Papillary thyroid carcinoma (PTC) is the most common histological type of thyroid cancer and accounts for more than 80 % of papillary thyroid malignancies [1]. DeLellis defined papillary carcinoma as a well differentiated malignant epithelial tumor characterized by formation of papillary structures, psammoma bodies and a set of distinct nuclear features such as grooves , pseudoinclusions and ground glass appearance [2]. Many variants of papillary carcinoma have been described-oncocytic, tall cell, diffuse sclerosing, encapsulated and follicular variant which is the most common subtype [3]. Fine needle aspiration cytology (FNAC) is an important investigation in preoperative diagnosis of thyroid lesions [4]. Follicular variant of papillary thyroid carcinoma (FVPTC) is a well defined entity in histopathology, but its diagnosis in FNAC is usually missed and is challenging [5]. Preoperative diagnosis is clinically significant because FVPTC behaves similar to classic PTC and its misdiagnosis leads to conservatory surgery and a need for revision surgery after biopsy confirmation. Though many studies had been performed in this area, diagnosis of FVPTC in FNAC smears is still a challenging one. Our study analyzes the cytological features which would help to increase the sensitivity of FNAC in diagnosing this lesion with reasonable accuracy.
Materials and Methods
Twenty six cases of histologically confirmed FVPTC with the FNAC slides were obtained from the pathology laboratory of a rural tertiary care referral hospital over a period of 6 years (2007 – 2012). Out of 26 cases, 4 were excluded from the study due to inadequate material for reporting. Smears stained with Papanicolaou and hematoxylin & eosin (H&E) stains were evaluated. Papanicolaou stained slides were analyzed because it increase the sensitivity of detection of nuclear features of PTC [6]. Cytomorphological features were analyzed by two independent pathologists from a minimum two representative smears and the results were recorded. Presence of 5-6 groups of well-preserved follicular cells, with each group containing 10 or more cells on at least two slides from different passes satisfies the adequacy of the aspirate [7].
The features analyzed included cellularity, microscopic pattern (monolayered sheets, syncytial clusters, microfollicular pattern, papillary fronds and single cell distribution), nuclear features (anisonucleosis, nucleomegaly, fine powdery chromatin, grooves, intranuclear cytoplasmic inclusions, irregular nuclear membrane and nucleoli), colloid characteristics (thick or thin ) and psammoma bodies. These features were graded as absent (0), occasional (1), frequently seen (2), prominent finding (3). Statistical analysis was done based on bivariate Pearson’s correlation coefficient.
Results
Among total cases, 21 were females and one was a male with age range 21 – 50 years. All patients had a solitary nodule of size 1 – 4.5 cm except for one patient with multicentric presentation. In the preoperative FNAC diagnosis, 14 cases were diagnosed with papillary carcinoma including classic PTC; 7, FVPTC; 3, PTC suspicious; 4. Diagnosis of remaining 8 cases revealed, follicular neoplasm; 5 and adenomatous goiter; 3. Diagnosis upon review were, FVPTC; 11, classic PTC; 7, PTC suspicious; 2, follicular neoplasm; 1 and adenomatous goiter; 1 [Table/Fig-1].
Preoperative diagnosis by FNAC and after review PTC – papillary thyroid carcinoma, FVPTC- follicular variant of papillary thyroid carcinoma
| Diagnostic category | Number of cases |
|---|
| Preoperative diagnosis | After review |
|---|
| Classic PTC | 7 | 7 |
| FVPTC | 3 | 11 |
| Suspicious of PTC | 4 | 2 |
| Follicular neoplasm | 5 | 1 |
| Adenomatous goiter | 3 | 1 |
| Total | 22 | 22 |
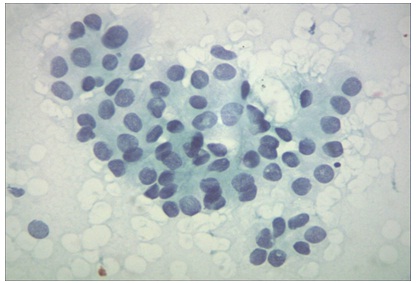
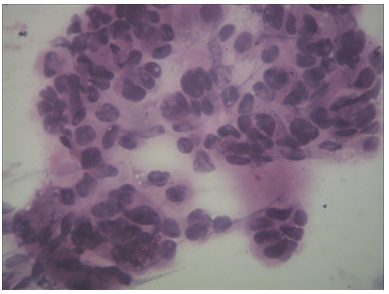
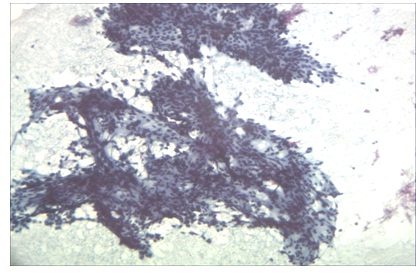
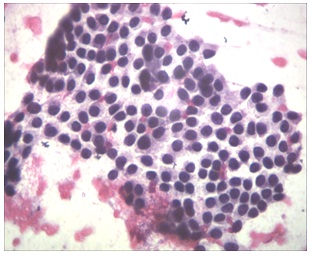
Our observation of nuclear features were shown in [Table/Fig-2]. Cases with moderate to high cellularity; 18 while low cellularity; 4 cases. Although multiple microscopic patterns in some cases were observed [Table/Fig-3,4,5and6], predominant microscopic pattern was microfollicular (20 cases), followed by syncytial clusters (17 cases). Grooves and pseudo inclusions were seen in 20 and 12 cases respectively [Table/Fig-7]. Fine powdery chromatin, anisonucleosis and nucleomegaly were seen in all cases [Table/Fig-8]. Number of cases with thick chewing gum colloid [Table/Fig-9]; 16, hurthle cells; 5, and psammoma bodies not identified in any of these cases.
Microscopic pattern and nuclear features
| Microscopic pattern |
|---|
| Grading | 0 – absent | 1- occasional | 2 – frequent | 3 – prominent |
|---|
| Microfollicular pattern | 2 | 2 | 12 | 6 |
| Syncytial clusters | 5 | 4 | 10 | 3 |
| Monolayered sheets | 10 | 2 | 6 | 4 |
| Papillary fronds | 15 | 3 | 3 | 1 |
| Single cells | 14 | 3 | 4 | 1 |
| Nuclear features |
| Nuclear grooves | 2 | 6 | 9 | 5 |
| Pseudoinclusion | 12 | 3 | 5 | 2 |
| Fine powdery chromatin | 0 | 3 | 8 | 11 |
| Anisonucleosis | 0 | 1 | 3 | 18 |
| Nucleomegaly (2 times RBC) | 0 | 1 | 2 | 19 |
| Irregular nuclear membrane | 10 | 6 | 4 | 2 |
| Nucleoli | 9 | 8 | 4 | 1 |
Cells in microfollicular pattern.( Papanicolaou stain, x400)
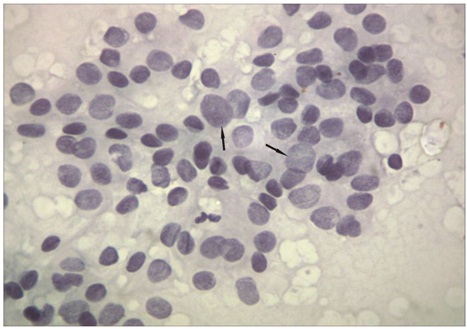
Cells in syncytial clusters. (H&E stain, x400)
Cells in papillary fronds. (Papanicolaou stain, x40)
Cells in monolayered sheets. (H&E stain, x100)
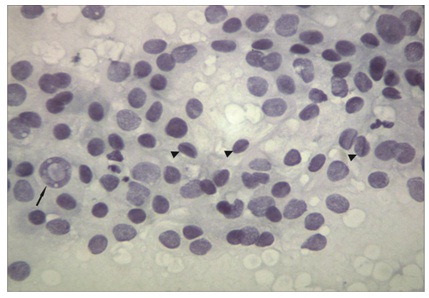
show intranuclear pseudoinclusion (arrow) and nuclear grooves (arrow heads). (Papanicolaou stain, x400)
show anisonucleosis, nucleomegaly (arrow) and fine powdery chromatin ( Papanicolaou stain, x400)
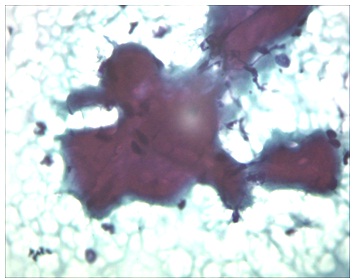
Thick chewing gum colloid (Papanicolaou stain, x400)
The p-value for microfollicular pattern, monolayered sheets, papillary fronds, nuclear grooves, nuclear pseudoinclusions and nucleoli were found to be significant.
Discussion
FVPTC was first described by Crile and Hazard who named this lesion alveolar variant of PTC [8]. This was confirmed by Lindsay and the author observed that although the neoplasm had a follicular architecture, the nuclear features were that of conventional PTC. Therefore the tumor should be designated FVPTC. Chen and Rosai stressed the importance of nuclear rather than architectural pattern in making a diagnosis of PTC and showed that FVPTC behaved similarly to the conventional PTC [9].
Because of the follicular pattern it was often confused with other benign and neoplastic follicular lesions including adenomatoid nodule , follicular adenoma and follicular carcinoma [10,11]. The diagnosis was solely based on nuclear features and owing to paucity of these findings on aspiration material, some of these lesions could be easily missed [7]. Even focal nuclear features of papillary carcinoma thyroid in fine needle aspiration cytology are strongly associated with papillary carcinoma at resection,[12]particularly FVPTC [13]. Higher tumor size and rate of suspicious for malignancy cytology were significantly higher in FVPTC [14]. If we use histologic diagnosis as the gold standard, the sensitivity and specificity of FNAC diagnosis of FVPTC were 42% and 83%, respectively [15].
In a study by Lin HS et al., [2] sensitivity of FNAC for the diagnosis of FVPTC was only 25% compared to 74% for the classic PTC. There are two reasons for the low sensitivity of FNAC in its diagnosis. One is FVPTC has features in common with benign and neoplastic follicular lesions because of the presence of colloid and monolayered sheets of follicular cells. Second, FVPTC show very few nuclear features of classic PTC. Most of the cases in our study were initially misdiagnosed as follicular neoplasm and adenomatous goiter. This may lead to inadequate surgical treatment like lobectomy and isthmusectomy. No well-defined minimal cytological criteria for the diagnosis of FVPTV in FNAC has been established [4]. This underscores the significance of increasing the accuracy of FNAC in the diagnosis of FVPTC.
Aron et al., [16] in their study stressed that syncytial clusters , microfollicular pattern, chromatin clearing and nuclear grooves were significant features to the diagnosis of FVPTC. Nucleomegaly was seen in all of their cases. In a study by Wu et al., [4] flat syncytial sheets, nuclear enlargement and fine chromatin were seen in all cases of FVPTC along with thick colloid in 20/29 cases. These syncytial sheets showed branching with nuclear crowding compared to honeycomb pattern of colloid nodule. In our study microfollicular and syncytial clusters were the predominant patterns while thick colloid was seen in 16 cases. Fine powdery chromatin, anisonucleosis and nucleomegaly were seen in all of our cases.
According to Powari et al., [17] FVPTC should be considered in the diagnosis if the smears show high cellularity, syncytial clusters and follicular arrangement and thick colloid. Shih SR et al., [15] concluded in their study that it was difficult to differentiate FVPTC from classic PTC in FNAC and when follicular structures were seen in smears, careful search for nuclear features should be done. In the present study papillary structures were seen in 7 cases all were diagnosed as classic PTC even after review.
In a study by Gallagher et al., [8] most of the smears were highly cellular and the neoplastic cells formed follicles, tubules, rosettes, papillary structures and the nuclei were twice the size of red blood cells, hyperchromatic and had smooth contours. Yan et al.,[18] in their study showed that branched sheets of follicular cells seen in low-power examination of Diff-Quick-stained smears are clue to the quick diagnosis of FVPTC and the diagnosis can be confirmed by further evaluation of nuclei in Papanicolaou-stained smears. In our study we analysed papanicoloau stained slides along with H&E slides and identified nuclear grooves in 20 cases, pseudoinclusions in 12 cases.
We conclude that cellular smears with features as observed in our case like microfollicular pattern, syncytial clusters, fine powdery chromatin, anisonucleosis and nucleomegaly should alert the pathologist to look carefully for other more specific features like nuclear grooves and nuclear pseudoinclusions. This approach will help in avoiding misdiagnosis of FVPTC and would aid in choosing the right treatment modality.