A strategically eminent landmark, the mental foramen (MF) shares its significance in various fields of dentistry. Being defined as- “A funnel like opening on the lateral surface of the mandible at the terminus of the mandibular canal”, it transmits mental nerves and vessels, providing sensory innervations and blood supply respectively [1].
Accurate identification of the mental foramen is important for both diagnostic and clinical procedures. Repeated failures which are witnessed during mental nerve blocks indicate its variability of location in a given population [2, 3]. Its radiographic misdiagnosis as a radiolucent lesion in the apical area of the mandibular premolars can lead to iatrogenic injuries. Treatment concepts for dental implant patients identify mental foramen and its anterior loop as a critical surgical landmark and essential reference point during treatment planning. It has also been acknowledged through various studies, that surgical trauma caused to the mental nerve bundle as a result of inappropriate prior assessment, would result in altered sensation from 8.5% to 24% during periods of upto 3-16 months post-operatively following implant surgeries [4,5].
A survey of published literature, investigated the location of MF directly on dry mandibles or by using radiographs of dry mandibles or patients. Debate initiates, as standard anatomical and radiological textbooks contain conflicting statements on location of MF. Contrasting results over the most common position of the foramen brood over positions between the two premolars and below the apex of second premolar. These, in addition to the illustrating presence of positional variability, also highlight existence of racial variability, as was documented in multiple studies, further intensifying complications of pre-surgical judgment [6–25].
Considering these factors, a retrospective study on the variability of the position of the mental foramen was carried out on standardized orthopantomograms of dentulous patients. Panoramic radiography is a curved plane topographic technique which allows broad coverage of oral structures with low radiation exposures (about 10% of full-mouth radiographs). However, major drawbacks include low image resolution, high distortion, and presence of phantom images. Despite developmental advancements in radiological examinations such as computed tomography, conventional panoramic radiographs are more commonly used, since advances in imaging techniques not only expose the patient to higher doses of radiation, but also are an expensive affair [17–19]. Need for economically reasonable yet accurate radiographical technique continues. This study was done to investigate the position of mental foramen which was relative to the mandibular premolars and the inferior border of the mandible, its bilateral symmetry, gender differences, if any and the presence of the anterior loop.
Materials and Methods
A total of 1123 panoramic radiographs of patients, which were taken for diagnostic purposes at Smile Care Center in Mumbai City (India), over the period which extended from Jan 2009 to Dec 2011, were examined in this study by a single examiner. Of the 1123 radiographs of patients whose ages varied from 18 years to 66 years, 300 radiographs were chosen, which best met the inclusion criteria.
The inclusion criteria were presence of a minimum of 22 teeth, including the lower canines, premolars and first molars, diagnostic images which clearly showed visible and traceable borders of mandible which had acceptable density and contrast, with minimal positioning errors and minimum or no superimposition of structures. Radiographs with mixed, unerupted or incomplete dentitions, and those showing a presence of radio-opaque/ radiolucent pathological lesions in the body of mandible, anywhere in the area which extended from right third molar to the left third molar, were excluded.
Classification of MF, based on interpretation from panoramic radiography, which was stated by Yosue and Brooks [20] is of Four types:
Type I- Mental foramen being continuous with mandibular canal.
Type II- Foramen being distinctly separated from the mandibular canal.
Type III- Foramen being diffused with an indistinct border.
Type IV- Unidentified type, in which the mental foramen could not be identified on panoramic radiographs under ordinary exposures and viewing conditions.
The radiographs in which the mental foramen was difficult to identify (Type IV) under ordinary exposures and viewing conditions were also excluded from examination.
All panoramic radiographs were taken by using Sirona X-ray unit ORTHOPHOS 3 (tube potential: 60-80 kV, tube current: 4-12 mA, focal size: 0.5 mm, exposure time: 11.3 s and magnification factor of 1:1.25) and high quality processing (Sirona Dental Systems, Bensheim, Germany). The values obtained from the panoramic measurements were corrected for their magnifications.
Tracing of the canal upto the foramen, including the anterior loop of the nerve, if it was present, was done on OPGs, viewed on an X-ray viewer. Mandibular plane was drawn by a line which connected the gonion and lowermost point of lower border of mandible was considered as the horizontal reference. Long axes of the premolars served as the vertical references. The position of the image of the mental foramen was recorded according to the categories which were put forward by Jasser and Nwoku [21], which were as follows:-
Position 1: Anterior to the first premolar,
Position 2: Below the first premolar,
Position 3: Between the premolars,
Position 4: Below the second premolar,
Position 5: Posterior to the second premolar,
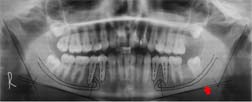
In terms of the perpendicular distance between the arbitrary centre of mental foramen and the reference line [Table/Fig-1,2].
Orthopantomograph of the patient before tracing
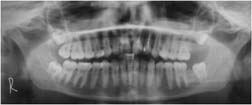
Orthopantomograph after tracing depicting the constructed mandibular plane (red arrow) as vertical reference and the long axis of the two premolars (dotted lines) as the horizontal reference
Few anatomical variations, such as unilateral and bilateral bifid mental nerves which terminate in the respective mental foramen, were gauged by using the mean centre of the two foramina.
The approval for the prerequisites was taken from the ethics committee of Nair Hospital Dental College. The radiographs were investigated and the readings were tabulated for statistical analysis, which was performed using Analyse –it 3 statistical software.
Results
The 300 panoramic radiograph which were evaluated, were grouped into those of 150 males and females each.
The most common position was found to be between the two premolars, i.e. Position 3, in approximately 63% cases, which also showed bilateral symmetry in 45.67% cases. This was followed by position 5, i.e. behind the second premolar, which scored 20.67%.
On assessing the vertical reference, the mean distance from the mental foramen was found to be on an average of 15.39mm from the vertical border of the mandible [Table/Fig-3a,3b], [Table/Fig-4,5].
| Position w.r.t. the long axis | Mean (Std. Deviation) |
|---|
| 1st Premolar | 2nd Premolar |
|---|
| Right | Left | Right | Left |
|---|
| Behind | 9.12 (4.44) | 8.92 (3.99) | 1.25 (2.80) | 1.07 (2.40) |
| Ahead | 5.72 (3.45) | 7.48 (1.58) | 6.10 (3.44) | 5.85 (2.91) |
| Along | 9.23 (3.32) | 4.67 (2.78) | 4.24 (2.85) | 4.57 (2.56) |
| 3 (A) |
(B) Vertical references
[Table/Fig-3a,b] Table showing the mean and the standard deviation values (in mm) and the number and percentage of patients falling within the range of Mean ± Standard Deviation
| Lower border of Mandible |
|---|
| Right | Left |
|---|
| Mean | 15.52 | 15.26 |
| Std. Deviation | 2.74 | 2.89 |
| %Probability | 70.67 | 67.33 |
| 3 (B) |
Frequency and percentage as calculated for the male and female individually for each side and a total value for the whole sample size
| Position | Male | Female | Total |
|---|
| Right Frequency (%) | Left Frequency (%) | Right Frequency (%) | Left Frequency (%) |
|---|
| 1 | 7 (4.67) | 7 (4.67) | 5 (3.33) | 3 (2) | 22 (3.67) |
| 2 | 4 (2.67) | 5 (3.33) | 3 (2) | 2 (1.33) | 14 (2.33) |
| 3 | 100 (66.67) | 90 (60) | 87 (58) | 101 (67.33) | 378 (63) |
| 4 | 11 (7.33) | 17 (11.33) | 20 (13.33) | 14 (9.33) | 62 (10.33) |
| 5 | 28 (18.67) | 31 (20.67) | 35 (23.33) | 30 (20) | 124 (20.67) |
Showing the number and percentage cases showing occurrence on the right and left side under various positions as classified by Jasser and Nwoku [21]
| No. of cases (Percentage) occuring on the left side |
|---|
| Position |
|---|
| Position | 1 | 2 | 3 | 4 | 5 | Total |
|---|
| No. of cases (Percentage) occuring on the Rightside | 1 | 1 | 0 | 6 | 2 | 3 | 12 |
| 3.33% | 0.00% | 2.00% | 0.67% | 1.00% | 4.00% |
| 2 | 0 | 1 | 2 | 2 | 2 | 7 |
| 0.00% | 0.33% | 0.67% | 0.67% | 0.67% | 2.33% |
| 3 | 7 | 5 | 137 | 11 | 27 | 187 |
| 2.33% | 1.67% | 45.67% | 3.67% | 9.00% | 62.33% |
| 4 | 1 | 0 | 21 | 3 | 6 | 31 |
| 0.33% | 0.00% | 7.00% | 1.00% | 2.00% | 10.33% |
| 5 | 1 | 1 | 26 | 13 | 22 | 63 |
| 0.33% | 0.33% | 8.67% | 4.33% | 7.33% | 21.00% |
| Total | 10 | 7 | 192 | 31 | 60 | 300 |
| 3.33% | 2.33% | 64.00% | 10.33% | 20.00% | 100.00% |
Anterior loop of mental nerve was found to be present in 45.3% cases on the right side and in 55.3% cases on the left side, with a bilateral occurrence in 35 % cases.
Discussion
There has been a relentless battle with regards to the most common position of the mental foramen in view of its variations in different populations and ethical groups.
The results of this study, which reported the most common location of the foramen to be between the two premolars, showed similarity with the findings of recent studies done in the Central Asian population, hence giving confirmatory evidence of the presence of a racial predilection over the location of the foramen [22–25]. However, variances have also been published in the studies which were done over other populations which described the MF to be most frequently aligned with the second premolar [6–16].
A summary of the recent studies done on various racial and ethnic groups has been summarized in [Table/Fig-6].
Comparison showing the percentage position of the mental foramen in different populations and ethnic groups
| Sample size | Year | Distribution | Population | Reference | Technique | Journal |
|---|
| 1 | 2 | 3 | 4 | 5 |
|---|
| 169 | 2003 | 0 | 3.4 | 19.6 | 69.2 | 7.7 | Malay | Ngeow et al., | Pan.* | J. Oral Sci |
| 70 | 2005 | 0 | 2.8 | 10 | 62.9 | 24.3 | Malawian | Igbigbi et al., | DM† | West Afr J Med |
| 361 | 2006 | 1.2 | 3.2 | 71.5 | 22.4 | 1.33 | Turkish | Gungor et al., | Pan. | Coll. Antropol. |
| 72 | 2006 | - | - | 26.8 | 64.3 | - | Korean | Kim et al., | Pan. | Implant Dent |
| 100 | 2007 | - | - | - | 45 | 35 | Tanzania | Fabian et al., | DM | Ital J Anat Embryol. |
| 70 | 2008 | - | - | 30 | - | - | Turkish | Yesilurt et al., | | Folia Morphol |
| 400 | 2009 | 0 | 1.6 | 47.3 | 46 | 5.1 | Iranian | Haghanifar et al., | Pan. | Indian J Dent Res |
| 500 | 2011 | 40 | | 55 | | 33.2 | | Pria et al., | Pan. | J Contemp Dent Pract. |
| 500 | 2013 | - | 4.4 | 44.4 | 43.2 | 8 | Kosovarian | Kquiku et al., | Pan. | Coll. Antro. |
| 377 | 2013 | 0.4 | 1.32 | 30 | 62.8 | 5.3 | Moroccan | Chkoura et al., | Pan. | Imaging Sci Dent |
*Pan= Panoramic radiograph , †DM= Dry mandible
Measurements of the vertical distance, which were calculated by Sankar et al., which scaled to 16.5 mm and 14.3 mm respectively on the right and the left sides (giving an average distance of 15 mm) [22], matched the average value of 15.46mm, which was accounted for in the present study, which ascertained that the referencing from the lower border of the mandible remained undeviated, even with the relocation of the MF closer to the alveolar crest, which was attributed to the post extraction resorption of the alveolar bone [15].The bilaterally symmetrical occurrence of the mental foramen, which was commonly observed between both the premolars in this study, has obtained an assorted review of references [26–28].
Identification of presence of anterior loop is imperative for surgical interventions in the area, particularly for implant placements and hence a safety zone establishment has been reviewed in all surgical procedures as the surgical rationale of the mental foramen’s position, as well as, when the anterior loop is suspected of being present [29].
Conclusion
In conclusion, the most common location of the foramen for the south Asian population was found to be between the two premolars. However, inter and intraracial variations have been reported. Hence, comprehending the significance of being aware of possibility of anatomical variations of the foramen as well as determining its location during the pre-operative radiological examinations were included in planning of the following surgery. The findings of this study could aid as the most common orientation of the mental foramina in the Indian population and they could help in gauging a safety limit during surgical procedures.
*Pan= Panoramic radiograph , †DM= Dry mandible