The present work on the intra-renal apical arterial segmental pattern of the human kidneys and its variations was undertaken because of its urosurgical importance in making a relatively bloodless surgical approach to the kidneys and to save the healthy renal tissue in partial nephrectomy. Anatomical knowledge of vasculature of human kidney and its segments is of great clinical significance in partial resection and transplantation of the human kidney. Advances made in urological surgery raised an interest to study various renal segments on the basis of branching pattern of renal arteries in greater detail. Renal arteries and veins are always described separately in anatomical textbooks, without giving details of mutual relationship of these vessels in details, Brodel [1]. Anson [2] have discussed the important branches of the renal arteries and corresponding venous tributaries. Most textbook and many publications still misrepresent the internal anatomy of the kidney, which tends to perpetuate old misconception, Hodson [3,4].
Many surgeons in treatment of renal tuberculosis and calculus now advocate partial nephrectomy. Control of hemorrhage is one of the technical difficulties of this operation and of more established procedure of nephrolithotomy in which failure of homeostasis necessitates nephrectomy. Knowledge of the vascular pattern of kidney greatly assists the surgeon in carrying out these operations, but it is neither complete nor readily accessible. Keeping in view, the academic as well as the applied importance of the subject, the present work was undertaken to study the vascular pattern in kidney specimens obtained from subjects of Indian origin. The vascular pattern was studied in the 3-D corrosion endocasts and a comparable series of angiograms obtained from the corresponding kidney specimens. The angiography of renal vasculature provides a clear view of the vascular anatomy, whereas the corrosion casts, on account of their minimal brittleness and easy handling unfold the vascular pattern in a 3-D set up.
Materials and Methods
After ethical clearance from concerned authorities of AIIMS, New Delhi, India, the present study was conducted on 40 kidneys obtained from 20 autopsies done at AIIMS mortuary. Autopsy Sample consisted of 15 males and 5 females and were in the range of 20-25 years. The commonest cause of death of these individuals was road traffic accident (RTA). Case displaying abdominal trauma, evidence of previous surgical intervention in abdomen, burning, drowning, hanging and fall from height, decomposed bodies, etc were excluded from the study. Specimens were collected within 24 hours of death. The specimen was then washed in running tap water and a cannula was secured in position by tying with thread. The kidney was then flushed with normal saline solution to remove blood clots.
For angiography, the radio-opaque dye – omnipaque ( a non-ionic contrast medium) with dilution of 2:1 was used. Around 10-15 ml of the dye was injected into the renal artery under fluoroscope. After injecting the dye, the specimens were X-rayed for obtaining the angiographic pictures. After this procedure, the specimens were washed with running water.
For corrosion cast technique, coloured acetate butyrate (CAB) granules were immersed in acetone (1:2) for 3 days to obtain a homogenous solution. Red coloured solution was injected by a 20 ml syringe under constant pressure into the renal arteries of both the sides. Around 10-15 ml of the solution was injected into the renal arteries. The specimens were kept in a deep freezer overnight at –250C for the solidification of the solution into minute arterioles. After 24 hours, the specimens were washed under tap water for half-an-hour and subsequently immersed in 50% hydro-chloric acid (HCL) for digestion of the parenchymatous tissue. This was followed by washing of the specimens in tap water and prunning with fine forceps. The endocasts thus obtained were kept in dust free environment on blotting paper for further observations.
The vascular pattern of the kidney specimens was studied in the angiographic pictures and a comparison was drawn with the pattern seen in the corresponding endocasts.
Results
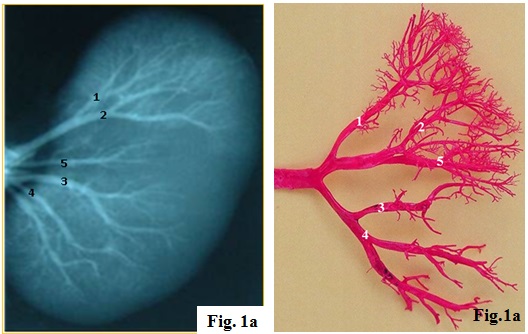
The investigation includes 40 arteriograms and endocasts of normal human kidney, which in the present study confirmed both the presence of segmental arrangement of the renal arteries and absence of collateral circulation between the segmental arrangements of the renal artery thereby indicating them as end arteries. Renal artery is a branch of aorta, which in turn divided into anterior and posterior division. Anterior division further divides into upper and lower branch. Upper branch give origin to apical and upper segmental arteries while lower division gives origin to middle and lower segmental arteries. In the present study, the arteriogram showed that there was a general pattern of the division of the renal artery. The renal artery was divided into anterior and posterior divisions. The anterior division gives apical, upper, middle and lower segmental branches while the posterior division continued as posterior segmental artery [Table/Fig-1a,1b]. The arteriogram showed that there was no anastomosis between the segmental arteries.
Gross photographs showing arterial supply of human kidney by arteriogram. Note the normal pattern of blood supply of human kidney. 1: Apical segmental artery (ASA), 2: upper segmental artery (USA), 3: middle segmental artery (MSA), 4: lower segmental artery (LSA), 5: posterior segmental artery (PSA)
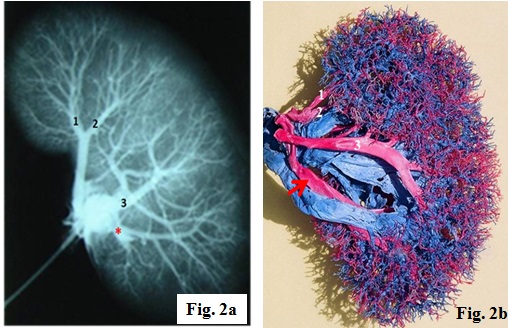
The ASA supplies the apical segment of the kidney and its origin was observed to be variable. In 60% (24/40) cases it originated as a common stem along with USA [Table/Fig-1a,b] while in 40% (16/40) cases it took origin as independent artery from renal artery [Table/Fig-2a,2b]. The USA supplied the upper anterior 1/4th surface of the kidney the area above the hilum. In 60% (24/40) cases USA originated as a common stem with ASA and then gave anterior and lateral branches to supply the whole of the upper pole. In 40% (16/40) cases the USA originated from the renal artery.
Gross photographs showing arterial supply of human kidney by arteriogram. 1: Apical segmental artery (ASA), 2: upper segmental artery (USA), 3: middle segmental artery (MSA), Red arrow and *: Independent origin of lower segmental artery (LSA) from anterior division of renal artery
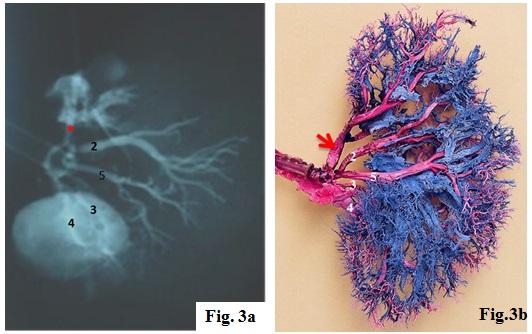
MSA mainly supplies the region between the upper and lower poles. In 50% (20/40) cases the MSA was observed as a branch of anterior division of the renal artery. In 50% (20/40) cases, it originated with LSA. Lower segmental artery originated from the lower branch of anterior division as has been observed in the present study. In 50% (20/40) cases it took origin with MSA. In 45% (18/40) cases it was observed as a separate branch from the main renal artery [Table/Fig-3a,3b] while in 5% (2/40) cases there were two renal arteries supplying the lower pole of the kidney [Table/Fig-1a]. PSA supplied the posterior surface of the kidney except upper and lower polar segment which were supplied by branches of apical and lower segmental artery in all the cases. In this study it was seen that PSA was comparatively small and was the continuation of the posterior division of the renal artery [Table/Fig-1b].
Gross photographs showing arterial supply of human kidney by arteriogram. 2: upper segmental artery (USA), 3: middle segmental artery (MSA), 4: lower segmental artery (LSA), 5: posterior segmental artery (PSA), Red arrow and *: Apical segmental artery (ASA) taking origin directly from renal artery
Discussion
The present study was focused on the vascular pattern of the kidney particularly pertaining to the main segmental branch of the renal artery. The present study has suggested a no. of findings about the renal vascular pattern, which possibly have practical applications in the segmental and partial resection of the kidney. The classical distribution of the renal arteries within the kidney as described in the text books form a general pattern which is constant and upon this is founded the division of renal parenchyma into five segments, i.e. Apical, upper, middle, lower and posterior segments. The area of kidney tissue which is supplied by a segmental artery is known as renal segment. The segmental arteries are supposed to be the end arteries, Hunter [4] and have also been observed in the present study. On the basis of branching pattern of the renal artery, Grave [5] described five segmental branches of the renal artery. Longia [6] on the other hand, in his observation of corrosion casts of human kidney, found variation in the branching pattern of the renal artery. According to his observations, in 46% kidney casts there were four renal segmental arteries probably due to either fusion of apical segmental artery and upper segmental artery or middle segmental artery and lower segmental artery or due to absence of ASA.
But in the present study five definite vascular segments were present in all the kidneys. The apical segment was present on the anterior and posterior surface in 80% cases in the present study and was restricted to the anterior surface only in 20% cases. This observation of the presence of apical segment and its distribution on the anterior and posterior surface was similar to the observation made by Grave [5]. Di-Dio [7] had also studied the vascular segments by corrosion casts and identified five arterial anatomico surgical segments. But he proposed different nomenclature than what has been described by previous worker. He named them superior, inferior and posterior and between superior and inferior he named antero-superior and antero-inferior, which seem to correspond with present upper and middle segments.
In the present study, there was a common origin of branches to apical and upper segments in 60% cases [Table/Fig-1a]. In the present study the upper and apical segments were present on the anterior surface of the upper pole and the upper central part of the kidney above in the hilum. The middle segmental artery was also seen on the anterior surface in the lower central part between upper segment above and lower segment below in all the cases. These findings were also in concurrence with the findings of Kher [8]. Di-Dio [7]. The posterior segmental artery was present on the posterior surface between the apical segment above and lower segment below and supplied entire posterior surface except a small portion of the upper and lower pole. This segment was very small in two cases in the present study. The present findings were in accordance with previous study, in which they used corrosion cast technique Verma [9]. The new techniques which are employed in renal surgery mainly depend upon the segmental resection, namely the wedge–type resections, if the disease affects the upper or the lower segments. But for the mid-portion lesions, either the enucleating technique or partial nephrectomy is indicated, although they are obviously limited to the tumours and they may be employed in other conditions in which there is a minimal loss of the renal functions Raghavendra [10].
The lack of arterial anastomosis in the neighbouring segments will affect only the affected segment and it will neither produce ischemia nor interfere with the blood supply of the neighbouring segments. This lack of the arterial anastomosis will render the technique of the resection easier, since the field of operation will be relatively bloodless, following the ligation of the segmental artery which supplies the area of the operation. It should be kept in mind that the origins of the segmental arteries are accessible. In majority of the cases, they are easily seen in the hilum and they are often at the points which are near to the aorta. This is of practical value, since the segmental resection is best carried out from the hilum towards the periphery. It is evident from the present study that the renal artery mostly shows a segmental branching pattern with one segmental branch being destined to supply particular area of renal parenchyma without effective anastomosis between terminal branches of segmental arteries.
Conclusion and Clinical Significance
Anatomical knowledge of vasculature of human kidney and its segmental distribution plays an important role in partial resection and transplantation procedures as controlling the hemorrhage is one of the technical skills, otherwise uncontrolled bleeding could even necessitate nephrectomy. Partial or segmental resection of the kidneys will help in the further development of different techniques for the removal of calculi or any affected part of kidneys. This will also help in partial renal transplantation surgeries with end-to-end anastomosis of the resected part of the kidney. There is lot of variation in their course and exact point-of-origin of the arterial segments of the kidney. After the advent of renal segments, the urological complications which followed partial nephrectomy have considerably reduced. Nephrectomy or the total removal of a kidney will no longer be performed, if minor procedure can offer a better prospect. Each & every fragment of the healthy, functional renal tissue should be preserved, provided that it has an arterial supply, a venous drainage and a urinary exit.