Metastatic Primary Signet Ring Cell Carcinoma of Rectum: A Case Report of 10-Year-old Male Child
Kumkum Singh1, Amit Singh2, Shyam Bhutra3, Geeta Pachori4, Mahesh Kumar Jangir5
1Professor and Head, Department of Surgery,Jawahar Lal Nehru Medical College, Ajmer Rajasthan, India.
2Senior Resident, Department of Surgery,Jawahar Lal Nehru Medical College, Ajmer Rajasthan, India.
3Associate Professor, Department of Surgery,Jawahar Lal Nehru Medical College, Ajmer Rajasthan, India.
4Professor and Head, Department of pathology,Jawahar Lal Nehru Medical College, Ajmer Rajasthan, India.
5Postgraduate Student, Department of Surgery,Jawahar Lal Nehru Medical College, Ajmer Rajasthan, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amit Singh, Senior Resident, Department of Surgery, Jawahar Lal Nehru Medical College, Ajmer Rajasthan, India.
E-mail:dr.amit5280@gmail.com
Signet ring cell carcinomas of the colon and rectum are well documented in the adult population, but the incidence is very low in the paediatric population. Signet ring cell carcinoma has more malignant potential, mostly present as advanced stage and carries very poor prognosis. We are describing a 10-year-old male patient who presented with acute intestinal obstruction; radiology revealed large bowel obstruction and was diagnosed metastatic primary signet ring cell carcinoma of rectum on biopsy. We have discussed the diagnostic work-up and the management of this rare entity. Due to the high mortality that can be caused by a delay in making the correct diagnosis, signet ring cell carcinoma of colorectum represents a special diagnostic and surgical challenge.
Mucinous Tumor, Colorectal Neoplasm, Intestinal obstruction
Case Report
A 10-year-old boy presented in emergency department with chief complaints of abdominal distension and vomiting for two days. He had history of intermittent lower abdominal pain, and altered bowel habits since two months. There was no history of bleeding per rectum. Family history was not significant. General physical examination revealed a healthy appearing male child. The blood pressure was 100/80 mm of Hg, pulse rate 110/minute and respiratory rate 22/minute. On examination abdomen was grossly distended, bowel sounds were increased. Generalised tenderness, guarding and rigidity present.
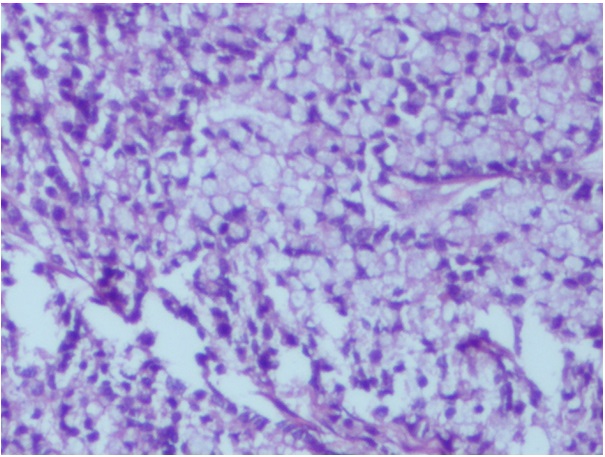
On digital rectal examination, a circumferential hard constricting growth was palpable about 5 cm from the anal verge. X- ray chest was within normal limit. X-ray abdomen was suggestive of large bowel obstruction. Routine investigations like Hb, serum Na+/K+, blood urea, liver function tests were within normal limits. With above findings, clinical diagnosis of acute intestinal obstruction due to rectal growth was made and laparotomy was planned. Laparotomy revealed gross distension of whole colon. Serosal surface showed multiple tiny nodules. A stricture was palpable in distal sigmoid colon and rest of Pelvis was frozen. Peritoneal seeding was noted and omentum was caked. Stomach, liver and spleen were normal. A diagnosis of non resectable advanced carcinoma rectum was made and considered for palliative surgery. Sigmoid colostomy with omental biopsy was done. omental biopsy shows features of metastatic deposit of adenocarcinoma having signet ring differentiation [Table/Fig-1]. The immediate postoperative course was uneventful and FOLFOX regimen (5 Fluoruracil, calcium folinate, oxaliplatin) was started. But unfortunately patient was lost to follow up after two cycles.
Photomicrograph showing tumour cell having intracytoplasmic mucin pushing the nucleus to the periphery and giving a signet ring appearance (H&Ex100)
Discussion
Signet ring cell carcinoma is a rare subtype of adenocarcinoma, where abundant intracytoplasmic mucin pushes the nucleus to the periphery giving a signet ring appearance. The carcinoma can occur in many different sites of the body but more than 96% of signet-ring cell carcinomas arise in the stomach. However, it can also originate from the colon, rectum, gallbladder, pancreas, urinary bladder, and breast. Primary Signet ring cell carcinoma of the colon and rectum was first described by Laufman and Saphir [1]. Primary Signet ring cell carcinoma of colon and rectum is a distinctive malignant disease and rarer than conventional adenocarcinoma, with a reported incidence ranging from 0.01% to 2.6% [2]. Primary signet ring cell carcinoma of colorectum is diagnosed when the following criteria are satisfied. Firstly tumor must be primary, histological material is adequate and signet ring cell present more than 50% of cancer [3]. All the three criteria were satisfied in our case. In our case clinical history and laparatomy ruled out primary growth in the stomach. Immunohistochemical staining profiles for MUC1, CDX2 and MUC2 have been used to characterize and differentiate SRCC of breast, stomach and colorectum [4].
Signet ring cell carcinoma of colorectum has an aggressive clinical course and poorer prognosis. There is high incidence of peritoneal metastases and relatively low incidence of hepatic metastases, a characteristic feature distinguishing colorectum signet ring cell carcinoma from non signet colorectum carcinoma [5].
In the literature, signet ring cell carcinomas tend to affect predominately adult individuals. Median age is about 59 years when compared to the non signet cell cancer, where the median age is about 61 years [6]. Our case is rare because of very young age of presentation of this cancer. The cases with colorectal signet ring cell carcinoma in young patients in the literature are shown in [Table/Fig-2].
The most common presenting symptom for the children with colorectal signet cell carcinoma is abdominal pain and vomiting. Other symptoms include rectal bleeding, mucus in stool, change on bowel habits and weight loss. These clinical symptoms resemble those of irritable bowel disease; hence the diagnosis of colorectal signet ring cell carcinoma in children is based on a high index of suspicion. Because of the lack of awareness at early age, vague symptoms and the aggressive characteristic of the tumour, signet ring cell carcinomas of the colon and rectum mostly present as advanced stage.
Colorectal malignancy can be confirmed by digital rectal examination (DRE), sigmoidoscopy or colonoscopy. Contrast studies, ultrasonography and computed tomography are essential procedures for detecting the extent of the disease. Surgery is the most effective treatment for colorectal cancer. It is to be stressed that the survival is dependent on the complete resection of the cancer and aggressive surgical procedures can increase the survival rates of these patients. In patients with resectable mass, complete tumor resection that includes the lymphatic basin of the affected colon and/or rectum has the greatest impact on the overall survival. The reported median survival time ranges from 15 to 32.6 months [12]. Although adjuvant chemo-radiotherapy has limited value of benefit in most of the cases, a variety of new agents such as irinotecan, oxaliplatin and leucovorin used in association with 5-FU should be considered.
Comparison of Colorectal signet ring cell carcinoma in young patients in the literature ND:Not determined
| Author’s | Age-Sex | Symptoms | Site of tumour and histology | Stage at presentation | Treatment | Survival |
| Ozgul et al., [7] | 19years, m | Persistant abdominal pain, weight loss | Sigmoid colon/signet ring cell carcinoma | Advanced | Palliative colostomy FOLFOX-6 +Bevacizumab | ND |
| Sun Hyung Kang et al., [8] | 21years, m | Hematochezia | Polyp at proximal rectum/signet ring cell carcinoma | Early | Local resection with end to end anastomosis | ND |
| Jagtap SV et al., [9] | 31years, m | Persistent abdominal pain, vomiting Subacute intestinal Obstruction | Rectsigmoid/signet ring cell carcinoma | Advanced | Radical resection with end to end anastomosis | ND |
| Pandey A et al., [10] | 10years, m
11years, m
11years, m
10years, m | All patients present with Bleeding per rectum, pain abdomen | Rectosigmoid/signet ring cell carcinoma | Advanced
Advanced
Advanced
Advanced | Transverse colostomy
Transverse colostomy
Refused treatment
Surgical resection | One year
11 month
ND
One year |
| Marone J et al., [11] | 17years, m | Progressive abdominal pain | Ascending colon/signet ring cell carcinoma | Advanced | Right colon rescection with iliocolic anastomosis | One year |
| Kumkum singh et al., (Present Study) | 10years, m | Abdominal pain & distension, vomiting | Rectosigmoid, Signet ring cell carcinoma | Advanced | Palliative Colostomy, FOLFOX | ND |
Conclusion
Colorectal malignancy in children are rare, hence any child presenting with pain in abdomen along with doubtful history of constipation and rectal bleeding should be evaluate properly. The present experience has shown that in the paediatric age group small bowel obstruction is common but once radiology shows large bowel obstruction, malignancy should be considered in differential diagnosis because early diagnosis and aggressive management lowers the morbidity and mortality in particular if it is a signet ring cell carcinoma of colon and rectum as in indexed case that carries extremely poor prognosis in advanced stage.
[1]. H Laufman, O Safir, Primary linitus plastica type of carcinoma of the colonAMA Arch Surg 1951 62:72-91. [Google Scholar]
[2]. T Anthony, R George, M Rodriguez-Bigas, NJ Petrelli, Primary signet-ring cell carcinoma of the colon and rectumAnn Surg Oncol 1996 3:344-48. [Google Scholar]
[3]. L Messerini, A Palomba, G Zampi, Primary signet-ring cell carcinoma of the colon and rectumDis Colon Rectum 1995 38:1189-92. [Google Scholar]
[4]. Chu Peiguo G, Weiss Lawrence M, Immunohistochemical characterization of signet-ring cell carcinomas of the stomach, breast, and colonAm J Clin Pathol 2004 121:884-92.DOI: 10.1309/A09ERYMFR64NERDW [Google Scholar]
[5]. HL Sim, KY Tan, PL Poon, A Cheng, Primary rectal signet-ring cell carcinoma with peritoneal dissemination and gastric secondariesWorld J Gastroenterol 2008 14(3):2118-20. [Google Scholar]
[6]. DE Henson, C Dittus, M Younes, H Nguyen, J Albores-Saavedra, Differential trends in the intestinal diffuse types of gastric carcinoma in the United States, 1973–2000: increase in the signet ring cell typeArchives of Pathology and Laboratory Medicine. 2004 128(7):765-70. [Google Scholar]
[7]. Pamukçu Ozgul, Selcukbiricik Fatih, Signet cell carcinoma of colon in a nineteen-year-old patient: A case report. Case Reports in Oncological Medicine. 2013, Article ID 695450http://dx.doi.org/10.1155/2013/695450 Accessed on 14 Aug 2013. [Google Scholar]
[8]. Kang Sun Hyung, Chung Woo Suk, A rare case of a signet ring cell carcinoma of the colon mimicking a juvenile polypGut and Liver 2012 6(1):129-31.PMCID: PMC3286732. [Google Scholar]
[9]. SV Jagtap, DB Nikumbh, AY Khirsagar, SS Jagtap, Shamima Primary signet-ring carcinoma (linitus plastica) of the colorectum presenting as subacute intestinal obstructionOnline J Health Allied Scs 2012 11(1):14 [Google Scholar]
[10]. A Pandey, Gangopadhyay AN, Sharma SP, Kumar V, Gupta DK, Gopal SC, et al. Paediatric carcinoma of rectum Varanasi experienceIndian Journal of Cancer. 2008 [Google Scholar]
[11]. J Marone, S Patel, M Page, P Cheriyath, Signet cell carcinoma of the colon in a 17 Year old childJSCR 2012 9(3) [Google Scholar]
[12]. W Song, SJ Wu, YL He, SR Cai, CH Zhang, XH Zhang, Clinicopathologic features and survival of patients with colorectal mucinous, signet-ring cell or nonmucinous adenocarcinoma: experien at an institution in southern ChinaChin Med J (Engl) 2009 122(13):1486-91.PubMed PMID: 19719934. [Google Scholar]