Re – treatment of a Two-rooted Maxillary Central Incisor – A Case Report
Roopadevi Garlapati1, Bhuvan Shome Venigalla2, Rammohan Chintamani3, Jayaprakash Thumu4
1Senior Lecturer, Department of Conservative Dentistry and Endodontics,Sibar Institute of Dental Sciences, Guntur, Andhra Pradesh, India.
2Professor, Department of Conservative Dentistry and Endodontics,Sri Sai College of Dental Surgery, Vikarabad, Andhra Pradesh, India.
3Reader, Department of Conservative Dentistry and Endodontics,Sri Sai College of Dental Surgery, Vikarabad, Andhra Pradesh, India.
4Professor, Department of Conservative Dentistry and Endodontics,Sibar Institute of Dental Sciences, Guntur, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Roopadevi Garlapati, Senior Lecturer, Department of Conservative Dentistry and Endodontics, Sibar Institute of Dental Sciences, Takkellapadu, Guntur-522509, Andhra Pradesh, India.
Phone: 09052073309,
E-mail:dr.rupagarlapati@gmail.com
This case report is on endodontic retreatment of a maxillary central incisor with two roots. A twenty-year-old male patient presented with pain in maxillary left central incisor. Radiographic examination showed an incompletely filled canal and an additional palatal root with periapical radiolucent lesion. Conventional cleaning and shaping of both the roots, i.e., buccal and additional palatal root canals was performed and obturation was done. After one year recall examination, the tooth was asymptomatic and periapical lesion had healed.
Additional root, Maxillary central incisor, Root canal
Case Report
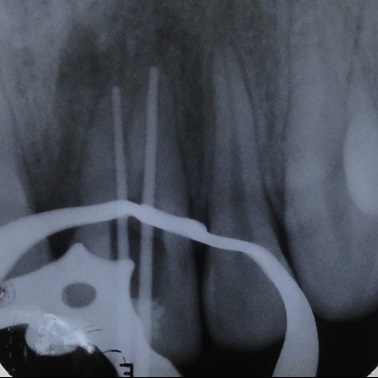
A 20-year-old male patient was referred to the Department of Conservative Dentistry and Endodontics with pain and labial swelling in the upper anterior region since two weeks. The pain was continuous and throbbing. His past dental history revealed that he visited the dentist two months ago with a complaint of pain in the upper front teeth region. Root canal treatment was planned and performed in relation to the maxillary left central incisor. His medical history was non-contributory. On clinical examination all the teeth were normal in number, size and color. A swelling was observed on the labial aspect of maxillary left central incisor and the tooth was tender on percussion. A permanent restorative material was seen on the palatal aspect of maxillary left central incisor. Radiographic examination revealed the previous root canal treatment with incomplete obturation and periapical radiolucency. Along the middle third of the root, an abnormal anatomical anomaly was seen which was suggestive of an additional root. Presence of an additional palatal root was confirmed by second intraoral periapical radiograph with altered (mesial tube shift) horizontal angulations [Table/Fig-1]. Based on the above clinical and radiographic findings, maxillary left central incisor was diagnosed as having necrotic pulp and chronic apical periodontitis. A nonsurgical endodontic re-treatment procedure was planned for the maxillary left central incisor to locate the missing root canal and the patient was informed about the procedure.
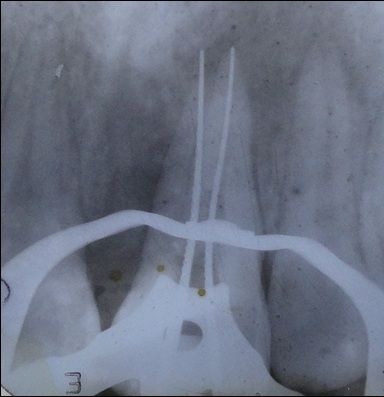
Under rubber dam isolation, the access cavity was re-entered using a No.1015 high speed round diamond bur and the permanent restorative material was removed. Entire gutta-percha was removed from the facial canal with the help of chloroform and alternatively by Hedstrom (H) files. Facial canal was irrigated with saline to flush the gutta-percha and sealer remnants. Entire gutta-percha removal from the facial canal was confirmed by radiographs [Table/Fig-2]. Additional distopalatal canal was located with a DG 16 endodontic explorer using endodontic loupes. For the enhancement of accessibility and instrumentation the access cavity was extended on to the distopalatal aspect. The distopalatal canal was located and the patency was checked with No.15 K-file. Working length was determined by an apex locator (Propex-II, Dentsplymallifer, Ballaigues, Switzerland) and confirmed by files in the radiograph [Table/Fig-3]. Cleaning and shaping was performed by hand instruments with step-back technique using Glyde as a chelating agent and with copious irrigation in between the instrumentation. The facial canal and the distopalatal canal were instrumented up to master apical size of 60 ISO size K-file with alternate irrigation of 3% sodium hypochlorite solution and saline. Finally the canals were rinsed with 2% Chlorhexidine (CHX). Calcium hydroxide paste (RC cal) was used as an intracanal medicament and the access cavity was closed with Zinc oxide eugenol temporary cement. Patient was prescribed antibiotics and analgesics to manage pain and swelling.
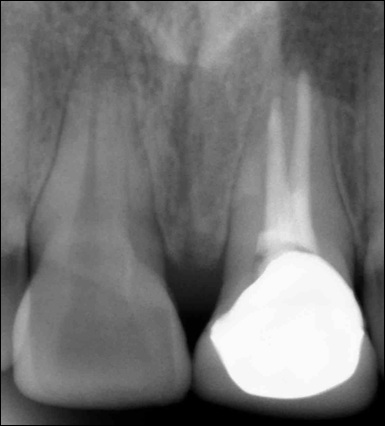
Patient was recalled after one week for further followup. At the second visit patient was totally asymptomatic. Temporary restorative material was removed, facial and distopalatal canals were irrigated and dried with paper points. Master cone radiograph was taken to confirm the length [Table/Fig-4]. Canals were coated with AH Plus sealer and obturation of both the canals was done with gutta-percha and AH Plus as the sealer using cold lateral compaction technique. The access cavity was restored with composite resin (Filtek Z 250, 3M Dental Products) [Table/Fig-5]. After two weeks, the patient was recalled to give metal ceramic crown for maxillary left central incisor for the enhancement of esthetics. Crown preparation was performed in relation to the maxillary left central incisor and impressions were made with a low viscosity material (Aquasil,Dentsply). Patient was recalled after one week for the cementation of crown. Re-treatment of maxillary left central incisor and restoring it with a crown was completed in a period of one month and the patient was periodically reviewed after three months, six months and one year. Patient was asymptomatic during one year follow-up and he was satisfied with esthetics and function. At one year follow-up, a radiograph was taken in relation to maxillary left central incisor, which confirmed the healing of periapical lesion [Table/Fig-6].
Pre-operative radiograph of maxillary left central incisor


Working length radiograph with files placed in two root canals
Post-obturation radiograph of maxillary left central incisor

Radiograph of maxillary left central incisor with crown
Discussion
Maxillary central incisors are usually considered to have single root and one root canal [1]. While some case studies reported with two to four canals, two roots and two root canals [2, 3]. Other variations like fusion, gemination, presence of dens invaginatus are also seen [4]. Usually maxillary central incisor with such variations present with an unusually large crown or defective crown surface either labially or lingually. In the present case, the crown was clinically normal in size and shape.
Sabala et al., reported that root canal aberrations occurring in less than 1% of the cases were 90% bilateral [5]. In the present case, the right maxillary central incisor was also seen with the presence of two roots.
During normal root formation, the Hertwig’s epithelial root sheath (HERS) is bent horizontally at the Cemento Enamel Junction causing the cervical opening of the tooth germ to narrow. Due to any traumatic injury or any unknown factor the fusion of the horizontal extensions of the diaphragm remains incomplete, which leads to the development of accessory root canals opening on the periodontal surface of the root [6].
In order to identify these anomalies or variations the radiographs should be taken in different angulations. Brynolf reported that endodontic diagnosis is correctly obtained 74% of the time with one radiograph and 90% of the time with three radiographs that included an angled view [7]. So, the clinician should always take more than one radiograph from different angulations. Cautiously tracing the outline of the root surface also helps in the diagnosis.
Intraoral radiography is commonly used method for diagnosis and treatment planning in endodontics, which may mislead the clinician into false positive results. So,with the advent of digital radiography and CT Scans the errors were minimized in the clinical cases. In complex root canal anatomy cases, Spiral Computed Tomography can be used as an additional tool [8]. Cone-Beam Computed Tomography (CBCT) is an advanced diagnostic aid which is used in endodontics for diagnosis, treatment planning and for follow-up. Main advantage of using CBCT in endodontics is reduced radiation exposure with added diagnostic information during complex endodontic procedures. CBCT is mainly useful to observe the expansion of periapical lesions, differentiation of periapical lesions, confirming the number of root canals [9,10].
In the present case, 2% Chlorhexidine (CHX) was used as a final irrigating solution, as it has wide range of activity against both grampositive and gram-negative bacteria. CHX is bactericidal, used in endodontics routinely during retreatment procedures, as it adsorbs to dental tissue and mucous membrane, resulting in its prolonged gradual release at therapeutic levels. Many studies reported that CHX has antibacterial substantivity in dentine for up to 12 weeks. Irrigating the root canals with CHX delays the contamination of obturated root canals by bacteria which enters through the coronal restoration or tooth interface [11].
Calcium hydroxide Ca(OH)2 was used as an intracanal medicament of choice because of its effective antibacterial properties and it causes healing of periapical tissues. Calcium hydroxide is a strong base with a high pH of approximately 12.5 -12.8. Ca(OH)2 powder is mixed with saline and is placed as intracanal dressing for few days or weeks. Antibacterial action of Ca(OH)2 is by the ionic dissociation of Ca+2 and OH- ions and their effects on vital tissues, which generates induction of hard tissue deposition and being antibacterial [12].
The major reason for the failure of this case was incompletely obturated facial canal and missed additional distopalatal canal. When a patient reports with persistent pain after endodontic treatment, suspect for missed canals. For locating the orifices of root canal diagnostic aids are very important. These include careful examination of floor of the pulp chamber using sharp explorer, troughing the grooves with ultrasonic tips, staining the pulp chamber with dye and performing champagne bubble test using Sodium hypochlorite (NaOCl). Explore for the missed canals using multiple angled radiographs. As the untreated root canal spaces acts as nidus for bacterial contamination,causing the failure of treatment.
The present case was successfully managed with the help of multiple angled radiographs and proper usage of irrigants and intracanal medicaments which eliminated the drug resistant bacteria during re-treatment procedure. A three dimensional obturation with hermetic seal resulted in success of endodontic treatment. The clinician should have an adequate knowledge about root canal configurations for the better treatment of root canal spaces. If possible advanced diagnostic aids are to be considered in treating such anatomical variations in the root canal configuration.
Discussion
The etiology of endodontic failure is multifactorial, but one of the significant cause may be related to missed root canals. When variations occur in a case, additional care has to be taken to investigate the case clinically and radiographically and treat such cases to avoid post-endodontic flare-ups. For a correct diagnosis, proper treatment planning and finally for the success of the endodontic treatment the clinician should have a thorough knowledge of variations in root canal morphology.
[1]. EA Rodrigues, SJA Silva, A case of unusual anatomy: maxillary central incisor with two root canalsInt. J. Morphol 2009 27:827-30. [Google Scholar]
[2]. Lin Wen –Chun, Yang Shue–Fen, Pai Sheng–Fang, Nonsursgical endodontic treatment of a two-rooted maxillary central incisorJ Endod. 2006 32:478-81. [Google Scholar]
[3]. G Thomas, KM Charlie, B Joseph, M George Rajani, S Mahapatra, Endodontic re-treatment of a maxillary central incisor with two rootsEndod 2012 24:125-8. [Google Scholar]
[4]. P Beltes, Endodontic treatment in three cases of dens invaginatusJ Endod 1997 23:399-402. [Google Scholar]
[5]. Cl Sabala, FW Benenati, BR Neas, Bilateral root or root canal aberrations in a dental school patient populationDiagn Cytopathol 1994 20:38-42. [Google Scholar]
[6]. GS Kumar, rban’s Oral Histology and Embryology Elsevier 2009 12th edition:30-1. [Google Scholar]
[7]. I Brynolf, Roentgenologic periapical diagnosis, IV. When is one roentgenogram not sufficient?Sven TandlakTidskr 1970 63:415-23. [Google Scholar]
[8]. GS Sachdeva, S Ballal, V Gopikrishna, D Kandaswamy, . Endodontic management of a mandibular second premolar with four roots and four root canals with the aid of spiral computed tomography: A case reportDJ Endod 2008 34:104-7. [Google Scholar]
[9]. L Ball Randy, Barbizam Joao V., Cohenca Nestor, RC Brahma, S Mahapatra, Intraoperative endodontic applications of cone-beam computed tomographyJ Endod 2013 39:548-57. [Google Scholar]
[10]. Marion J Jose de Carvalho, Nagata J. Yuri, Santos B. Luis Sa , al et, Cone-beam computed tomography and periapical radiograph limitations in the diagnosis of endodontic complications: A report of clinical casesInternational Journal of Clinical Dentistry. 2013 6:227-35. [Google Scholar]
[11]. Mohamaddi Z., Abott P.V., The properties and applications of chlorhexidine in endodonticsInt Endod 2009 42:288-302. [Google Scholar]
[12]. Z Mohammadi, PMH Dummer, Properties and applications of Calcium hydroxide in endodontics and dental traumatologyInt Endod J 2011 44:697-730. [Google Scholar]