Struma ovarii is uncommon tumor of ovary which can mimic as advanced carcinoma of ovary. Thyroid tissue is relatively frequent constituent of mature ovarian teratoma. Case of struma ovarii masquerading as cancer of ovary in a female aged 63 yrs showing complex large unilateral multilocular adnexal mass with elevated CA 125 (more than 1721 IU/L) and massive ascites mislead treating surgeons for long time. Clinicians were virtually clueless about preoperative diagnosis. Combination of ascites has been seen in one third cases but association with raised CA 125 is rare(only 8-10 cases so far). This case developed hypothyroidism one week after surgery.
Struma Ovarii, Ca-125, Ca Ovary, Ascites
Introduction
Struma ovarii, the most common type of monodermal mature teratoma, which is composed exclusively of thyroid tissue with associated ascites and elevated CA 125 levels, has rarely been reported ( only 8-10 cases have been reported so far) [1]. This tumour mimics a malignant ovarian neoplasm due to complex multilocular adnexal mass, ascites and high CA 125 levels [2]. Hence, pre-operative diagnosis is really very difficult to make and it leads to mental agony for patient as well. Diagnosis of struma ovarii can be made only on histopathology. Radiological findings, ascites and raised CA 125 levels make it a unique and highly suspicious case of malignancy [3]. This case has been presented here because surgeons had a very strong doubt that it was a malignancy prior to operation, based on clinical, radiological findings and raised CA125 levels, but frozen section report and finally, histopathology report proved that it was benign struma ovarii.
Germ cell tumours are derived from the primordial germ cells of the ovary and 20-25% of all benign and malignant ovarian neoplasms are of germ cell origin. Vast majority of these tumours are mature teratomas. Teratomas are composed of various tissues including hair, skin, bone, teeth, as well as thyroid tissue [4]. Struma ovarii is a rare monodermal variant of ovarian teratoma [5].
Case Report
A 63-year-old hypertensive, nondiabetic female (para1+0, attained menopause 23 years back) came to OPD with massive ascites and restlessness. Her vitals were normal. She was admitted and after preliminary treatment, was sent for imaging and tumour marker evaluation. She had massive ascites, few mesenteric nodules and big sized, multilocular, heterogeneously enhancing, adnexal mass on right side on CT, with CA 125 in range of 1,721 IU/L. CEA and CA 19.9 were normal. Her ascitic fluid was tapped and it was sent for cytology, which was reported to be negative for malignant cells. Radiological findings and raised CA 125 levels prompted surgeons to believe that it was a case of advanced CA ovary. Hence, total abdominal hysterectomy, B/l salpingo-oophorectomy, omentectomy and exploratory laparotomy were done. During operation, 4.5 L of ascitic fluid was drained out. Left ovary, although it was normal, was found to be adherent to sigmoid colon. Specimen was reported as struma ovarii- predominantly consisting of mature thyroid tissue on biopsy.It got reviewed elsewhere (USA) and was reported as same.
Her post-operative period was uneventful, except for development of hypothyroidism after 1 week of removal of struma ovarii. Free T3, T4 and TSH levels were 3.01 pg/ml, 0.897 ng/dl and 22.34 IU/ML respectively after one week of post-operative removal of struma ovarii. Pre-operative evaluation of thyroid could not be done due to lack of clinical suspicion and lack of any significant hyperthyroidism. She was discharged after ten days. Patient is reporting to us at 3 monthly intervals and is currently in good health.
Pathological Finding
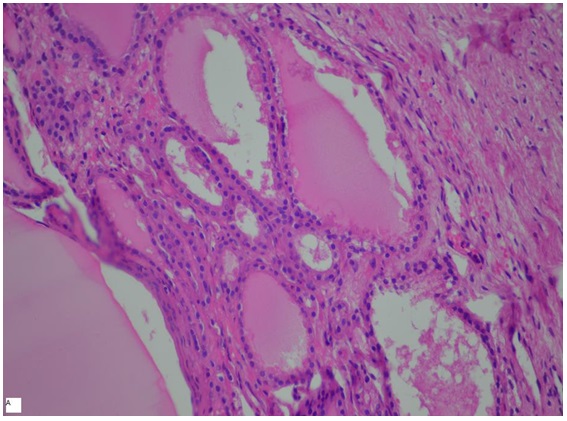
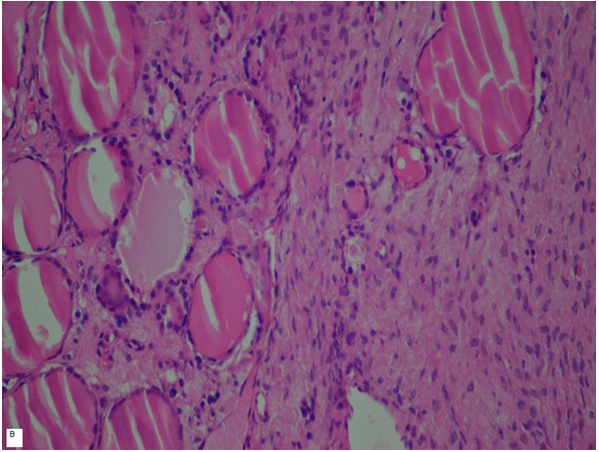
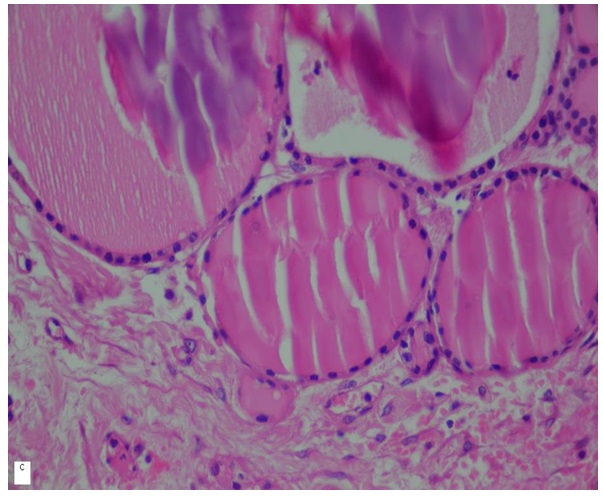
Gross examination of right side adnexal mass showed multinodular ovary measuring 10.5x9.5x4.5 cm, with attached fallopian tube measuring 8.5 cm in length. Cut section showed predominantly fleshy areas with greenish brown, solid and gelatinous cystic areas. Cystic areas measured 2.5x2.5 cm .Capsule was intact. Uterus and cervix were grossly unremarkable, except two intramural fibroids. Left ovary with attached tube measured 3x1.5x1.5cm and 3.5 cm respectively. Cut section of left ovary was unremarkable. Microscopic examination of right ovarian mass revealed mature cysticmonodermal teratoma which consisted of mainly thyroid follicles which were lined by single layered cuboidal epithelium which contained colloid [Table/Fig-1A,1B,1C] . Specimen was received for frozen section and it was reported as struma ovarii. Sections from left ovary, omentum and peritoneal tissues from right and left paracolic gutters and from under surface of diaphragm remained histologically unremarkable. Case was sent for second opinion to USA based lab and was reported as same. Post-operative CA- 125 levels became normal.
Photomicrograph of struma ovarii – clearly showing thyroidal acini lined with low cuboidal epithelium and filled with colloid along with ovarian stromal tissue
Photomicrograph of another section from ovary showing acini of thyroid gland along with ovarian stromal tissue
Photomicrograph showing struma ovarii- large follicles filled with colloid lined with cuboidal epithelium
Discussion
Struma ovarii is a rare form of germ cell tumour (1 % of all ovarian tumours and 2.7 % of all dermoid teratomas) of reproductive age group (its occurrence mostly peaks in 5 th to 6 th decades of life, but it is rare in pubertal females) which is composed predominantly of mature thyroid tissue (more than 50%). It is a benign condition, but a malignant change can occur in 1/3rd of cases.Patients usually present with abdominal pain, palpable mass, abnormal vaginal bleeding with ascites and hydrothorax [6].
Ascites is mainly transudative from tumour surface, which exceeds absorptive capacity of peritoneum or obstructs lymphatics due to tumour cells or increases permeability of the neovasculature with protein leakage and an inflammatory reaction.In literature review done on cases reported from 1996 to 2008, a total of eight cases of struma ovarii with pseudomeigs syndrome and elevated CA- 125 level with maximum volume of ascites ranging from 20,000 L (Huh et al., 2006) to few L and CA-125 ranging from 124.9 to more than 5218 IU/L(Mul et al., 2009) were reported. In our case, total ascitic fluid drained was 4.5 L and preop CA 125 level was 1721 IU/L. CA-125 is widely accepted tumour marker for ovarian cancer, but it increases in tumourous conditions of many organs like -breast, endometrium, intestine and lung, as well as in some non -malignant gynaecologic conditions also, thus indicating that there is a limit in clinical application of this tumour marker as an indicator of an ovarian malignancy. CA 125, as a tumour marker, was found to be elevated, mimicking ovarian carcinoma (only 8-10 cases have been reported so far for struma ovarii). Pre-operative evaluation with triple contrast CT /MRI [7] and increased uptake of radio-iodine 123 in ovary are pointers to diagnosis. Struma ovarii can be incidentally discovered during pelvic imaging. In a majority of cases final diagnosis comes from histopathologist desk only as surprise. On histopathology, brown to green brown, solid, cystic, mature thyroid tissue which is arranged in papillae or follicles, with acini which are lined with low cuboidal epithelium and lumen filled with colloid, are pointers to diagnosis. Doing immunohistochemistry with TSH antibody can also be useful for arriving at a diagnosis. Atypia, stromal sclerosis, hyperchromasia or nuclear features of papillary carcinoma of thyroid, capsular and vascular invasion indicate a transformation to malignancy.Malignant struma ovarii can turn into follicular carcinoma (resulting in peritoneal spread which is called peritoneal strumosis), papillary carcinoma or follicular/ microcarcinoma, which is a variant of papillary carcinoma (showing BRAF and RAS mutations), rarely with carcinoid and lymphoma also6.Struma ovarii can be incidentally discovered in association with mucinous cystadenoma or Brenner tumour, which are detected on radio iodine uptake studies [8].
Surgery is treatment of choice for benign tumours .Surgery, along with radioiodine I-131 as adjuvant, can be given for metastatic and recurrent tumours. Thyroglobulin is preferred tumour marker postoperatively, to monitor recurrence. Although tumour is composed predominantly of thyroid tissue, thyrotoxicosis is reported in only 5% of the cases. Prognosis is excellent in benign form of disease.
Conclusion
Elevated tumour markers in a post -menopausal woman who presents with a multilocular adnexal mass and ascites can be interpreted as highly suggestive of a malignancy. The diagnosis is usually made postoperatively by the pathologists.Struma ovarii should be included in differential diagnoses of pelvic masses in aforementioned clinical scenario.
Abbreviations
CT-Computerised Tomography, CA125-carbohydrate antigen 125OPD- out patient department, TSH-Thyroid stimulating hormoneMRI- magnetic resonance imaging.
Acknowledgement
I acknowledge MRD department of Action Cancer Hospital, Delhi for providing me all necessary documents and file related to this case.
[1]. S Mitrou, S Manek, S Kehoe, Cystic struma ovarii presenting as pseudomeigs syndrome with elevated CA-125 level.A case report and review of the literature.Int J Gynaecol Cancer18(2):372-75. [Google Scholar]
[2]. MP Mui, KF Tam, FK Tam, HY Ngan, Coexistence of struma ovarii with marked ascites and elevated CA-125 levels: case report and literature review.Arch Gynecol Obstet May 2009 279(5):753-7. [Google Scholar]
[3]. PH Williemse, JW Oosterhuis, JG Alders, DA Piers, DT Sleijfer, A Vermay, Malignant struma ovarii treated with ovariectomy, thyroidectomy and I 131 administration.Cancer 1987 60(2) [Google Scholar]
[4]. LM Roth, A Talerman, Knowledge of staff nurses regarding legal and ethical responsibilities in the field of psychiatric nursing.Pathology Feb 2007 39(1):139-46. [Google Scholar]
[5]. A Bal, H Mohan, SB Singh, A Sehgal, Malignant transformation in mature cystic teratoma of the ovary: report of five cases and review of the literature.Arch Gynecol Obstet. Mar 2007 275(3):179-82. [Google Scholar]
[6]. SC Yoo, KH Chang, MO Lyu, SJ Chang, HS Ryu, HS Kim, Clinical characteristics of struma ovarii.J Gynecol Oncol Jun 2008 19(2):135-8. [Google Scholar]
[7]. R Shaco-Levy, RY Peng, MJ Snyder, GW Osmond, E Veras, SM Bean, Malignant struma ovarii: a blinded study of 86 cases assessing which histologic features correlate with aggressive clinical behavior.Arch Pathol Lab Med. Feb 2012 136(2):172-8. [Google Scholar]
[8]. D Utsunomiya, S Shiraishi, K Kawanaka, Struma ovarii coexisting with mucinous cystadenoma detected by radioactive iodineClin Nuc Med 2003 28(9):725-7. [Google Scholar]