Sclerosing Lobular Hyperplasia- Correlation between Cytomorphological and Histological Findings
Rachna Lamichaney1, Mingma Sherpa2, Diwakar Pradhan3
1Assistant Professor, Department of Pathology, Sikkim Manipal Institute of Medical Sciences, Sikkim, India.
2Assistant Professor, Department of Pathology, Sikkim Manipal Institute of Medical Sciences, Sikkim, India.
3Junior Resident, Department of Pathology, Sikkim Manipal Institute of Medical Sciences, Sikkim, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rachna Lamichaney, Assistant Professor, Department of Pathology, Sikkim Manipal Institute of Medical Sciences, Sikkim, India.
Phone: 9002446517,
E-mail: creation_rl@hotmail.com
Sclerosing lobular hyperplasia of the mammary gland is an uncommmon benign lesion which is mainly seen in adolescents and young women. The breast lobules are enlarged due to ductal and acinar proliferations but they have normal architecture. There is extensive fibrosis of the intralobular stroma, and to a lesser degree, of the interlobular parenchyma. Patients generally complain of a palpable, painless/slightly tender and well-defined lump in breast. Fine-needle aspiration cytology of sclerosing lobular hyperplasia is non diagnostic with features similar to fibroadneoma except for the absence of stromal fragments. In order to reach a definitive diagnosis, a histopathologic evaluation is needed. However, a distinction between the two benign entities is of no clinical significance.We are describing a case of sclerosing lobular hyperplasia that occurred in the left breast of a 26-year-old lady.
Sclerosing lobular hyperplasia, Fibroadenoma, Fine needle aspiration cytology
Case Report
A 26-year-old lady presented with a painless lump in the left breast. On examination, the lump was found to be firm, freely mobile and was approximately 5 x 3 cms in size. The overlying skin was unremarkable. There were no palable lymph nodes and no relevant family or personal history. Clinicoradiological diagnosis of fibroadenoma was further supported by FNAC. Eventually, left lumpectomy was performed.
Pathological Finding
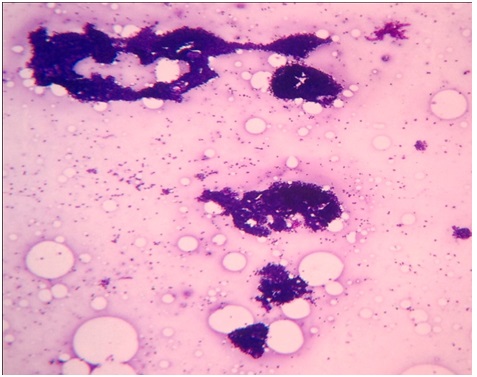
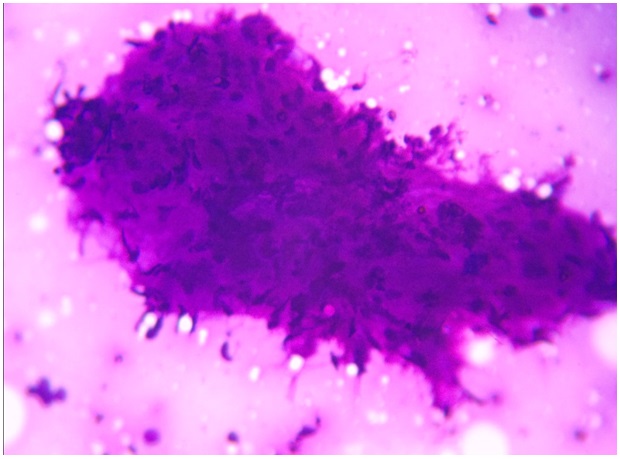
Fine needle aspiration cytology revealed cellular smears comprising of small and large clusters of bland ductal epithelial cells and myoepithelial cells, as shown in [Table/Fig-1]. Few stromal fragments were noted [Table/Fig-2]. Background was relatively clean, with few bare nuclei. The ductal epithelial cells had round to oval nuclei with dispersed chromatin and scant basophilic cytoplasm. Keeping these in mind, a cytological diagnosis of fibroadenoma was made. However, many a times, fibroadenomas can be confused with other breast lesions like phyllodes tumour. Phyllodes tumour shows hypercellular stromal fragments and large number of dissociated stromal cells as compared to fibroadenoma.
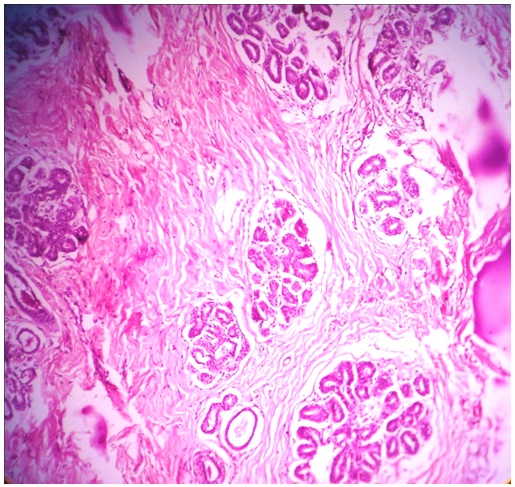
The resected specimens received were two, soft to firm, greyish white tissues which measured 4.5x2x1.5 cm and 1.5x1 x 0.5 cm in size. Histology revealed multiple large lobules showing proliferation of ductules and acini along with sclerosis of the intervening stroma [Table/Fig-3]. Large areas of stroma with keloid like sclerosis were also noted. A final diagnosis of sclerosing lobular hyperplasia was made.
Small and large clusters of bland ductal epithelial cells and myoepithelial cells.Background shows few bare nuclei (H&E X100)
Stromal fragment (H&E X 400)
Multiple large lobules showing proliferation of ductules and acini along with sclerosis of the intervening stroma (H&E X 100)
Discussion
The basic structural unit of the female breast is a lobule, which consists of a varying number of acini. In lobular hyperplasia, there is an increase in the number of acini within the lobules. Besides lobular hyperplasia, sclerosis of the intralobular and interlobular stroma characterizes the entity of “sclerosing lobular hyperplasia”. Sclerosing lobular hyperplasia is an infrequently encountered benign proliferative lesion of the breast and it was first described by Kovi et al., [1]. It most commonly occurs within the age group of 14 and 46 years [1]. It usually presents as a discrete, palpable, and painless mass in the upper outer quadrant of the breast. Mammography reveals a lobular or oval, well-circumscribed mass with echogenic septa, that correspond to interlobular sclerosis [2].
Fine-needle aspiration cytology findings which were previously reported in two cases of sclerosing lobular hyperplasia [3,4] emphasized the presence of ductal epithelial cells in monolayered sheets and round acinar clusters in a clean background which was devoid of stromal fragmants and few bare nuclei. In our case, the findings were similar, but for the presence of few stromal fragments, which were similar to the findings of Kapur P et al., [5].The sclerosed stroma may make fine-needle aspiration a difficult task and it may also account for the relative paucity of stromal fragments. However, a complete absence of stromal fragments and rarity of bare nuclei are not consistent features of sclerosing lobular hyperplasia and they cannot not be relied upon to distinguish it from fibroadenoma. Grossly, the specimen that we received was greyish white, firm, which was same as seen in other reported cases.
Histologically, there are enlarged lobules with increased numbers of acini. The intralobular stroma is collagenized, with loss of stromal mucopolysaccharides, and there is variable sclerosis of the interlobular stroma [1,6]. The lobular acini and ducts have distinct single-layered epithelial and myoepithelial components. Like all the cases of sclerosing lobular hyperplasia the histological findings of our case were also similar.
It is distinguished from fibroadenoma histologically by preservation of the acinar architecture, despite the hyperplastic appearance which is caused by an increased number of acini per lobule and increased collagenized intralobular and interlobular stroma.
Fibroadenomas, on the other hand, have irregular proliferating elongated and distorted ducts and loose cellular stroma [6].
The natural course of sclerosing lobular hyperplasia is not known. However, till date, no association with or a natural progression towards malignancy has been reported. Excision of the lesion is considered as adequate therapy. Recurrences have not been documented[7].
Conclusion
We have described cytologic and histologic features of sclerosing lobular hyperplasia, breast seen in a young lady. We wish to emphasize that sclerosing lobular hyperplasia can be easily mistaken for fibroadenoma in fine needle aspiration smears. For making a definitive diagnosis, histological studies are required. However, the difference is of no clinical significance, since the two lesions have similar clinical behaviours and both need surgical interventions.
[1]. J Kovi, HB Chu, LD Leffall, Jr. Sclerosing lobular hyperplasia manifesting as a palpable mass of the breast in young black women.Hum Pathol. 1984 15:336-40. [Google Scholar]
[2]. TB Poulton, ES de Paredes, M Baldwin, Sclerosing lobular hyperplasia of the breast: imaging features in 15 cases.AJR Am J Roentgenol. 1995 165:291-94. [Google Scholar]
[3]. M Jain, VK Arora, N Singh, A Bhatia, Fine needle aspiration cytology of sclerosing lobular hyperplasia of the breast: a case reportActa Cytol. 2001 45:765-67. [Google Scholar]
[4]. N Panikar, S Agarwal, Sclerosing lobular hyperplasia of the breast: fine-needle aspiration cytology findings – a case reportDiagn Cytopathol 2004 31:340-41.doi: 10.1002/dc.20135 [Google Scholar]
[5]. P Kapur, D Rakheja, Cavuoti Dominick C, Johnson-Welch Sarah F, Sclerosing lobular hyperplasia of breast: cytomorphological and histomorphological features: a case report.Cytojournal. 2006 3(8)doi: 10.1186/1742-6413-3-8. [Google Scholar]
[6]. PP Rosen, neoplasm Fibroepithelial, In: Rosen PP, editor. Rosen’s Breast Pathology 2001 Philadelphia:Lippincott Williams and Wilkins:163-70. [Google Scholar]
[7]. M Kamal, Aj Evans, H Denley, SE Pinder, IO Ellis, Fibroadenomatoid hyperplasia: a cause of suspicious microcalcification on mammographic screeningAJR Am J Roentgenol 1998 171:1331-34. [Google Scholar]