Piriformis Fossa – An Anatomical and Orthopedics Consideration
O.P. Lakhwani1, P.S. Mittal2, D.C. Naik3
1 Associate Professor, Department of Orthopedics, ESI – Postgraduate Institute of Medical Sciences and Research, New Delhi, India.
2 Assistant Professor, Department of Anatomy, Sri Aurobindo Medical College and Postgraduate Institute, Indore (M.P.), India.
3 Professor and Head, Department of Anatomy, S. S. Medical College, Rewa (M.P.), India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. O.P. Lakhwani, Associate Professor, Department of Orthopedics, ESI – Postgraduate institute of Medical Sciences and Research, Basaidarapur, Ring Road, New Delhi – 110015, India.
Phone: 09827395622,
E-mail: orth365@gmail.com
Introduction: Piriformis fossa is an important anatomical landmark having significant clinical value in orthopedic surgery; but its location and anatomical relationship with surrounding structures are not clearly defined. Hence it is necessary to clearly describe it in respect to anatomical and orthopedic aspect.
Materials and Methods: Fifty Cadaveric dry femoral bones and Dissection of the four hip specimens were used to study the Piriformis fossa in respect to location and its relationship with surrounding structures. Clinical importance of piriformis fossa was determined in reference to antegrade femoral nail insertion.
Observations: Piriformis muscle and so called piriformis fossa are unrelated entities. Piriformis fossa is anatomical site of insertion of obturator externus. In dry cadaveric femora; fossa was not always located in the direction of femoral shaft. It was located in the direction of femoral shaft in 24% cases only. In 68% cases femoral canal was aligned lateral and in 8% cases, it lies medial to the fossa.
Conclusion: Piriformis fossa should be named as Trorchanteric fossa or Obturator fossa for better anatomical description. So called Piriformis fossa does not found to be universally corresponding to femoral shaft hence selection of entry site should be based on variable proximal femur and area on femur which corresponds to femoral shaft.
Piriformis fossa, Trochanteric fossa, Piriformis muscle, Femoral nail
Introduction
Piriformis fossa [1–5] is an important anatomical landmark described as the entry point for antegrade intramedullary nailing of fracture shaft femur. In orthopedics literature the piriformis fossa [1–4] is considered as synonymous to the insertion of the piriformis muscle. Human Anatomy literature does not mention any structure on proximal femur as piriformis fossa rather it mentions landmark named as Trochanteric fossa [5,6]. So, it is necessary to describe and revisit the Piriformis fossa or the Trochanteric fossa and its anatomical basis for the better understanding. The present study is aimed to rectify these doubts and establish the correct anatomical landmarks and its significance.
Materials and Methods
Study involved the fifty dry adult cadaveric femora non-fractured without any deformity in anatomy museum and biomechanical laboratory. Selected femora 24 were of Right side and 26 Left side. Dissection of four lower extremities of formalin fixed adult Indian cadavers with mobile hip joints that allowed 60 degrees of hip flexion and without any scars indicating former hip surgery was undertaken to localize and describe the anatomical relationship of piriformis fossa with the surrounding structures.
Observations
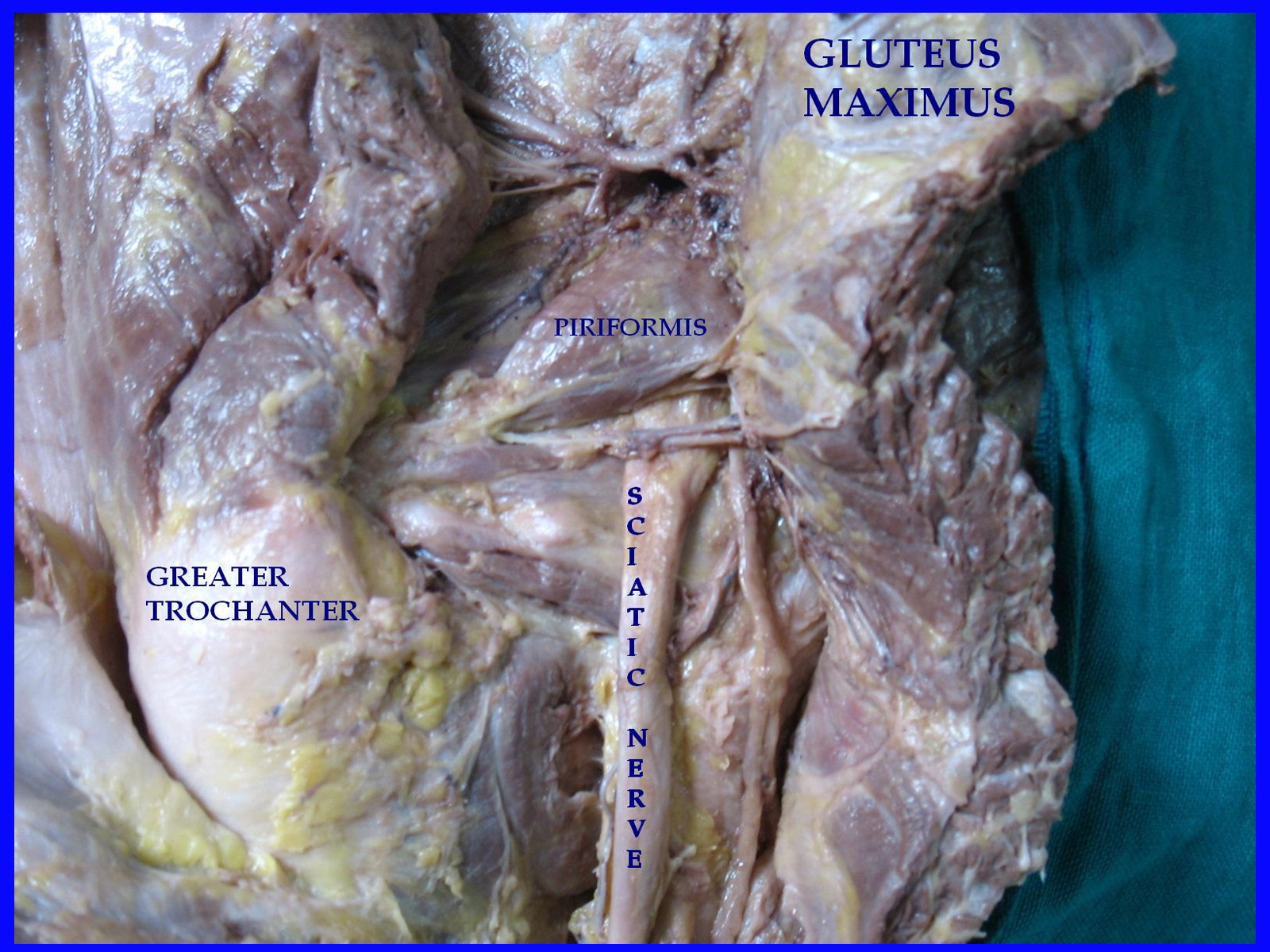
The dissection of the specimens of human cadaveric hip showed piriformis muscle as a key structure in deep gluteal region. The muscle arises from the front of middle three sacral vertebrae. Its rounded tendon inserted into the medial part of the tip of the greater trochanter of femur. It divides Greater sciatic foramen into superior and an inferior part; the nerve and the vessels that emerge superior to the piriformis muscle are the superior gluteal nerve and vessels and inferiorly named as inferior gluteal nerve and vessels. Sciatic nerve also emerges inferiorly to this muscle [Table/Fig-1,2].
Showing location and relationship of muscles in posterior dissection of cadaveric hip specimen
Showing locations of piriformis and obturator externus muscles
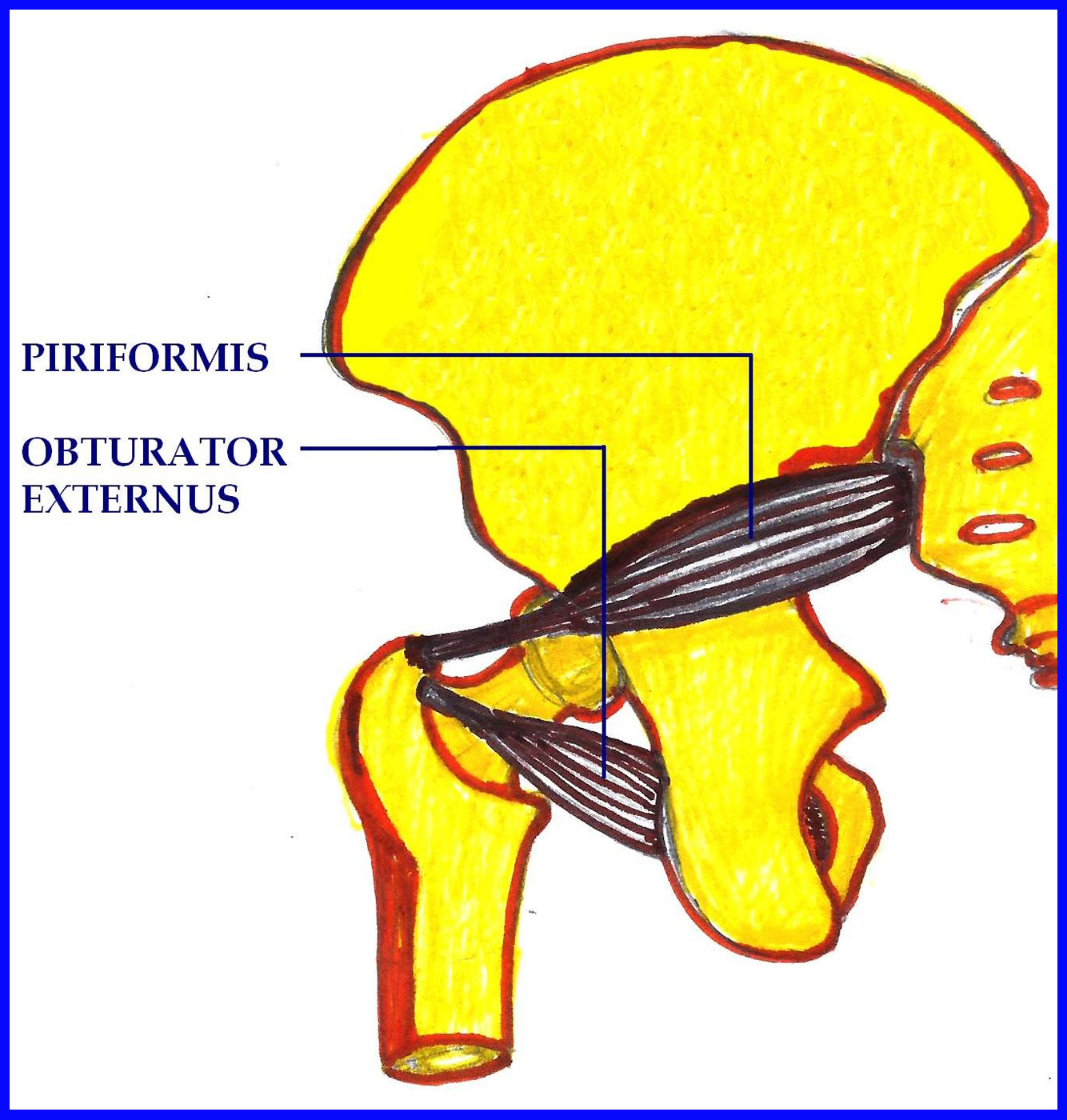
Obturator externus muscle is a flat, triangular muscle originates from the anteromedial two-thirds of the external surface of the obturator membrane and from the adjacent part of the pubis and ischial rami and was inserted on the floor of a fossa located on medial surface of greater trochanter.
Cadaveric dry femoral bone showed the greater trochanter which is large and quadrangular projection at the junction of the neck and shaft. Rough area at tip of greater trochanter gives the insertion to piriformis tendon. Its medial surface has deep depression which gives the insertion to obturator externus muscle. This fossa was also identified during dissection of cadevaric hip. For anatomical and safe entry site of femur antegrade nailing direction of femoral shaft and location of this fossa was determined. In 12 (24%) dry cadaveric femora, fossa lies in the direction of shaft. In 34 (68%) alignment of the femoral shaft was lateral to the fossa in the region of tip of greater trochanter. In 4 (8%) femoral shaft was aligned medial to fossa in the direction of femoral neck [Table/Fig-3,4]. Piriformis muscle was consistently attached to tip of greater trochanter and fossa provides the insertion site to the obturator externus.
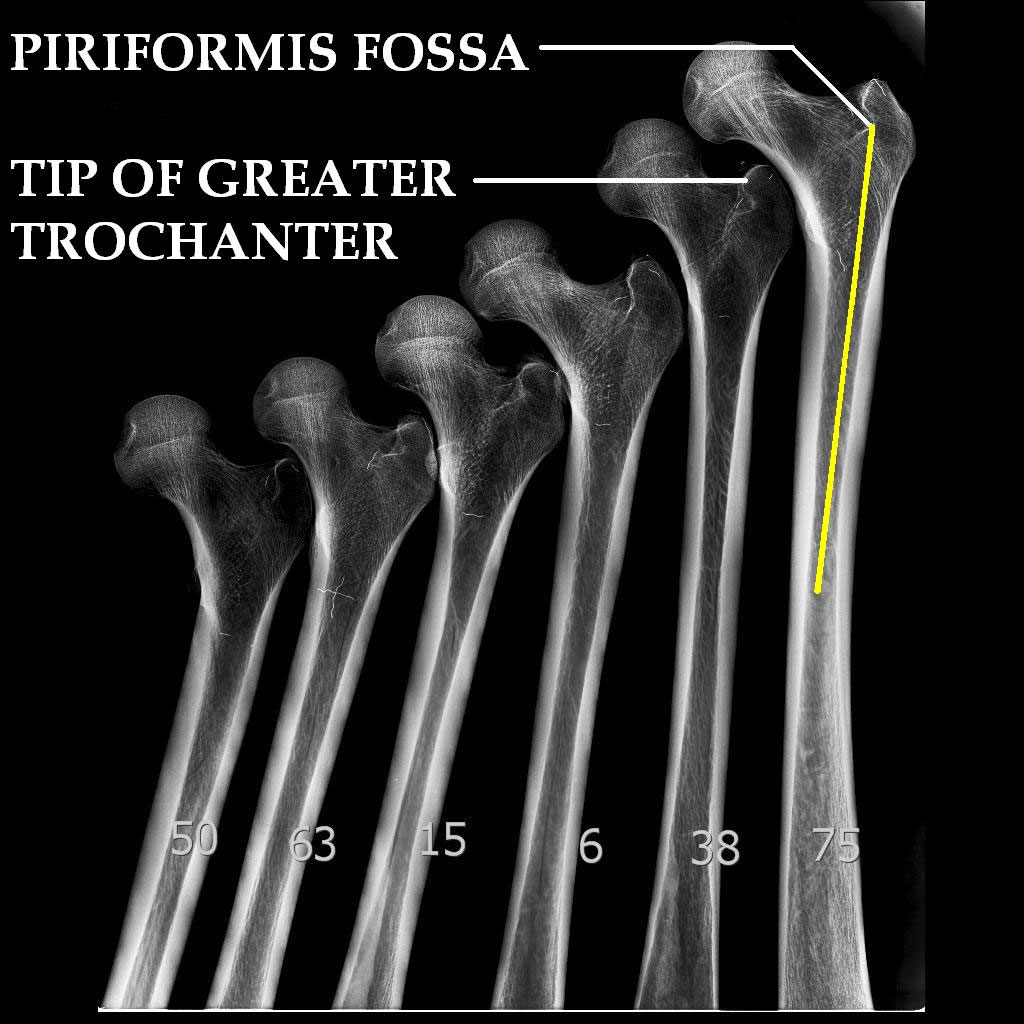
Showing location of the trochanteric fossa (site of insertion of the obturator externus) and tip of greater trochanter (site of insertion of the piriformis)

Skiagram of the femora verifying radiological location of the trochentric fossa (Piriformis fossa) and greater trochanter tip
Discussion
The piriformis [5,6] (L. piriformis = “pear shaped”) is a muscle in the gluteal region of the lower limb. It was first named by Spigelius, a professor from the University of Padua in the 16th century. However, anatomical dissection of this region and the study of the proximal end of the dry femoral bones suggested that so called “Piriformis fossa” is neither piriform in shape nor piriformis muscle is being inserted in to it.
The insertion of piriformis muscle represents a small, area on the tip of the greater trochanter whereas the trochanteric fossa is a deep depression on the inner surface of the greater trochanter. This fossa is not the insertion site for piriformis muscle rather obturator externus muscle was found to be inserted in the fossa. The obturator externus is actually located anterior to the remaining all lateral rotators just behind the neck of femur and can’t be seen easily from posterior aspect of hip during surgical exposure while, piriformis can be easily identified in surgical exposure, hence probably it has been taken as synonymous with the fossa. Piriformis muscle and “Piriformis fossa” are two unrelated entities. Fact was also been studied by Papadakis SA et al., [7] and considered as drawing mismatch or terminology error. Current study further analyses and describes anatomical location and description of both the terms.
Piriformis fossa can be felt during surgical exposure and can be seen in the skiagram. In orthopedic literature [8,9], it has been described as standard entry site for femoral nail insertion and considered to lie in the direction of femoral canal. In an study by Ricci WM et al., [10], trochanteric versus piriformis fossa entry portal for treatment of femoral shaft fracture and anatomical study by Wolfgang Grechenig et al., [11] it was found that piriformis fossa is not the anatomical site for femoral nail insertion. Clinical [12–13] and anatomical studies [14] described the various entry points for femoral nail insertion. In the present study we found that the femoral shaft did not always correspond to the piriformis fossa. In only 24% dry cadaveric femora, this fossa lies in the direction of shaft, in 68% femora alignment of the shaft was lateral to the fossa in the region of tip of greater trochanter and in 8% femora, the femoral shaft was aligned medial to fossa in the direction of femoral neck.
Conclusion
So called Piriformis fossa should be termed as Trochateric or Obturator fossa for clear and correct anatomical description. Proper entry site for femoral nailing is variable and cannot be fixed universally, due to variable alignment of femoral canal, trochateric fossa cannot be used as universal entry site; rather it should be determined by proximal femoral anatomy and direction of shaft of femur to the proximal corresponding area on femur.
[1]. Kempf I, Grosse A, Beck G, Closed locked intramedullary nailing. Its application to comminuted fractures of the femurJ Bone Joint Surg Am 1985 67:709-20. [Google Scholar]
[2]. Winquist RA, Hansen ST, Clawson DK, Closed intramedullary nailing of femoral fracturesJ Bone Joint Surg Am 1984 Apr 66(4):529-39. [Google Scholar]
[3]. Lakhwani OP, Correlation of Trochanter-Shaft Angle in Selection of Entry Site in antegrade Intramedullary Femoral NailISRN Orthopedics 2012 Article ID 431374,doi:10.5402/2012/431374 [Google Scholar]
[4]. Solomon LB, Lee YC, Callary SA, Beck M, Howie DW, Anatomy of piriformis, obturator internus and obturator externus:implications for the posterior surgical approach to the hipJ Bone Joint Surg Br September 2010 92-B:1317-24. [Google Scholar]
[5]. Susan Standring; 40th Ed GRAY’S Anatomy-The Anatomical Basis of Clinical Practice: P-1361-72 [Google Scholar]
[6]. Moore KL, Agur AMR, Essential clinical anatomy 3rd ed 2007 BaltimoreLippincott Williams & Wilkins [Google Scholar]
[7]. Papadakis SA, Shepherd L, Babourda EC, Papadakis S, Piriform and trochanteric fossae. A drawing mismatch or a terminology error?A review Surg Radiol Anat 2005 [Google Scholar]
[8]. Nork SE, Femoral shaft fractures. In: Bucholtz RW, Court-Brown CM, Heckman JD, Tornetta PRockwood and Green’s fractures in adults 2010 7th ed.PhiladelphiaWolters Kluwer/Lippincott Williams & Wilkins:1655-1777. [Google Scholar]
[9]. Browner BD, Caputo AE, Femur fractures: antegrade intramedullary nailing. In: Wiss DA editorMaster techniques in orthopaedic surgery: fractures 2006 2nd edPhiladelphiaLippincott William & Wilkins:323-47. [Google Scholar]
[10]. Ricci WM, Schwappach J, Tucker M, Trochanteric versus piriformis entry portal for the treatment of femoral shaft fracturesJ Orthop Trauma 2006 20:663-67. [Google Scholar]
[11]. Wolfgang Grechenig, Wolfgang Pichler, Hans Clement, Norbert Peter Tesch, Stephan Grechenig, Anatomy of the greater femoral Trochanter: clinical importance for intramedullary femoral nailing Anatomic study of 100 cadaver specimensActa Orthopaedica 2006 77(6):899-901. [Google Scholar]
[12]. Ostrum Robert F, A Critical Analysis of the Eccentric Starting Point for Trochanteric Intramedullary Femoral NailingJ Orthop Trauma 2005 19:681-86. [Google Scholar]
[13]. Ansari Moein CM, ten Duis HJ, Oey PL, de Kort GA, vd Meulen W, Intramedullary nailing through the trochanteric fossa versus greater trochanter tip: prospective randomized study with in-depth functional outcome resultsEuropean Journal of Trauma 2011 37(6):615-22. [Google Scholar]
[14]. Gausepohl T, Pennig D, Koebke J, Antegrade femoral nailing: an anatomical determination of the correct entry pointInjury 2002 :701-05. [Google Scholar]