Microfilaria in Human Subcutaneous Dirofilariasis: A Case Report
Ajit Shriram Damle1, Jyoti Anil Iravane (Bajaj)2, Mukta Nagorao Khaparkhuntikar3, Ganesh Tarachand Maher4, Rajashri Vilasrao Patil5
1 Professor and Head, Department of Microbiology, Government Medical College, Aurangabad, Maharashtra, India.
2 Associate Professor, Department of Microbiology, Government Medical College, Aurangabad, Maharashtra, India.
3 Assistant Professor, Department of Microbiology, Government Medical College, Aurangabad, Maharashtra, India.
4 Resident, Department of Microbiology, Government Medical College, Aurangabad, Maharashtra, India.
5 Resident, Department of Microbiology, Government Medical College, Aurangabad, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ganesh T. Maher, 27, Nathpuram, Near Nath-valley school, Paithan Road, Aurangabad-431001, Maharashtra, India.
Phone: 8087482741,
E-mail: ganeshmaher@yahoo.co.in
Human subcutaneous dirofilariasis, a rare zoonosis is being increasingly reported from various parts of the world. Most of the reported cases have lesions in and around the eye. The adult female dirofilariae release microfilaria into the definitive host’s blood. Various mosquitoes that serve as intermediate hosts such as Culex, Aedes and Anopheles take up the microfilariae (mf-L1) while feeding on an infected host. Microfilariae develop in the mosquitoes. The transmission to dogs or other hosts including humans occurs through mosquito bite during subsequent blood meal. Humans may be infected as aberrant (accidental) hosts, mainly by D. repens and D. immitis. D. repens usually resides subcutaneously, while D. immitis frequently ends up in the human lung. In human infections usually just one larva develops, which does not reach sexual maturity. In India, almost all reported cases of dirofilariasis in humans have involvement of face in the form of ocular dirofilariasis with a few reports on subcutaneous dirofilariasis. We report a case of human subcutaneous dirofilariasis, from western India, involving leg and showing microfilaria in tissue indicating presence of gravid female dirofilaria (sexual maturity). To the best of our knowledge, it is among rare cases of subcutaneous dirofilariasis wherein microfilariae have developed in human host.
Microfilaria, Dirofilariasis, Human, Subcutaneous
Case Report
A 62-year-old male farmer, resident of Maharashtra presented in October 2012 with pain, redness and burning sensation just above left ankle for a period of 3 months. A pea-nut sized nodular swelling occurred over the same region within the past 20 days, which gradually migrated to the dorsum of left foot. On examination, the swelling was soft and tender. Systemic examination did not reveal any abnormal findings. The hemogram was normal. The lesion at that time was treated with antihistaminics considering the lesion to be allergic. It did not respond.
Then, considering the lesion to be probably of infective type, an incision was taken under local anesthesia by a private practitioner. A slender, live parasite measuring 6 cm in length wriggled out from the biopsy material removed from the nodular swelling. Being seen on dorsum of foot, it was suspected to be guinea worm. The worm was sent for histology. While observing the histopathology slides, apart from cross-sections of the worm, a microfilaria was observed [Table/Fig-1]. This indicated it to be filarial worm and not guinea worm. A cross-section of the worm showed an average diameter to be 460 μm with 20 μm thick cuticle having ridges on the external surface. A well developed muscular layer was also noted beneath the cuticle. In the body cavity, two uteri were clearly seen filled with mirofilariae in various stages of development. Presence of ridges on cuticle ruled out W. bancrofti and B. malayi. Thus we narrowed down to Dirofilaria Sp. The ridges of D. repens are spaced at double the size of height of individual ridge [1]. This feature along with the diameter of the worm as seen in sections, thickness of the cuticle, well developed muscular layer clinched the diagnosis as D. repens [Table/Fig-2].
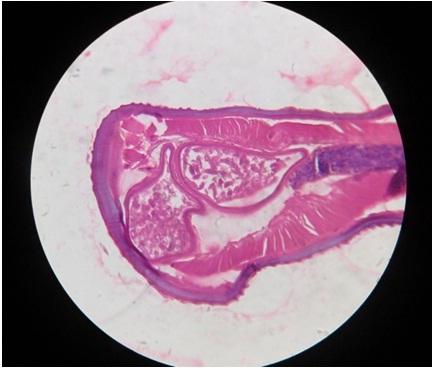
Cross-section of adult dirofilaria worm

Our patient had undergone surgical resection of nodule. As surgical resection of lesion is both diagnostic as well as therapeutic for human subcutaneous dirofilariasis, no further treatment was required. There was no recurrence of the disease afterwards.
Discussion
Dirofilariasis is primarily confined to animals such as dogs, cats, foxes, raccoons and some wild animals that act as definitive hosts. Various mosquitoes serve as intermediate hosts take up the microfilariae (mf-L1) while feeding on an infected host. Microfilariae develop further in mosquitoes. The transmission to dogs or other hosts including humans occurs through mosquito bite during subsequent blood meal. In human infections usually just one larva develops, which does not reach sexual maturity [2–4].
In India, almost all reported cases of dirofilariasis in humans have involvement of face in the form of ocular dirofilariasis with a few reports on subcutaneous dirofilariasis [3–11]. Although about 40 different species of dirofilaria are recognized, fewer than 6 are known to cause human infections, which can be found worldwide [8]. D. repens causes most cases of human dirofilariasis in Europe, Asia and Africa; hence it is considered an emerging zoonosis in these continents [9]. The first reported case of human ocular dirofilariasis in India occurred in Kerala in June 1976 [3] and the first reported case of human subcutaneous dirofilariasis caused by D. repens occurred in June 2004 from the same region [5]. While it is considered endemic in southern India, there are few case reports from the Northern and Western parts of India [8]. Among the documented cases of human dirofilariasis caused by D. repens, recorded in India, most of them had ocular infections and a few had subcutaneous involvement of the face [10–12]. A case of subcutaneous dirofilariasis involving scrotal region has also been reported from (Orissa) eastern India [12].
In our case, as the worm was detected from a lesion on foot, primary clinical suspicion was guinea worm (Dracunculus medinensis) infection. The size of the worm was very small as compared with that of guinea worm. Guinea worm has been eradicated from India [13, 14]. Moreover observing an intact microfilaria in the histopathology section, ruled it out to be guinea worm.
D. repens is the most common causative agent while in a few cases D. immitis is also recorded as a causative agent of dirofilariasis from India. Exact identification of species may be possible only after studying the fully matured worm. Sexes are determined by the number of reproductive tubes present in the body cavity, typically two in females and only one in males [1].
The definite diagnosis of HSD can be made after surgical excision or biopsy. Blood eosinophilia or elevated serum IgE levels are rarely observed [8]. In order to confirm the diagnosis of D. repens infection, DNA extraction followed by pan filarial polymerase chain reaction (PCR) may be performed [5]. Surgical resection/ Excision of lesion is both diagnostic as well as therapeutic. There is no need of chemotherapy. In our case, the patient responded to treatment and there was no recurrence of the disease.
Subcutaneous dirofilariasis is mostly caused by D. repens in Asia and patients usually present with single migratory nodules measuring 0.5 to 2.5 cm in size, occurring in exposed parts of the skin, which may or may not be tender [8].
In human infection of D.repens, parasite development is impaired (i.e. dead end infection) and microfilariae have never been reported in human blood [8,10]. In fact even maturation of the worm in human host is rare [4]. Thus finding of mirofilaria in human subcutaneous tissue in our case is interesting and remarkable.
Human infection with D. repens has been increasing in India and other parts of the world [3]. Many of them remain undiagnosed or unreported. Hence, it is emphasized that physicians should have an increased awareness about this infection and includes dirofilariasis in the differential diagnosis in patients presenting with subcutaneous nodules (migratory or non-migratory, tender or non-tender) at any site of body. They should develop a high index of suspicion in order to recognize this infection.
Declaration
The present study has been presented as a case report in MAHAMICROCON 2013 XIX Maharashtra Chapter Conference of Indian Association of Medical Microbiologists held at Armed Forces Medical College, Pune from 4th- 6th October, 2013.
[1]. Orihel TC, Eberhard ML, Zoonotic filariasisClin Microbiol Rev 1998 11:366-81.from Marusic ’08 [Google Scholar]
[2]. Garcia LS, Diagnostic Medical Parasitology 2003 4th edWashington, D.CASM Press:354-6. [Google Scholar]
[3]. Joseph K, Vinayakumar AR, Criton S, Vishnu MS, Pariyaram SE, Periorbital mass with cellulitis caused by dirofilariaIndian J Med Microbiol 2011 29:431-3. [Google Scholar]
[4]. Popescu I, Tudose I, Paul R, Muntau B, Giurcaneanu C, Poppert S, Human Dirofilaria repens Infection in Romania: A Case ReportCase Reports in Infectious Diseases Vol 2012 Article ID 472976 [Google Scholar]
[5]. Popescu I, Tudose I, Paul R, Muntau B, Giurcaneanu C, Poppert S, Human Dirofilaria repens Infection in Romania: A Case ReportCase Reports in Infectious Diseases Vol 2012 Article ID 472976 [Google Scholar]
[6]. Nadgir S, Tallur SS, Mangoli V, Halesh LH, Krishna BV, Subconjunctival dirofilariasis in IndiaSoutheast Asian J Trop Med Public Health 2001 32:244-6. [Google Scholar]
[7]. Bhat KG, Wilson G, Mallya S, Human dirofilariasisIndian J Med Microbiol 2003 21:223 [Google Scholar]
[8]. Srinivasamurthy V, Rao MS, Thejaswini MUY, Human subcutaneous dirofilariasisAnn Trop Med Public Health 2012 5:349-51. [Google Scholar]
[9]. Permi HS, Veena S, Kishan Prasad HL, Kumar YS, Mohan R, Shetty KJ, Subcutaneous human dirofilariasis due to Dirofilaria repens: Report of two casesJ Glob Infect Dis 2011 3:199-201. [Google Scholar]
[10]. Khurana S, Singh G, Bhatti HS, Malla N, Human subcutaneous dirofilariasis in India: A report of three cases with brief review of literatureIndian J Med Microbiol 2010 28:394-6. [Google Scholar]
[11]. Nath R, Bhuyan S, Dutta H, Saikia L, Human subcutaneous dirofilariasis in AssamTrop Parasitol 2013 3:75-8. [Google Scholar]
[12]. Singh R, Shwetha JV, Samantaray JC, Bando G, Dirofilariasis: A rare case reportIndian J Med Microbiol 2010 28:75-7. [Google Scholar]
[13]. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1117704/ [Google Scholar]
[14]. Dam T, Das P, The Importance of Dirofilariasis in IndiaThe Internet Journal of Parasitic Diseases 2006 1(1)DOI: 10.5580/11b6 [Google Scholar]