Splenic Epidermoid Cyst - A Rare Entity
Amrit Pal Singh Rana1, Manjit Kaur2, Parvinder Singh3, Satish Malhotra4, Amarjit Singh Kuka5
1Assistant Professor, Department of Surgery,Guru Gobind Singh Medical College, Faridkot, India.
2Assistant Professor, Department of Pathology,Guru Gobind Singh Medical College, Faridkot, India.
3Assistant Professor, Department of Surgery,Guru Gobind Singh Medical College, Faridkot, India.
4Assistant Professor, Department of Surgery,Guru Gobind Singh Medical College, Faridkot, India.
5Assistant Professor, Department of Surgery,Guru Gobind Singh Medical College, Faridkot, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amrit Pal Singh Rana, 218, Medical Campus, Faridkot-151203, India.
Phone: 9464794566,
E-mail:dramritpalsingh@gmail.com
C Splenic epidermoid cysts are relatively uncommon. Most often, they are asymptomatic, but they may present with abdominal discomfort, predominantly at young ages. We are reporting a rare case of 12-years-old female child with history of dull intermittent pain, tender palpable mass in left hypochondrium on physical examination. Ultrasonography (USG) of abdomen showed large cyst in upper pole of spleen, and an X ray of chest revealed slightly raised left hemidiaphragm. Axial sections taken on computerized tomography of abdomen showed a large well defined cystic mass near upper pole of spleen, with a thin septum in it. On laparotomy, open total splenectomy was performed. Sections from cystic wall were processed and histopathological examination revealed fibrous tissue covered by stratified squamous epithelium. Although, now-a-days emphasis is being laid on minimal invasive operative procedures which preserve spleen. This case report favours total splenectomy, considering postoperative outcome. The final diagnosis always depends upon histopathological examination.
Spleen, True splenic cyst, Total splenectomy
Introduction
Splenic cysts are rare. They may be congenital, neoplastic, vascular, inflammatory and posttraumatic in origin and may contribute to 30-40% of the total splenic lesions [1]. Congenital splenic cysts are usually asymptomatic and they are rarely seen in the routine surgical practice. Also, due to lack of typical clinical presentation, they are discovered incidentally. Splenic epidermoid (congenital) cysts constitute approximately 10% of total cysts and they are encountered more commonly in children and young adults. Their prognosis is good. The traditional treatment of splenic cysts had been splenectomy, but during the past decade, it was observed that splenectomy led to short and long-term complications. Presently, the emphasis is being laid on conservation of spleen, especially in children and young adults, in order to avoid overwhelming postsplenectomy infections [2]. However, not all splenic cysts can be treated by partial splenectomy [3].
We are reporting a case of a large splenic epidermoid cyst- a rare type of splenic cyst, which was removed by open total splenectomy.
Case Report
A 12-year-old female child presented with chief complaints of dull pain, discomfort and feeling of fullness in left upper abdomen, which had been present since past three years. Pain was intermittent in nature, which had increased in intensity since past 15 days. There was no history of fever, trauma and there was no association with food intake. On physical examination, a firm, smooth, slightly tender mass was seen in left hypochondrium, which was palpable.
USG of abdomen was done and it showed enlarged spleen with well defined cystic mass, which measured 8.5x8.2 cm in size, with internal echoes in upper pole of spleen, in subdiaphragmatic location. X-ray of chest revealed slightly raised left hemidiaphragm.
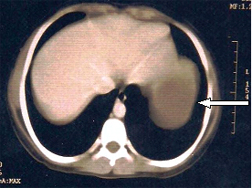
CT of abdomen was conducted on a helical scanner, after administering oral and intravenous contrast. Axial sections showed a large well defined cystic mass which was 10.2x8.4 cm in size, at upper pole of spleen [Table/Fig-1], with a thin septum in it.
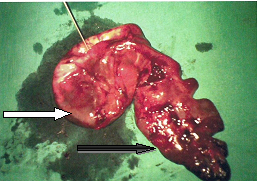
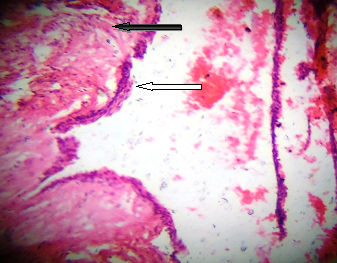
Elective laparotomy was performed and a large splenic cyst was found, which was located at the upper pole of spleen. Reduction in size of cyst was done by intraoperative aspiration of about 600 ml of turbid coloured fluid. Due to location and size of cyst, preservation of the spleen was considered as impossible and splenectomy was done. Grossly, large sized cystic lesion which was approximately 10.0 cms of maximal diameter was discovered, with almost total replacement of splenic tissue at one side [Table/Fig-2]. Histopathological examination revealed that the whole cyst wall which was constituted by stratified squamous epithelium underneath the epithelium was fibrous tissue [Table/Fig-3]. The diagnosis of splenic epidermoid cyst was confirmed. The post-operative clinical course of the patient was satisfactory and uneventful.
CT (abdomen) demonstrating a large cystic mass (white arrow head) of splenic origin.
Gross photograph depicting a larger cyst (white arrow head) and part of normal spleen at one side (black arrow head).
Showing dense fibrous tissue (black arrow head) underneath the stratified squamous epithelium (white arrow head). H&E(40x)
Results
Patients with splenic cysts are usually asymptomatic, who present occasionally with vague symptomatic presentations. Discovery of cystic lesions of spleen is an easy task which can be achieved by doing imaging studies, but determination of true nature and pathology of the cyst is not possible all the times preoperatively. Although, now-a -days emphasis is being laid on spleen preserving surgeries, it has been observed that conservative treatment is not possible in the cases where cysts are of large sizes and where the chances of surgical complications are higher than the rare risk of overwhelming post-splenectomy sepsis. The ultimate diagnosis, however, depends upon histopathological findings .
Discussion
Splenic cystic lesions are rare, uncommonly encountered in routine surgical practice. Robbins reported a series of 42,327 autopsies over a 25-year period and results showed that only 32 patients had the diagnosis of splenic cyst [4].The classification, diagnostic modalities and treatment guidelines for splenic cysts are far from being uniform or clear. Three classifications have been found in literature (Fowler’s, Martin’s and Morgenstern’s classifications). Martin et al., had classified splenic cysts as Type I cysts which were primary (true) cysts with cellular linings of parasitic or non parasitic origin. Nonparasitic type I splenic cysts have been further divided into congenital and neoplastic cysts. Congenital cysts include epidermoid, dermoid and endodermoid cysts, whereas neoplastic cysts constitute hemangiomas, lymphangiomas. Of these, hemangiomas are the most common ones and dermoid cysts are the least common ones. Type II cysts are false (secondary) cysts without cellular linings [5]. Differential diagnoses include intrasplenic abscesses, hydatid cysts, true cystic neoplasms (hemangiomas, lymphangiomas, epidermoid and dermoid cysts) and cystic metastases. Epidermoid cysts are the rarest among all true cysts which occur in spleen [2].
Primary (true) cysts make up approximately 20% of all types of cysts which occur in spleen. Epidermoid cysts are the rarest, which comprise only 10% of benign, nonparasitic cysts which occur in the spleen. Splenic epidermoid cysts are “true” cysts, as they possess inner epithelial linings of stratified squamous epithelium, whereas “false” cysts have no cellular linings, and are usually related to prior trauma, haemorrhage or infarction [4]. The origin of true cysts is still not very clear, but they are thought to develop from mesonephric tissue in the developing spleen in early embryonic life. The mechanism which has been suggested is infolding or entrapment of peritoneal mesothelial cells in the splenic parenchyma during embryogenesis in the intrauterine life. The age at presentation ranges from newborns to 50 years, with average age of around 17 years. There is slight female preponderance [6]. Majority of the cases (approximately 80%) present with solitary and unilocular cysts.
True cysts and false cysts are usually indistinguishable on imaging studies; false cysts tend to have thicker fibrous walls and eggshell like calcifications, along with internal debris. On USG, epidermoid cysts are recognized as well-defined, thin walled, anechoic cystic lesions. There can be increased ecogenecity caused by intracystic haemorrhage and cholesterol crystals and inflammatory necrotic debris which are same as those which are seen in false cysts. Although peripheral calcifications occur more frequently in posttraumatic or false cysts, in epidermoid cysts with occasional internal septations, cystic walls may show curvilinear or plaque like calcifications. In addition, computerized tomography may give clearer picture regarding intracystic fluid, internal septations or calcifications. Although partial splenectomy offers a definite solution in case of splenic cysts (<5 cm), conservative treatment like aspiration alone, incision and drainage can also be considered [7-8]. But total splenectomy is the treatment of choice in case of larger cysts (>5cm), as it prevents serious complications like rupture, haemorrhage, infection and sometimes, the recurrence which is attributed to coexistence of invisible tiny cysts that had remained in the splenic tissue after the dissection of the major cyst. In the cases where hilum is involved, splenectomy remains a relatively safe procedure [3-7].
Finally, radiologically distinguishing between true and false splenic cysts does not seem to be possible preoperatively and the final diagnosis relies on histopathological examinations of wall of the cyst. However, total splenectomy (open or laparoscopic) is primarily recommended for the prevention of complications which are seen as infections, haemorrhage and rupture.
[1]. M Urrutia, PJ Mergo, LH Ros, Cystic masses of spleen; Radiologic pathologic correlationRadiographics 1996 16(1):107-29. [Google Scholar]
[2]. ZO Marjanovic, IM Djordjevic, Epidermoid splenic cysts in children and adolescentsActa Chir Iugosl 2008 51(1):63-67. [Google Scholar]
[3]. K Kalinova, Giant pseudocyst of the spleen: A case report and review of the literatureJournal of Indian Association of Pediatric Surgeons 2005 10(3):176-78. [Google Scholar]
[4]. FG Robbins, AE Yellin, RW Lingua, JR Crsig, FL Turrill, WP Mikkelsen, Splenic epidermoid cystsAnn Surg 1978 187(3):231-35. [Google Scholar]
[5]. JW Martin, Congenital splenic cystsAm J Surg 1958 96:302-08. [Google Scholar]
[6]. MB Hansen, AC Moller, Cysts Splenic, Surg Laparosc Endosc Percutan Tech 2004 Dec 14(6):316-22. [Google Scholar]
[7]. AK Elias, R Evangelos, C Evangelos, Surgical management of nonparasitic splenic cystsJSLS 2009 13(2):207-12. [Google Scholar]
[8]. O Boybeyi, I Karnak, FC Tanyel, AO Çiftçi, ME Enocak, The management of primary nonparasitic splenic cystTurk J Pediatr 2010 52:500-04. [Google Scholar]