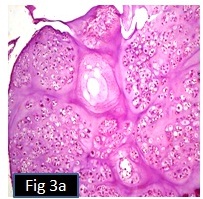
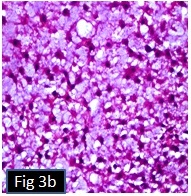
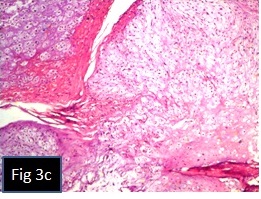
A 85-year-old male presented with swelling and pain in the 4th and 5th digits of the right hand[Table/Fig-1a] . Fifteen years back there was a small marble-sized swelling at the same site, which on radiographic examination was found to be lytic and was suspected to be an enchondroma. A wedge biopsy was done and histopathological examination had confirmed the diagnosis of enchondroma. The patient had refused further treatment. There was now a rapid increase in the size of the swelling at the same site, since the past 3 years. Radiography now showed a lytic lesion in the right 5th metacarpal bone, causing erosion of the 4th metacarpal bone along with bone expansion, cortical destruction and soft tissue extension [Table/Fig-1b] . A trucut biopsy from the swelling was done, which on histopathological examination was diagnosed as chondrosarcoma. Subsequently, ray amputation was performed, i.e, removal of the entire 4th and 5th fingers with their metacarpal bones along with the entire tumour, and subjected for histopathological examination. Grossly, the amputation specimen showed a globular mass measuring 9.5 x 8 x 7.5 cms, involving the 4th and 5th digits of the right hand. The cut surface of the mass was brown, myxoid, with gelatinous material. The tumour was well delineated with a variegated appearance with areas of cartilage [Table/Fig-2] . Microscopy revealed tumour tissue composed of cartilaginous matrix within which plump crowded tumour cells with hyperchromatic nuclei and a moderate degree of pleomorphism, were noted [Table/Fig-3a] . Mitoses were 0 to 2/10hpf. Interspersed areas also showed stellate cells in a myxoid matrix [Table/Fig-3b] . Permeation of bone with entrapment of the bony trabeculae within the tumour, was also noted [Table/Fig-3c] . In a focal area at the periphery of the tumour, a classic enchondromatous lesion with a preserved fibrous capsule was evident [Table/Fig-4] . A final diagnosis of chondrosarcoma with myxoid areas, arising in a preexisting enchondroma, was given. The ray amputation done did not significantly interfere with the function of the hand. Followup of the patient has been done for three years during which he is free of disease.
Swelling in the 4th and 5th digits of the right hand

X-ray showing a lytic lesion in the right 5th metacarpal bone, erosion of the 4th metacarpal with soft tissue extension

Globular mass in the 4th and 5th digits. Cut surface - brown, myxoid, with gelatinous material
Cartilaginous matrix with plump crowded, hyperchromatic tumour cells (x100, H&E)
Stellate cells in a myxoid matrix (x200, H&E)
Permeation of bone with entrapment of bony trabeculae (arrow) (x100, H&E)
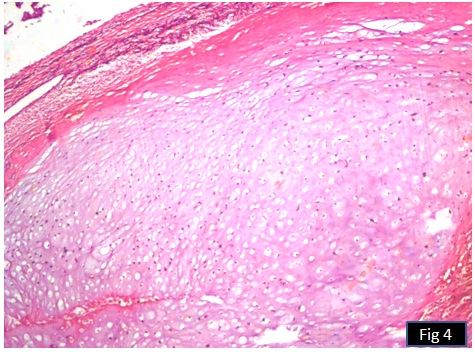
Focal area of enchondromatous lesion with preserved fibrous capsule (x100, H&E)
Discussion
Chondrosarcoma is a malignant tumour of proliferating cartilage tissue. It may arise as a primary lesion, or occur secondarily at the site of a previous benign lesion such as enchondroma or osteochondroma[1] . Chondrosarcomas constitute about 10% of primary malignant bone tumours with a peak incidence in the fifth and sixth decades of life. The male to female ratio is 3:1 [2] . They can occur in any location, however majority are located in the trunk, pelvis and proximal femur and humerus [1]. Conventional chondrosarcomas based on their location, are categorized into primary central chondrosarcomas (85%) and secondary peripheral chondrosarcomas (15%) [3] . Distinction between enchondroma and chondrosarcoma is a diagnostic dilemma, however radiological findings help to make a differential diagnosis [4] . Chondrosarcoma involving the metacarpal bone in the hand is a highly aggressive lesion. Painful swelling for a long period in the aged, cortical irregular thickening, disruption and soft tissue expansion are useful signs for diagnosis of chondrosarcoma [5] . Primary chondrosarcomas are rare in the hand with a frequency of less than 1.5% to 3.2% of all chondrosarcomas [6] . In the hand, chondrosarcomas are noted in the phalanges, metacarpals, trapezium and trapezoid [1] . Metacarpal involvement is still rarer [7] .
Enchondromas are benign cartilaginous tumours that present in small bones of the hands and feet. Malignant transformation of a benign solitary enchondroma to secondary chondrosarcoma, especially in the hand, is extremely rare. There are very such few cases published in literature [6] . Our patient had a painful swelling for 15 years at the little finger of the right hand that on histological examination was diagnosed as an enchondroma without any malignant features, for which he did not seek any medical treatment. This case is unique since it is a longstanding solitary enchondroma located at the right metacarpal bone, transforming into a chondrosarcoma, necessitating a ray amputation.
The differential diagnosis between a chondrosarcoma and chondroma rests on radiographic, architectural and cytologic features. Microscopically chondromas show mature lobules of hyaline cartilage with no evidence of atypical cells. Chondrosarcoma is differentiated from osteosarcoma by the lack of malignant osteoid. Chondromyxoid fibroma is an unusual benign cartilaginous tumour seen in small bones of the hands and feet.
Microscopically the tumour has a lobulated appearance in which myxochondroid islands are separated by intersecting bands of fibroblast-like spindle cells and osteoclasts [2] .
In a case similar to ours, reported by Wirbel and Remberger, a chondrosarcoma of the first metacarpal bone of the right hand, was radiographically interpreted initially as enchondroma and treated conventionally by curettage and bone grafting. After final histopathological examination it was diagnosed as chondrosarcoma for which wide resection of the metacarpal bone was done with reconstruction using corticocancellous bone graft and plate fixation to avoid local recurrence or metastasis [8] .
In another similar case reported by Demireli et al., a solitary enchondroma was located at the index finger of the right hand. Seven months later, the tumour recurred and was destructive, and amputation material was diagnosed as an intermediate grade chondrosarcoma arising secondary to the former solitary enchondroma. Wide excision of the tumour was done to avoid local recurrence or metastasis [4] .
Despite the low metastatic potential of chondrosarcomas of the hand in comparison with other sites, ray amputation of the mass is usually done as in our case, to avoid local recurrence or distant metastasis [4,9] .
Conclusion
Chondrosarcoma involving the hand is very rare. Moreover, very few cases of enchondroma transforming into a chondrosarcoma are documented in the literature. However, keeping this rare possibility in mind, excision of an enchondroma has to be done as soon as possible. Chondrosarcoma requires a prompt and more radical treatment than enchondroma. In addition to histopathological findings, a painful swelling in the hand for a long period in the aged, with cortical irregular thickening, destruction and soft tissue extension are useful signs for the diagnosis of chondrosarcoma. Wide excision is recommended to avoid local recurrence or metastasis.
[1]. S Chaudhary, D Singh, R Sen, Chondrosarcoma of Distal Radius- A case report and brief review of literature.Webmed Central Orthopaedics 2010 1(WMC001274):1-9. [Google Scholar]
[2]. J Rosai, LV Ackerman, Bones and Joints. In: Rosai J ed. Rosai and Ackerman’s Surgical Pathology, 2011 10th EditionMosby ElsevierSt. Louis:2013-104. [Google Scholar]
[3]. M Hatori, M Watanabe, H Kotake, Chondrosarcoma of the ring finger: A case report and review of the literature.Tohoku J Exp Med. 2006 208:275-81. [Google Scholar]
[4]. P Demireli, DK Cavdar, S Vural, GY Ovali, T Ozalp, Secondary chondrosarcoma arising from a solitary enchondroma at the index finger of the right hand- a case report.Turkish Journal of Pathology 2006 22:53-6. [Google Scholar]
[5]. H Gelderblom, PCW Hogendron, SD Dijkstra, CSV Rijswijk, AD Krol, The clinical approach towards chondrosarcoma.The Oncologis 2008 13:320-9. [Google Scholar]
[6]. PE Muller, HR Durr, A Nerlich, C Pellengahr, M Maier, Malignant transformation of a benign enchondroma of the hand to secondary chondrosarcoma with isolated pulmonary metastasisActa Chir Belg 2004 104:341-4. [Google Scholar]
[7]. KP Kavitha, MC Savithri, KC Ramani, D Puthoor, Periosteal chondrosarcoma of the metacarpal bone- Report of a rare entity.Australasian Medical Journal 2012 5(11):589-92. [Google Scholar]
[8]. RJ Wirbel, K Remberger, Conservative surgery for chondrosarcoma of the first metacarpal boneActa Orthopaedica Belgica. 1999 65:226-9. [Google Scholar]
[9]. T Gohla, VJ Schoonhoven, KJ Prommersberger, U Lanz, Chondrosarcomas of the hand.Handchir Mickrochir Plast Chir 2004 36:328-32. [Google Scholar]