Benign Hepatic Mesenchymal Hamartoma (HMH) – A Case Report
Shaileshkumar Radheshyam Patel1, Vatsala Misra2, Kachnar Verma3, Pooja Gupta4, Vishal Dhingra5
1Junior Resident, Department of Pathology, Motilal Nehru Medical College, Allahabad, Uttar Pradesh, India.
2Head and Professor, Department of Pathology, Motilal Nehru Medical College, Allahabad, Uttar Pradesh, India.
3Assistant Professor, Department of Pathology, Motilal Nehru Medical College, Allahabad, Uttar Pradesh, India.
4Junior Resident, Department of Pathology, Motilal Nehru Medical College, Allahabad, Uttar Pradesh, India.
5Lecturer, Department of Pathology, Motilal Nehru Medical College, Allahabad, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Shaileshkumar Radheshyam Patel, /309, Shirdi Nagar, Navghar Fatak Road, Bhayandar (East), Thane, Maharashtra-401105 India. hone:9869620666, Email:shailesh3366@yahoo.co.in
A one-year-old male child presented with progressive enlargement of abdomen and loss of appetite which he had suffered from, since 4 months. Physical examination showed a palpable mass in right hypochondrium. Ultrasonography and MRI showed a solid mass arising from right lobe of liver. The resected mass was well encapsulated, yellowish white in colour and it measured 20 x 18 x 17cm. Cut surface showed a Nutmeg like appearance. Histology showed a well-defined, fibrous capsule with numerous ducts which were lined by flat to low cuboidal epithelium and which were surrounded by concentric layers of fibrous tissue which showed myxoid changes at places. Intervening area showed normal appearing hepatocytes with clear cell changes, dilated congested sinusoids, along with extramedullary haematopoiesis. Based on distinctive morphological features, a histological diagnosis of Benign Hepatic Mesenchymal Hamartoma of liver was made. IHC was not done, as no specific marker has been described for making a differential diagnosis. Benign Hepatic Mesenchymal Hamrtoma (HMH) of liver is an extremely rare tumour of childhood and therefore, the case was considered worth documentation.
Bile duct, Extramedullary hematopoiesis, Liver, Mesenchymal hamartoma, Paediatric tumour
Case Report
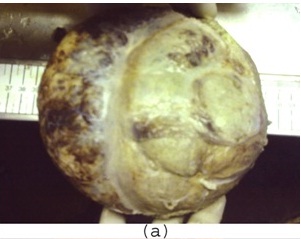
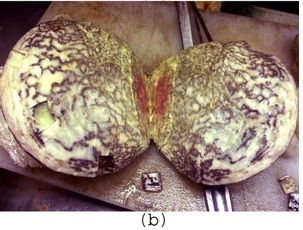
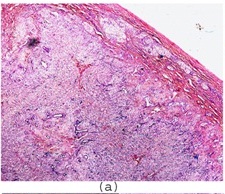
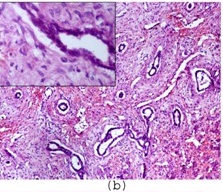
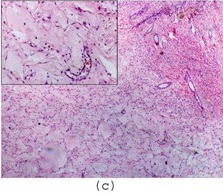
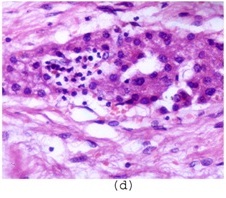
A one-year-old male child presented with progressive enlargement of abdomen and loss of appetite, which he had suffered from, since 4 months. On physical examination, a palpable mass was seen in right hypochondrium. Ultrasonography and MRI revealed a well- defined, solid mass arising from right lobe of liver, which measured 20cm in diameter. Haematological and biochemical investigations and coagulation profile were within normal limits. Patient was operated for the mass by making a mid line incision. Per-operatively, a well encapsulated, solid mass arising from right lobe of liver was seen and it was resected by enucleation method, thus saving the rest of the liver. On gross examination, tumour mass was found to be well encapsulated, yellowish white in colour and it measured 20 x 18 x 17cm [Table/Fig-1a]. No attached liver tissue was seen. Cut surface showed multiple brownish bands like areas in a dirty white background (Nutmeg appearance) [Table/Fig-1b]. Multiple pieces from representative areas were processed. Histology from different areas showed a mass which was covered by a well-defined, fibrous capsule[Table/Fig-2a]. Underlying areas showed numerous cystically dilated ductular structures which were lined by flat to low cuboidal epithelium [Table/Fig-2b], which were surrounded by concentric layers of fibrous tissue, which showed myxoid changes at places [Table/Fig-2c]. Intervening area showed normal appearing hepatocytes with clear cell changes, dilated congested sinusoids, along with extramedullary haematopoiesis [Table/Fig-2d].
Based on distinctive morphological features, a histological diagnosis of Benign Hepatic Mesenchymal Hamartoma of liver was made. IHC was not done, as no specific marker has been described for making a differential diagnosis. The patient recovered well and was discharged from the hospital. He did not report back for follow-up.
Discussion
HMH is a tumour which occurs in childhood, with mean age of presentation of 20 months [1]. This lesion probably represents a localized abnormality of ductal plate development and is related to polycystic disease, congenital hepatic fibrosis, Caroli’s disease and biliary hamartoma. The pathogenesis which has been suggested is that, at birth, the basic lesion of congenital hepatic fibrosis corresponds to ductal plate formation of interlobular bile ducts which result from faulty development, i.e. disturbance in epithelio-mesenchymal inductive interaction. (Desmet1). Patient usually presents with progressive enlargement of abdomen or mass effect of tumour. Radiological features reveal solid or cystic masses of variable sizes which reach sizes of up to 30cm [2]. Multiple cysts are usual findings. Cysts contain clear to yellow fluid. Occasionally, gelatinous material may be present. A thin rim of normal liver parenchyma is often seen at the periphery. On FNAC, clusters of normal bile duct epithelium and hepatocytes which are admixed with bland mesenchymal cells in a myxoid background are highly suggestive of HMH. Histologically, myxomatous connective tissue containing scattered bland stellate-shaped mesenchymal cells are seen. Branching bile ducts are seen and they are surrounded by loose mesenchyme. The cysts often have no epithelial lining and are bounded by the mesenchyme. Extramedullary haematopoiesis is noted in approximately 85% of cases[3]. Hepatocytes may be present in single cords or in large groups, especially at the periphery of the mass. Atypical mitoses and invasion of adjacent liver are absent. Although it is rare, a malignant transformation to embryonal sarcoma (malignant mesenchymoma) has been reported. Begueret et al., reported a case of a large, cystic hepatic mass in a 17-year-old girl, that had areas which were characteristic of both embryonal sarcoma and HMH and a transition zone that contained the architectural features of a HMH and embryonal sarcoma [4]. Breakpoint at 19q13.4 has been reported in several cases [5]. Due to its age and presentation as intra-abdominal mass, differential diagnoses which were considered were hepatoblastoma, infantile haemangioendothelioma and undifferentiated ( embryonal) sarcoma.
There is no specific immunohistochemistry (IHC) marker for HMH and IHC is used primarily to rule out other entities. In HMH, bile ducts and hepatocytes are cytokeratin positive, whereas the mesenchyme and pseudocysts are vimentin positive [3]. In, myxomatous infantile haemangioendotheliomas endothelium is positive for factor VIIIrelated antigen, CD31, and CD34 immunohistochemical stains.
Mixed epithelial-mesenchymal hepatoblastoma is very similar to HMH histologically. This particular type of hepatoblastoma can be composed of relatively bland appearing hepatocytes (of the foetal type) with spindle/stellate mesenchyme, osteoid or cartilage. IHC is not helpful in its differentiation.
Distinguishing embryonal sarcoma from HMH is based on identifying atypical, pleomorphic stellate cells in a background of haemorrhage and/or necrosis. Periodic acid-Schiff–positive and diastase resistant hyaline globules may be seen in tumour cells or in stroma. An epithelial component is not seen in embryonal sarcoma, while it is present in HMH. Complete tumour excision is curative, with rare recurrences.
Thus, this rare case has been documented here to highlight its histological features and to make the pathologists and clinicians aware of these benign intra-abdominal cystic lesions in differential diagnoses of other malignant intra-abdominal lesions which are seen in infants and children.
Gross Appearance: Outer surface with whitish and brownish area
Cut surface of mass showing nutmeg appearance
Section showing well-defined fibrous capsule along with bile ductules and hepatocytes (H&E x40)
Cystically dilated bile ducts surrounded by concentric layers of mesenchymal tissue (H&E x100) Inset -Higher magnification showing low cuboidal lining of bile duct (H&E x 400)
Myxoid changes in stroma with normal hepatocyte and bile ductules (H&Ex100). Inset- stromal myxoid changes (H&E x400)
Bile sinusoids showing extramedullary hematopoiesis in liver (H&E x100)
[1]. A Pandey, AN Gangopadhyay, SP Sharma, V Kumar, DK Gupta, SC Gopal, Patne SC. Long-term follow up of mesenchymal hamartoma of liver- Single center studySaudi J Gastroenterol 2011 17:20-2. [Google Scholar]
[2]. B Yen J, S Kong M, N Lin J, Hepatic mesenchymal hamartomaJ Paediatr Child Health. 2003 39:632-4. [Google Scholar]
[3]. KG Ishak, ZD Goodman, JT Stocker, Tumors of the Liver and Intrahepatic Bile Ducts. Washington, DC: Armed Forces Institute of Pathology;Atlas of Tumor Pathology 2001 :71-79.3rd series, fascicle 31. [Google Scholar]
[4]. H Begueret, H Trouette, P Vielh, C Laurent, G MacGrogan, M Delsol, Hepatic undifferentiated embryonal sarcoma: malignant evolution of mesenchymal hamartoma? Study of one case with immunohistochemical and flow cytometric emphasis.J Hepatol 2001 34:178-9. [Google Scholar]
[5]. MA Siddiqui, BJ McKenna, Hepatic Mesenchymal Hamartoma A Short ReviewPathol Lab Med 2006 130:1567-9. [Google Scholar]