Nasal Discharge Cytology an Important Diagnostic Method for Allergic Fungal Sinusitis: Report of Three Cases
Sharada Raju Rane1, Nalini Vinayak Kadgi2, Sonal Ashok Agrawal3, Anita Neelkanth Kavatkar4
1Associate Professor, FICP, Department of Pathology,Byramjee Jeejeebhoy Government Medical College, Pune, India.
2Assistant Professor, Department of Pathology,Byramjee Jeejeebhoy Government Medical College, Pune, India.
3Ex-Student, Department of Pathology,Byramjee Jeejeebhoy Government Medical College, Pune, India.
4Associate Professor, Department of Pathology,Byramjee Jeejeebhoy Government Medical College, Pune, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nalini Vinayak Kadgi, B-403, Nancy Lake Homes, Opposite Bharati Vidyapeeth, Pune – Satara Road, Katraj, Pune-411046, India.
Phone: 091- 9881690690,
E-mail: nalini.kadgi@gmail.com
Allergic fungal sinusitis (AFS) is a distinct clinicopathological entity. It occurs in immunocompetent individuals with history of atopy, increased IgE levels and peripheral eosinophilia and causes noninvasive pansinusitis. It is histologically characterised by the presence of ‘allergic mucin’ with clusters of eosinophils, charcot – Leyden crystals and scattered fungal hyphae. AFS is an immunological reaction to fungal deposits. As AFS is noninvasive, fungal hyphae can be demonstrated in nasal secretions on cytology. Etiological agent of AFS is Aspergillus or pigmented dematiaceous family. Special stains are helpful for identification. We came across three cases of age group ranging from 26 to 60-year of recurrent rhinitis with nasal discharge. The nasal secretions were collected by nasal swabs onto the glass slide and stained with Giemsa and silver stains. Smears revealed fungal hyphae amidst inflammatory cells with occasional Charcot-Leyden crystals. Nasal secretion cytology plays an important role in diagnosis and can be used for preoperative as well as intraoperative diagnosis of AFS and can be used as an additional diagnostic tool.
Fungal hyphae, Allergic mucin, Charcot – Leyden crystals
Case Report
Case 1
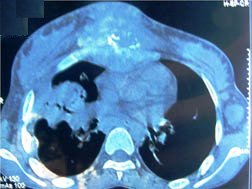
A 27-year-old female presented with right nasal discharge , nasal blockage, right sided recurrent headache and progressive proptosis since 2 years. The differential diagnosis on clinical examination was Pansinus polyp / Allergic fungal sinusitis. CT scan revealed inflammatory soft tissue swelling involving right maxillary, right ethmoid, right frontal air cells and sphenoid sinus with extension into the nasopharynx with hyperdensity and proptosis.
Case 2
A 26-year-old female presented with recurrent rhinitis and left nasal obstruction, change in voice since 6 weeks. The clinical diagnosis was a sinonasal polyp in this case. CT scan revealed large heterogenous density with sinonasal mass lesion extending into the left frontal bone. The differential diagnosis on CT scan were malignancy, olfactory neuroblastoma, sarcoma.
Case 3
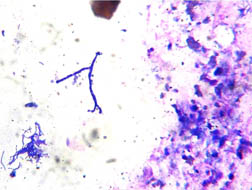
A 60-year-old female presented with nasal bleeding with foul smelling discharge and nasal twang. The clinical diagnosis in this case was a maxillary sinus polyp [Table/Fig-1]. CT scan revealed soft tissue mass involving maxillary sinus with palatal perforation. on clinical examination nothing significant was found but the anterior and posterior rhinoscopy in all the cases revealed polyps in nostrils extending into nasopharynx. The third case also revealed palatal perforation. Routine investigations performed revealed eosinophilia, the rest of the haematological, biochemical and serological profiles were within the normal limits. All the patients were tested for HIV and were negative. Nasal swabs were taken from both the nostrils and were immediately rolled onto the glass slides. Smears were air dried and stained with May Grunwald – Giemsa (MGG)[Table/Fig-2] and silver methanamine stain. The nasal discharge cytology showed groups of acute inflammatory cell collections with few scattered fungal hyphae showing dichotomous branching and septation [Table/Fig-3]. Occasional Charcot – Leyden crystals were also noted. Eosinophils were not seen on cytology [Table/Fig-4]. Culture was tried on nasal discharge cytology but no growth was seen as the number of hyphae were few. Silver Stain highlighted the septation of the fungal hyphae [Table/Fig-5]. All the cases were confirmed on histology. As the tissue was put in 10% formalin, culture was not done so further typing of fungus was not possible. Fungal spore assessment was not done.
CT scan of paranasal sinuses showing soft tissue mass involving left maxillary sinus, left nasal cavity with nasopharyngeal extension and bony destruction.
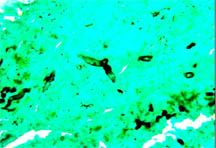
Inflammatory cell collections with stained fungal hyphae , MGG stain (400 X )
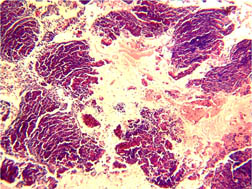
Thick masses of mixed inflammatory infiltrate with clusters of eosinophils with laminated histology. H and E stain ( 100 X )
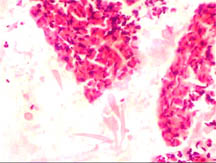
Charcot – Leyden crystals against a background of allergic mucin with clumps of eosinophils. Eosinophilic masses with Charcot – Leyden crystals , H and E stain(400X)
Thin filamentous fungal hyphae showing branching, Silver Methanamine stain (400 X)
Discussion
Allergic Fungal Sinusitis (AFS) is a distinct clinicopathological entity. It was described by Millar et al., in Great Britain and Katzenstein et al., in the United States. It is a relatively new and incompletely understood clinical entity with characteristic clinical, radiographic and histopathologic findings. Recognition and understanding of this unique disease will lead to efficient diagnosis and treatment of this curable process [1]. It occurs in immunocompetent individuals and causes noninvasive pansinusitis [2]. It is histologically characterised by the presence of ‘allergic mucin’ with clusters of eosinophils and Charcot – Leyden crystals and scattered fungal hyphae [3,4]. As AFS is noninvasive , fungal hyphae can be demonstrated in nasal secretions. AFS is an immunological reaction to fungal deposits [5]. It occurs in young people with equal incidence in males and females. It is noninvasive and occurs unilaterally. Etiological agent of AFS is Aspergillus or pigmented dematiaceous family members like Bipolaris, Curvularia, etc, [2]. This fungus is seen in immunocompetent patients with history of atopy, increased IgE levels and peripheral eosinophilia. Since the fungus is not invasive, hyphae are easily detected on cytology than histology even on Giemsa stain Charcot – Leyden crystals are better appreciated on histology than cytology. Fungal hyphae generally appear fragmented and distorted due to degenerative changes and not easily detected on H&E stain. Silver methanamine stain and Masson Fontana are helpful for identification. It can be cultured in mold inhibitory agar and sabourauds dextrose agar at 30oC. Fungal detection is better in sinus fluid DNA PCR [6] Treatment of AFS consists of combined surgical and medical treatment. Debridement of impacted mucus and aeration of diseased sinuses with systemic and topical steroids. Follow up is essential as multiple recurrences are common [7]. All 122 Journal of Clinical and Diagnostic Research. 2014 Mar, Vol-8(3): 121-122 our patients were treated with combined medical and surgical treatment with steroids being the mainstay of medical treatment. The patients were given systemic corticosteroids post-operatively in tapering doses and then shifted to intranasal steroid spray for prolonged periods. Patients have to be followed upto five years after steroid therapy because recurrence can occur even after three years [8]. All the patients are on regular follow up for the past one year and have shown no signs of recurrence.
Most of the studies in literature are based on histological findings, in our cases we tried to diagnose AFS on nasal discharge cytology. [1,9-11]. The CT scan diagnosis in one of our case was malignancy, nasal discharge cytology in this case helped the clinicians to plan their management. Thus nasal discharge cytology in cases of high degree of clinical suspicion and in proper clinical settings helped us as a first diagnostic modality.
Conclusion
Nasal discharge cytology plays an important role in diagnosis of allergic fungal sinusitis in correct clinical settings and can be used for pre-operative as well as intraoperative diagnosis of allergic fungal sinusitis and can be used as an additional diagnostic tool.
[1]. Glass Daniel, Amedee Ronald G, Allergic fungal rhinosinusitis : A review.Ochsner J. 2011 11(3):271-75. [Google Scholar]
[2]. C Torres, JY Ro, AK el-Naggar, SJ Sim, RS Weber, AG Ayala, Allergic fungal sinusitis: a clinicopathologic study of 16 cases.Hum Pathol. 1996 27(8):793-9. [Google Scholar]
[3]. S Rane, A Jayaraman, VV Holla, Allergic fungal rhinosinusitis-a case report.Indian J Pathol Microbiol. 2003 46(3):450-1. [Google Scholar]
[4]. VJ Schnadig, CH Rassekh, WK Gourley, Allergic fungal sinusitis. A report of two cases with diagnosis by intraoperative aspiration cytologyActa Cytol 1999 43(2):268-72. [Google Scholar]
[5]. SM Houser, JP Corey, Allergic fungal rhinosinusitis – Pathophysiology, epidemiology and diagnosis.Otolaryngol Clin North Am 2000 33(2):399-409. [Google Scholar]
[6]. SM El-Morsy, YW Khafagy, MM El-Naggar, AA Beih, Allergic fungal rhinosinusitis: detection of fungal DNA in sinus aspirate using polymerase chain reaction.J Laryngol Otol 2010 124(2):152-60. [Google Scholar]
[7]. Sullivan Daniel P, 111 John P Bent, Allergic fungal sinusitis: Diagnosis and management , Operative Techniques in Otolaryngology-Head and Neck Surgery Endoscopic Sinus Surgery 2001 12(1):2-6. [Google Scholar]
[8]. FA Kuhn, AR Javer, Allergic fungal rhinosinusitis : Perioperative management , prevention of recurrence, and role of steroids and antifungal agentsOtolaryngol Clin North Am. 2000 33(2):419-33. [Google Scholar]
[9]. S Challa, SG Uppin, S Hanumanthu, MK Panigrahi, AK Purohit, S Sattaluri, R Borgohain, A Chava, L Vemu, MM Jagarlapudi, Fungal rhinosinusitis: a clinicopathological study from South India.Eur Arch Otorhinolaryngol 2010 267(8):1239-45. [Google Scholar]
[10]. KT Montone, VA Livolsi, MD Feldman, J Palmer, Fungal rhinosinusitis: A Retrospective Microbiologic and Pathologic Review of 400 patients at a Single University Medical Center.Int J Otolaryngol. 2012 2012(684835) [Google Scholar]
[11]. A Das, A Bal, A Chakrabarti, N Panda, K Joshi, Spectrum of fungal rhinosinusitis; histopathologist’s perspective.Histopathology. 2009 54(7):854-9. [Google Scholar]