Neuroendocrine Carcinoma of the Stomach-A Case Report
Poorana Priya P1, Hemalatha Ganapathy2, Subhash A.R3
1Post Graduate, Department of Pathology,Sree Balaji Medical College and Hospital, Bharath University, Chrompet, Chennai, India.
2Professor, Department of Pathology,Sree Balaji Medical College and Hospital, Bharath University, Chrompet, Chennai, India.
3Professor, Department of Pathology,Sree Balaji Medical College and Hospital, Bharath University, Chrompet, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Poorana Priya P., Sree Balaji Medical College, No.7, Works Road, New Colony, Chrompet, Chennai-600 044, India.
Phone: 8148486849,
E-mail: poorna.priya86@gmail.com
Neuroendocrine carcinomas of stomach have been considered a rare neoplasm. The present case concerns with a 69 year old male, who presented with vague abdominal discomfort and history of malena. Upper alimentary tract endoscopy showed an ulcero-proliferative growth in the antrum. Computed tomography abdomen revealed thickening of the gastric antrum, a subtotal gastrectomy was performed after correction of anemia. Microscopic evaluation revealed a neuroendocrine neoplasm. Immunohistochemically positive for Chromogranin A and Synaptophysin.A diagnosis of Neuroendocrine carcinoma of the stomach was given based on recent WHO classification of Neuroendocrine carcinoma of the stomach and on mitotic index with reference to grading scale.
Stomach, Neuroendocrine carcinoma, Chromogranin A, Synaptophysin, Mitotic figures
Case Report
A 69-year-old male, who presented with complaints of vague abdominal discomfort since two months and with history of malena since one month .The patient is a known case of diabetic and hypertensive, post CABG on regular medication .On physical examination pallor and bilateral minimal pitting pedal edema were seen. Abdomen was soft with epigastric tenderness. There were no organomegaly or free fluid , bowel sounds heard, hernial orifices and renal angle were free and external genitalia appeared normal. Per rectum examination showed normal spinchter tone, and the glove stained black. His haemoglobin was about 5.2g/dl and PCV of 17%, stool for occult blood was positive. Peripheral smear examination showed microcytic hypochromic picture. His renal and liver function tests were normal.
Chest X-ray, Echocardiography and ultrasound examination of abdomen were normal. Upper Alimentary tract endoscopy, showed an ulceroproliferative growth in the antrum.
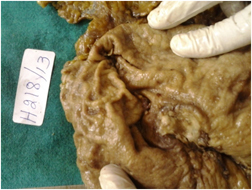
Computed tomography abdomen revealed thickening of the gastric antrum. Clinically diagnosed as carcinoma of the stomach with features of anemia. After the correction of anemia the patient underwent subtotal gastrectomy with Roux-en-Y Gastro jejunostomy and jejuno- jejunostomy with 5cm clearance proximally. The resected specimen was sent to the Department of Histopathology. On Gross examination, the Subtotal gastrectomy specimen measured 12x8x4 cm. On the cut section an ulcer was identified measuring 3x2 cm along the lesser curvature of the stomach with everted edges and necrotic base [Table/Fig-1].
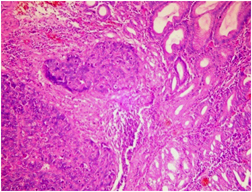
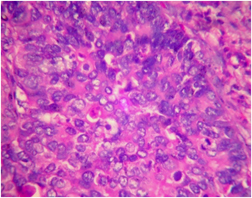
Microscopic evaluation showed a neoplasm in the submucosa [Table/Fig-2] composed of round to oval cells, with vesicular nucleus and dispersed chromatin [Table/Fig-3], with tumor exhibiting microglandular, nesting and trabecular pattern. Some of the cells show hyperchromatic and pleomorphic nuclei with More than 5 mitotic figures per high power field [Table/Fig-3] along with areas of necrosis and infiltration of the tumor up to the serosa. Resected margins, rest of the gastric mucosa and omental fat appeared normal.
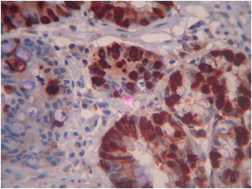
Immunohistochemically, the tumor cells were positive for Chromogranin A [Table/Fig-4] and Synaptophysin [Table/Fig-5]. Based on histological tumor patterns, positivity for neuroendocrine markers and mitotic counts a diagnosis of Neuroendocrine carcinoma of stomach –Grade 3 was made.
The post-operative period was uneventful. He was discharged on 13th post-operative day and followed up on an outpatient basis. He has now completed his 4th cycle of chemotherapy and he is doing well.
Gross specimen showing ulcerative lesion of size 3x2cm along the lesser curvature of the stomach with everted edges and necrotic base.
Tumor Island involving the submucosa(hematoxylin and eosin,x10)
Tumor cells showing pleomorphism ,vesicular nuclei, dispersed chromatin and more than More than 5 mitotic figures per high power field.(hematoxylin and eosin X 40)
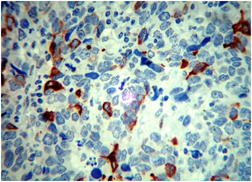
Chromogranin A positivity of the tumor cells.(IHC,X40)
Synaptophysin positivity of the tumor cells (IHC X 40)
Discussion
Neuroendocrine carcinoma of stomach is a rare neoplasm known for its aggressive behaviour and poor prognosis [1]. Neuroendocrine carcinoma accounts for less than 1% of all gastric tumors[2] . To the best of our knowledge only few cases of neuroendocrine carcinoma of the stomach have been reported in India. It occurs mostly in adults and rare in children and has prelidiction for females [3].
Siegfried oberndorfer coined the term carcinoid and found the malignant intensity of the carcinoid [4]. Langhans in 1867 described the carcinoid tumor [5]. Enterochromaffin cells are located along the lower third of the gastric mucosa adjacent to the chief cells. Proliferation of these enterochromaffin cells results in hyperplasia, Dysplasia and neoplasia [6].
Recently WHO classifies the gastric neuroendocrine carcinoma in to well differentiated neuroendocrine tumor, well differentiated carcinoma and poorly differentiated carcinoma based on the biological behavior, tumor size, tumor infiltration and angioinvasion [7].
The proliferative rate of the tumor is assessed based on number of mitoses per 10 high per field or the percentage of neoplastic cells immunolabelleling for KI-67, a proliferative marker [7].
Ultrasound and computed tomography of abdomen are helpful in locating and staging the lesion. But a definitive diagnosis can be made only on the basis of histopathological findings along with neuroendocrine markers. Therefore in the present case the diagnosis of Neuroendocrine carcinoma of the stomach was arrived based on the histological criteria like tumor patterns, dispersed chromatin with typical “salt and pepper” appearance, serosal infiltration of the tumor, areas of necrosis and more than 20 mitotic figures per 10 high per field. Hence we classified and graded our case as neuroendocrine carcinoma of the stomach Grade- 3,according to the recent WHO criteria of classification and the grading scale for mitotic counts [7].
Our case revealed immunohistochemically positive for Chromogranin A and Synaptophysin. which further supported in arriving the diagnosis.
Conclusion
In conclusion, Neuroendocrine carcinoma is a rare neoplasm arising in the stomach. Histological findings and Neuroendocrine markers like Chromogranin A and Synaptophysin plays a significant role in confirming the diagnosis. A complete surgical resection followed by chemotherapy is curative in most cases. Follow-up is necessary for assessing lymphatic invasion of the tumor and for prognostic significance.
[1]. N Chiba, T Suwa, M Hori, M Sakuma, M Kitajima, Advanced gastric endocrine cell carcinona with distant lymph node metastasis: a case report and clinicopathological characteristics of the diseaseGastric Cancer 2004 7(2):122-27. [Google Scholar]
[2]. IM Modlin, KD Lye, M Kidd, Carcinoid tumors of the stomachSurgical Oncology. 2003 12(2):153-72. [Google Scholar]
[3]. C Bordi, JY Yu, MT Baggi, Gastric carcinoids and their precursor lesions. A histologic and immunohistochemical study of 23 casesCancer 1991 67:663-72. [Google Scholar]
[4]. Tsoucalas Gregory, Karamanou Marianna, Androutsos George, Medical School, University of Athens, GreeceAnn Gastroenterol 2011 24(2):98-100. [Google Scholar]
[5]. T Langhans, Ueber einen Drusenpoly im IleumVirchows Arch 1887 38:559-60. [Google Scholar]
[6]. Bordi C, T D’Adda, Azzoni C, G Ferraro, Pathogenesis of ECL cell tumors in humansYale J Biol Med 1998 71(3-4):273-84. [Google Scholar]
[7]. S Klimstra, David, Modlin R Irvin, Coppola Domenico NANETS Guidelines The pathologic classification of Neuroendocrine Tumors: A review of nomenclature, Grading and Staging SystemsPancreas 2010 39(6):707-12. [Google Scholar]