Background: The suprascapular notch, a depression on the lateral part of the superior border of the scapula, medial to the coracoid process, is bridged by the superior transverse scapular ligament, which is sometimes ossified and the foramen which is thus completed, transmits the suprascapular nerve to the supraspinatus fossa. Variations in the morphology of suprascapular notch have been identified as one of the causes of suprascapular nerve entrapment. Rengachary et al. classified this notch into six types, based on its shape.
Aim of Study: To study morphological variations of suprascapular notch in Indian dry scapulae and to analyze the incidence of completely ossified superior transverse scapular ligament with other ethnic populations which have been cited earlier.
Materials and Methods: A total of 400 human dry scapulae which were obtained from the Department of Anatomy of selected eight medical colleges were analyzed. The type of suprascapular notch was noted and it was recorded as per the description given by Rengachary et al. The results of the present study were compared with the results of previous authors in different populations.
Results: In our study, out of 400 scapulae, 40 (10%), were identified to have completely ossified superior transverse scapular ligaments. The frequencies of various types of suprascapular notches were: Type I -20%, Type II -10%, Type III -52%, Type IV -4%, Type V -4%, Type VI -10%.
Conclusion: Since the suprascapular nerve entrapment syndrome might be caused by complete ossification of superior transverse scapular ligament with formation of suprascapular foramen and other morphometric variations of suprascapular notch, the knowledge on such variations is essential for clinicians, for making a proper diagnosis and for planning the most suitable surgical intervention.
Introduction
The suprascapular notch (SSN) is a depression on the lateral part of the superior border of the scapula, medial to the coracoid process. This structure is bridged by the superior transverse scapular ligament (STSL), which is sometimes ossified and the foramen which is thus completed, transmits the suprascapular nerve (SN) to the supraspinatus fossa [1,2]. Suprascapular nerve supplies motor branches to the muscles supraspinatus and infraspinatus, and sensory branches to rotator cuff muscles, and ligamentous structures of the shoulder and acromioclavicular joints. Accordingly, this notch is an important landmark of the suprascapular nerve during arthroscopic shoulder operations [3,4].
Furthermore, variations in the morphology of suprascapular notch have been identified as one of the causes of suprascapular nerve entrapment [5]. Rengachary et al., [6–8], classified this notch into six types, based on its shape and they also stated that the size of the suprascapular notch played a role in the predisposition for suprascapular nerve entrapment. In their opinion, a small notch gave a greater chance of a nerve impingement than a large one. One of the clinically most important places on the scapula is the suprascapular notch. The suprascapular nerve and vein run below this superior transverse scapular ligament, and above the ligament passes suprascapular artery [9–12].
Morphological variations of the suprascapular notch are veryimportant clinically for possible predisposing factors, for compression of the suprascapular nerve in this region. In the whole population, approximately 1–2% all shoulder pain is caused by the suprascapular nerve entrapment syndrome [13]. Suprascapular nerve entrapment was first described by Kopell and Thompson [14]. The result of suprascapular nerve entrapment is weakness of the arm, difficulty in external rotation and abduction, and then, atrophy of the infraspinatus and supraspinatus muscles. This entrapment syndrome is most frequently found in volleyball players and athletes who repeatedly experience stress on their shoulder. These include baseball players, weight lifters, tennis players, fencers, hunters using bows, dancers, figure skaters and individuals with occupations which require a lot of overhead work which requires extreme abduction and external rotation [15–19].
The suprascapular notch type, apart from the anatomical interest, may have some clinical significance for suprascapular nerve entrapment [20–22]. The size and shape of the suprascapular notch may be a factor in suprascapular nerve entrapment, because narrow suprascapular notches have been found in patients with this syndrome [23–28].
Aim of study
To study morphological variations of suprascapular notch in Indian dry scapulae and to analyze the incidence of completely ossified superior transverse scapular ligament with other ethnic populations which have been cited earlier.
Materials and Methods
A total of 415 human scapulae of unknown ages and sexes, which were collected from the Department of Anatomy of Mahatma Gandhi Medical College and Research Institute and other medical colleges in and around Pondicherry, India, were analyzed after obtaining consents and permissions from the heads of the institutions and anatomy departments for the study. Broken scapulae which were 15 in number, were excluded. The study was conducted between March 2013 and September 2013. Representative photographs of various types of suprascapular notches along the superior borders of the scapulae, were taken by using a digital camera (Sony 12.1 Mega pixels) and they were documented.
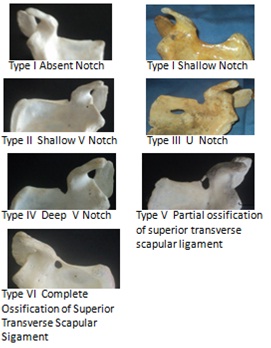
We followed the classification which was stated by Rengachary et al., [6–8]: Type I –complete absence of notch. Type II -wide blunted V shaped notch occupying a third of superior border of scapula. Type III -symmetrical and U shaped notch with parallel lateral margins. Type IV -small V shaped notch. Type V -U shaped notch with partial ossification of medial part of suprascapular ligament. Type VI -complete ossified ligament with bony foramen of variable size. He also suggested that various transitions existed between these types of notches.
Results
In the present study out of 400 scapulae, 40 (10%) scapulae were found to have completely ossified superior transverse scapular ligaments. Representative photographs of various notch types in our study are shown in [Table/Fig-1]. On analysis of morphological variations of suprascapular notch, we found: Type I -20%, Type II -10%, Type III -52%, Type IV -4%, Type V- 4%, Type VI -10%. [Table/Fig-2].
Representative photographs of the various notch types from our study, as per Rengachary’s classification
The frequency of various types of suprascapular notch as per Rengachary’s classification in our study [6–8]
| Type | Type I | Type II | Type III | Type IV | Type V | Type VI |
|---|
| Number of Scapulae | 80 | 40 | 208 | 16 | 16 | 40 |
| Percentage | 20% | 10% | 52% | 4% | 4% | 10% |
Discussion
The incidence of completely ossified superior transverse scapular ligaments in our present study was 10% and ranges of 10.57% and 12.6% have been reported by Vandana and Sudha et al., [36] and Jadhave et al., [28] [Table/Fig-3]. However, Muralidhar Reddy et al., [32], G Soni et al., [28], Vyas et al., [33], Kalpana et al., [34] and Pragna et al., [35] have reported lesser incidences, i.e., 1.93% to 3.75%. The incidence of suprascapular foramen in Indian dry scapulae was relatively significant in comparison to those seen in other ethnic studies. This observation was significant as compared to those of other studies done on various ethnic populations. It has been reported to be more in Brazilian (30.76%) population, followed by Turkish (12.5%) and American (6.5%) populations [Table/Fig-4].
Comparative statement of incidence of completely ossified superior transverse scapular ligament in Indian population studied by different authors
| Serial No. | Author (year of study) | Total No. of Scapulae Studied | No. Scapulae with suprascapular foramen | (n=17) Percentage |
|---|
| 1 | G Soni [28] | 100 | 3 | 3% |
| 2 | Khan M A et al., [29] | Single case report | | |
| 3 | Das et al., [30] | Single case report | | |
| 4 | Iqbal et al., [31] | 250 | 0 | 0% |
| 5 | Muralidhar Reddy [32] | 104 | 2 | 1.93% |
| 6 | Vyas et al., [33] | 300 | 11 | 3.67% |
| 7 | Kalpana et al., [34] | 100 | 2 | 2% |
| 8 | Pragna et al., [35] | 80 | 3 | 3.75% |
| 9 | Vandana and Sudha et al., [36] | 134 | 17 | 12.6% |
| 10 | Jadhave et al., [25] | 350 | 37 | 10.57% |
| 11 | Present study | 400 | 40 | 10% |
Comparative statement of Incidence of suprascapular foramen in different population studied by different authors
| Serial No | Author | Population | Percentage of suprascapular foramen |
|---|
| 1. | Kajava [37] | Finnish (133) | 1.5% |
| 2. | Olivier [38] | French | 5-6.5% |
| 3. | Vallois [39,40] | French (200) Italian (200) | 6.5% 6.1% |
| 4. | Ticker et al., [41] | American (79) | 1.27% |
| 5. | Edelson [42] | American (700) | 3.7% |
| 6. | Natsis et al., [43] | Greek (423) | 6% |
| 7. | Sinkeet et al., [44] | Kenyan (138) | 4% |
| 8. | Urgüden et al., [45] | Turkish (120) | 6% |
| 9. | Bayramoglu et al., [46] | Turkish (36) | 12.5% |
| 10. | Wang HJ et al., [47] | Chinese (295) | 1.36% |
| 11. | DJ Gray [48] | American & Europeans (1,151) | 6.34% |
| 12. | DJ Gray [48] | Brazilian (221) | 30.76% |
| 13. | Poirier and Charpy et al., [50] | French(60) | 5% |
| 14. | Osuagwu et al., [51] | Nigerian | Single case report |
| 15. | R Shane et al., [26] | American (79) | 3.7% |
| 16. | Hrdicka [21] | Native America (2792) | 2.1-2.9% |
| 17. | Rengachary et al., [6–8] | American (211) | 4% |
| 18. | M. Polguj et al., [13] | Poland(86) | 7% |
| 19. | Paolo Albino et al., [27] | Italian (500) | 3.6% |
| 20. | Present study | Indian (400) | 10% |
Ticker et al., [41] classified suprascapular notch on basis of morphological appearance as U and V. Iqbal et al., [21] reported three types of suprascapular notches, based on their shapes, ‘U’, ‘V’, ‘J’ on gross examination, following the observations cited by Bayramoglu et al., [46], Hrdicka [21]. Nastis et al., [43] distinguished V notch on the basis of vertical and transverse diameter measurements and Polguj et al., [13] used geometrical parameters for assessment of V shape suprascapular notch. In our present study, we applied the classification of six types of suprascaular notches, which was stated by Rengachary et al., Morphological classification of suprascapular notch in the present study represented Type III (52%) more, followed by Type I, Type IV and Type VI. Since no uniform standard of classification was followed by different authors, it was difficult to do a reasonable comparative study on the reports of various authors. However, we compared our results with those of few authors who also followed Rengachary’s classification [Table/Fig-5]. Our results were in accordance with reports of Murlalidhar et al., in Indian population and similar findings on Americans, Kenyans and Italians, which were reported by Rengachary et al., [6–8], Sinkeet et al., [44] and Paolo et al., [27].
Frequency of various types of suprascapular notch (SSN) in different populations
| Numbers | Population (n) | Type I | Type II | Type III | Type IV | Type V | Type VI |
|---|
| Rengachary et al., [6–8] | American (211) | 8% | 31% | 48% | 3% | 6% | 4% |
| Sinkeet et al., [44] | Kenyan (138) | 22% | 21% | 29% | 5% | 18% | 4% |
| Muralidhar [32] | Indian (104) | 21.15% | 8.65% | 59.61% | 2.88% | 5.76% | 1.93% |
| Paolo Albino et al., [27] | Italian (500) | 12.4% | 19.8% | 22.8% | 31.1% | 10.2% | 3.6% |
| Present study | Indian (400) | 20% | 10% | 52% | 4% | 4% | 10% |
Conclusion
Since the suprascapular nerve entrapment syndrome might be caused by complete ossification of superior transverse scapular ligament with formation of suprascapular foraman and other morphometric variations of suprascapular notch, the knowledge on such variations is essential for clinicians, for making a proper diagnosis and for planning the most suitable surgical interventions. Further detailed ventures like: (a) clinical screening of high risk population by specialists of community medicine, sports medicine, orthopaedicians and general surgeons for the incidence of suprascapular nerve entrapment syndrome, (b) confirmation of suprascapular nerve entrapment syndrome by radiologists by using imaging modalities like MRI, CT and Ultrasound and (c) surgical interventions for either open or laparoscopic suprascapular nerve entrapment syndrome, coupled with histopathological studies on suprascapular nerve may throw fresh information on this issue.
[1]. Aajmani ML, The cutaneous branch of the human suprascapular nerveJ Anat. 1994 185:439-42. [Google Scholar]
[2]. Standring S, Ellis H, Healy J, Johnson D, Williams A, Pectoral girdle,shoulder region and axillaGray’s Anatomy - The Anatomical Basis of Clinical Practice 2005 39th edNew YorkElsevier Churchill Livingstone:821-2. [Google Scholar]
[3]. Bigliani , Dalsey RM, McCann PD, April EW, An anatomical study of the suprascapular nerveArthroscopy 1990 6:301-5. [Google Scholar]
[4]. Shishido H, Kikuchi S, Injury to the suprascapular nerve during shoulder joint surgery: an anatomical studyJ Shoulder Elbow Surg 2001 10:372-6. [Google Scholar]
[5]. Callahan JD, Scully TB, Shapiro SA, Worth RM, Suprascapular nerve entrapment: a series of 27 casesJ Neurosurg 1991 74:893-6. [Google Scholar]
[6]. Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H, Suprascapular entrapment neuropathy: a clinical, anatomical, and comparative study. Part 1: Clinical studyNeurosurgery 1979 5(4):441-6. [Google Scholar]
[7]. Rengachary SS, Burr D, Lucas S, Hassanein KM, Mohn MP, Matzke H, Suprascapular entrapment neuropathy: a clinical, anatomical, and comparative. Study Part 2: anatomical studyNeurosurgery 1979 5(4):447-51. [Google Scholar]
[8]. Rengachary SS, Burr D, Lucas S, Brackett CE, Suprascapular entrapment neuropathy: A clinical, anatomical, and comparative study. Part 3Neurosurgery 1979 5(4):452-5. [Google Scholar]
[9]. Barwood SA, Burkhart SS, Lo IK, Arthroscopic suprascapular nerve release at the suprascapular notch in a cadaveric model: an anatomic approachArthroscopy 2007 23:221-5. [Google Scholar]
[10]. Harmon D, Hearty C, Diameter of suprascapular nerve in the suprascapular notchPain Phys 2008 11:263-4. [Google Scholar]
[11]. Lafosse L, Tomasi A, Corbett S, Baier G, Willems K, Gobezie R, Arthroscopic release of suprascapular nerve entrapment at the suprascapular notch: technique and preliminary resultsArthroscopy 2007 23:34-42. [Google Scholar]
[12]. More KL, Dalley AF, Agur AM, Clinical oriented anatomy 2010 6th Ed edPhiladelphiaLippincott Wiliams and Wilkins [Google Scholar]
[13]. Polguj M, Jdrzejewski K.S, Podgórski M, Topo M, Correlation between morphometry of the suprascapular notch and anthropometric measurements of the scapulaFolia Morphol 2011 70(2):109-15. [Google Scholar]
[14]. Kopell HP, Thompson WAL, Pain and the frozen shoulderSurg Gynecol Obstet 1959 109:92-6. [Google Scholar]
[15]. Antonoiou J, Tae SK, Wiliams GR, Bird S, Ramsey MJ, Iannotti JP, Suprascapular neuropathy. Variability in the diagnosis, treatment, and outcomeClin Orthop Rel Res 2001 386:131-8. [Google Scholar]
[16]. Cummins CA, Messer TM, Nuber GW, Suprascapular nerve entrapmentJ Bone Join Surg 2000 82-A:415-24. [Google Scholar]
[17]. Edeland HG, Zachrisson BE, Fracture of the scapular notch associated with lesion of the suprascapular nerveActa Orthop Scand 1975 46(758):763 [Google Scholar]
[18]. Ferretti A, Cerullo G, Russo G, Suprascapular neuropathy in volleyball playersThe Journal of Bone Joint Surg AM 1987 69:260-3. [Google Scholar]
[19]. Vastamaki M GH, Suprascapular nerve entrapmentClin Orth Rel Res. 1993 297(135):143 [Google Scholar]
[20]. Bhatia DN, de Beer JF, van Rooyen KS, du Toit DF, Arthroscopic suprascapular nerve decompression at the suprascapular notchArthroscopy. 2006 22(1009):1013 [Google Scholar]
[21]. Hrdicka A, The scapula: visual observationsAm J Phys Antropol. 1942 29(73):94 [Google Scholar]
[22]. Zehetgruber H, Noske H, Lang T, Wurnig C, Suprascapular nerve entrapment: a meta-analysisInt Orthop. 2002 26:339-43. [Google Scholar]
[23]. Ofusori D, Ude R, Okwuonu Ch, Adesanya O, Complete absence of the suprascapular notch in a Nigerian scapula: a possible cause of suprascapular nerve entrapmentInt J Shoul Surg. 2008 2(85):86 [Google Scholar]
[24]. Yücesoy C, Akkaya T, Özel O, Cömert A, Tüccar E, Bedirli N, Ultrasonographic evaluation and morphometric measurements of the suprascapular notchSurg Rad Anat 2009 31(409):414 [Google Scholar]
[25]. Jadhav SD, Patil RJ, Roy PP, Ambali MP, Doshi MA, Supra scapular foramen in Indian dry scapulaeNJCA. 2012 1(3):133-5. [Google Scholar]
[26]. Tubbs R. Shane, Nechtman Carl, D’Antoni Anthony V, Shoja Mohammadali M, Mortazavi Martin M, Loukas Marios, Rozzelle Curtis J, Spinner Robert J, Ossification of the suprascapular ligament: A risk factor for suprascapular nerve compression?Int J Shoulder Surg. 2013 7(1):19-22. [Google Scholar]
[27]. Albino Paolo, Carbone Stefano, Candela Vittorio, Arceri Valerio, Vestri Anna Rita, Gumina Stefano, Morphometry of the suprascapular notch: correlation with scapular dimensions and clinical relevanceBMC Musculoskelet Disord. 2013 14:172 [Google Scholar]
[28]. Malik G, Soni VS, Shukla L, Chabbra S, Gaur N, Morphometric Analysis of the Suprascapular NotchThe Internet Journal of Biological Anthropology 2012 5(1)DOI:10.5580/2B19 [Google Scholar]
[29]. Khan MA, Complete ossification of the suprascapular transverse ligament in an male adultInt J Morphol. 2006 24(2):195-6. [Google Scholar]
[30]. Das Srijit, Suri Rajesh, Kapur Vijay, Ossification of Superior Transverse Scapular Ligament and its Clinical ImplicationsSultan Qaboos Univ Med J 2007 August 7(2):157-60. [Google Scholar]
[31]. Iqbal K, Iqbal R, Khan SG, Anatomical variations in shape of suprascapular notch of scapulaJ Morphol Sci 2010 27(1):1-2. [Google Scholar]
[32]. Sangam Muralidhar Reddy, A Study on the Morphology of the Suprascapular Notch and Its Distance from the Glenoid CavityJ Clin Diagn Res 2013 7(2):189-92. [Google Scholar]
[33]. Vyas KK, Rajput HB, Zanzrukiya KM, Suttarwala I, Sarvaiya BJ, Shroff BD, An osseous study of suprascapular notch and various dimentions of safe zone to prevent suprascapular nerve injuryIndian Journal of Applied Basic Medical Sciences 2013 15(20):27 [Google Scholar]
[34]. Karam Kalpana Thounaojam Renuca, Singh N. Saratchandra, Ossification of transverse scapular ligament. / Volume 2/ Issue 12/ March 25, 2013: 1790-1791Journal of Evolution of Medical and Dental Sciences 2013 2(12):1790-1. [Google Scholar]
[35]. Patel Pragna, Patel S V, Patel S M, Jotania Badal, Chavda Sanjay, Patel Dhara, Study of variations in the shape of the suprascapular notch in Dried Human ScapulaInt J Biol Med Res 2013 4(2):3162-4. [Google Scholar]
[36]. Vandana R, Patil Sudha, Morphometric study of Suprascapular NotchNational Journal of Clinical Anatomy 2013 2(3):140-44. [Google Scholar]
[37]. Kajava Y, Uber den Schultergiirtel der FinenAnn Acad Sci Fenn, Series A 1924 21(5):1-69. [Google Scholar]
[38]. Olivier G, Pratique anthropologiqueLe scapulum 1960 ParisVigot Freres [Google Scholar]
[39]. Vallois H.V, L’os acromial dans les races humaineL’ Anthropologie 1925 35:977-1022. [Google Scholar]
[40]. Vallois HV, Variations de la cavite glenoide de l’ omoplateSoc Biol Comptes Rendus Hebdomadaires Seances et memoires 1926 94(559):560 [Google Scholar]
[41]. Ticker JB, Djurasovic M, Strauch RJ, April EW, Pollock RG, Flatow EL, The incidence of ganglion cysts and other variations in anatomy along the course of the suprascapular nerveJ Shoulder Elbow Surg 1998 7(5):472-8. [Google Scholar]
[42]. Edelson JG, Bony bridges and other variations of the suprascapular notchJ Bone Joint Surg Br 1995 77:505-6. [Google Scholar]
[43]. Natsis K, Totlis T, Tsikaras P, Appell HJ, Skandalakis K, Proposal for classification of the suprascapular notch: a study on 423 dried scapulasClin Anat 2007 20:135-9. [Google Scholar]
[44]. Sinkeet SR, Awori KO, Odula PO, Ogeng’o JA, Mwachaka PM, The Suprascapular notch: its Morphology and distance from the glenoid cavity in a Kenyan populationFolia Morphol 2010 69:241-5. [Google Scholar]
[45]. Urgüden M, Ozdemir H, Dönmez B, Bilbasar H, Oguz N, Is there any effect of suprascapular notch type in iatrogenic suprascapular nerve lesions? An anatomical studyKnee Surg Sports Traumatol Arthrosc 2004 12(241):245 [Google Scholar]
[46]. Bayramoglu A, Demiryürek D, Tüccar E, Variations in anatomy at the suprascapular notch possibly causing suprascapular nerve entrapment: An anatomical studyKnee Surg Sports Traumatol Arthrosc 2003 11:393-8. [Google Scholar]
[47]. Wang HJ, Chen C, Wu LP, Pan CQ, Zhang WJ, Li YK, Variable morphology of the suprascapular notch: an investigation and quantitative measurements in Chinese populationClin Anat 2011 24(1):47-55. [Google Scholar]
[48]. Gray DJ, Variations in human scapulaeAmerican Journal of Physical Anthropology 2013 29(1):57-72.1942 [Google Scholar]
[49]. Silva JG, Abidu-Figueiredo M, Fernandes RMP, Aureliano-Rafael F, Sgrott EA, Silva SF, High incidence of ossification of superior transverse scapular ligament in Brazilians and its clinical significanceInt J Morphol 2007 25(4):855-9. [Google Scholar]
[50]. Poirier P, Charpy A, Traité d’anatomie humaine 1911 3rd edParis [Google Scholar]
[51]. Osuagwu FC, Imosemi IO, Shokunbi MT, Complete ossification of the superior transverse scapular ligament in a Nigerian male adultInt J Morphol 2005 23(2):121-2. [Google Scholar]