Encysted Spermatic Cord Hydrocele in a 60-year-old, Mimicking Incarcerated Inguinal Hernia: A Case Report
Manimaran D1, Karthikeyan T M2, Dost Mohamed Khan3
1Associate Professor, Department of Pathology,Shri Sathya Sai Medical College and Research Institute, Tiruporur, Tamilnadu, India.
2Associate Professor, Department of Pathology,Melmaruvathur Adhiparasakthi Institute of Medical Science and Research, Melmaruvathur, Tamilnadu, India.
3Associate Professor, Department of Pathology,Shri Sathya Sai Medical College and Research Institute, Tiruporur, Tamilnadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Manimaran D., New No. 5, LIC Colony, Main Road, Velachery, Chennai, Tamilnadu-600042, India.
Phone: 9841310232, manimaran.anu@gmail.com
Hydrocele of spermatic cord is caused by defect in closure of the processus vaginalis, as the testicles descend into the scrotum during foetal development. It usually occurs in infancy and childhood. There are two types of hydrocele of spermatic cord. Encysted type is caused by defective closure at both proximal and distal ends of processus vaginalis and it does not communicate with the peritoneal cavity. Funicular type is caused by defective closure of only distal end of tunica vaginalis and it communicates with the peritoneal cavity. The encysted type can be confused clinically with incarcerated inguinal hernia, inguinal lymphadenopathy, undescended testis and primary tumours of cord like lipoma. We are presenting a case of encysted hydrocele of spermatic cord in a 60-year-old male, which clinically mimicked incarcerated inguinal hernia.
Encysted spermatic cord hydrocele, Cord hydrocele, Hydrocele
Case Report
A 60-year-old male presented with swelling in the left inguinal region, which progressively increased in size within three years. He complained of intermittent dull aching pain for 3 days duration. History of constipation was present. There was no history of abdominal pain, vomiting and fever. On examination, a well circumscribed lesion which measured 4 cm in diameter was seen in the middle of inguinal canal, which was tense, cystic and nontender on palpation. Transillumination test and cough impulse test showed negative results. The lesion was felt as separate mass from the testicle. Ultrasonogram showed turbid cystic focus in the left inguinal region And the left testis measured 2.4 x 1.5 cm, which showed heterogeneous echo pattern with varices. Right testis was normal. Clinical differential diagnosis were incarcerated inguinal hernia and encysted hydrocele of the cord. Intra-operatively, a cystic structure which was attached to spermatic cord was found. Cyst was opened and 100 ml of straw coloured fluid was let out. Left testis was found to be small and atropic. Left high orchidectomy was done, along with resection of the cyst.
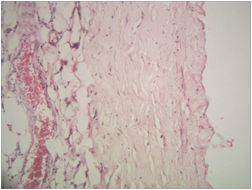
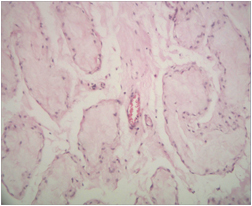
Grossly, the specimen consisted of testis which measured 2.5 x 1.5 cm, along with spermatic cord which was 13 cm in length. Cut surface showed a cyst with smooth inner surface, which measured 4 cm in diameter, in the middle of the spermatic cord [Table/Fig-1]. Microscopy of the cyst wall showed thick fibrotic wall which was lined by flattened mesothelial cells, along with congested blood vessels and lobules of adipocytes [Table/Fig-2]. Testis showed hyalinization of seminiferous tubules [Table/Fig-3].
Cut open cyst with smooth inner surface measuring 4 cm in diameter was seen in the middle of the spermatic cord with testis in the lower end.

Section of cord hydrocele show fibrous wall with congested blood vessels and flattened mesothelial lining on the right side (H&E stain , x100)
Section from testis show atrophic seminiferous tubules.(H&E stain, x100)
Discussion
Embryologically, as the testis descends from its retroperitoneal position into its final destination in the scrotum between 28 and 32 weeks of gestation, it carries with it two layers of peritoneum, which are called the processus vaginalis. It normally closes proximally at the level of the internal inguinal ring, distally above the epididymis and the segment which is present in between, undergoes involution [1]. The distal end around the testis becomes tunica vaginalis. When there is a defect in the closure of both proximal and distal points, a communicating hydrocele or a congenital inguinoscrotal hernia results and if only the distal point closes, then a funicular type hydrocele results. If the intervening segment between proximal and distal points fails to undergo involution, then an encysted hydrocele results [2]. Some patients have both the features and they are called mixed variety [3]. Conditions that may cause non-closure of the processes vaginalis, which lead to spermatic cord hydrocele, include: prematurity, cystic fibrosis, Ehlers-Danlos syndrome, hip dysplasia, peritoneal dialysis or ventriculo-peritoneal shunt [4]. An equivalent lesion in females is called a hydrocele of the canal of Nuck, which is the portion of the processes vaginalis within the inguinal canal in women [5].
A spermatic cord hydrocele produces a mass in the inguinal region, that may be difficult to differentiate from other lesions in the groin, like an incarcerated inguinal hernia, a paratesticular mass ( cyst or tumour), an inguinal lymphadenopathy or an ectopic testis [6]. Ultrasonogram can be used for differentiating this cystic lesion from other lesions in the inguinal region [7]. In our case, ultrasonogram was helpful for considering encysted spermatic cord hydrocele in the differential diagnosis. In ultrasonograms, it will be seen as avascular cystic lesion which is superior to and away from the testicle [8]. Computerized Tomography (CT) and magnetic resonance imaging (MRI) are also helpful for making the diagnosis of the lesion [2].
In a study which was done on three cases by Busigo J P et al., [2], two cases (65 and 69-year-old male) presented with cystic lesions in right inguinal region and one case (56-year-old male) presented with bilateral cystic lesion in the groin. All three cases had no complaints of pain, all had past histories of treatment for malignancies and all had been clinically suspected to have secondary deposits in the lymph nodes. In case report of Wani I et al., [6], a 36-year-old male had presented with swelling and severe progressive pain in the right inguinal region, with low grade fever of 12 days duration. Clinically, the lesion was soft, tender and it was misdiagnosed as irreducible inguinal hernia. Our case presented with cystic lesion in the middle of spermatic cord, on the left groin in a 60-year-old male, with complaint of intermittent dull aching pain, which mimicked incarcerated inguinal hernia. The lesion was felt as independent mass from the testicle. When there is a cystic lesion in the inguinal canal, the possibility of encysted hydrocele of the spermatic cord should be considered in the differential diagnosis, even though it is rare in adults. Clinically, it should be differentiated from incarcerated inguinal hernia, inguinal lymphadenopathy, undescended testis and spermatic cord tumours like lipoma, which will help in avoiding unnecessary invasive procedures.
[1]. V Garriga, A Serrano, A Marin, S Medrano, N Roson, X Pruna, US of the tunica vaginalis testis: anatomic relationships and pathologic conditionsRadio Graphics 2009 29:2017-32. [Google Scholar]
[2]. JP Busigo, F Eftekhari, Encysted spermatic cord hydroceles: A report of three cases in adults and a review of the literatureActa Radiol 2007 (48):1138-42. [Google Scholar]
[3]. YT Chang, JY Lee, JY Wang, CS Chiou, CC Chang, Hydrocele of the spermatic cord in infants and children: its particular characteristicsUrology 2010 76(1):82-6. [Google Scholar]
[4]. V Rathaus, O Konen, M Shapiro, L Lazar, M Grunebaum, M Werner, Ultrasound features of spermatic cord hydrocele in childrenBr J Radiol 2001 74(885):818-20. [Google Scholar]
[5]. A Caviezel, X Montet, J Schwartz, JF Egger, CE Iselin, Female hydrocele: the cyst of nuckUrol Int 2009 82(2):242-5. [Google Scholar]
[6]. I Wani, M Rather, G Naikoo, I Gul, Z Bhat, A Baba, Encysted hydrocele of cord in an adult misdiagnosed as irreducible hernia: a case reportOman Med J 2009 24(3):218-9. [Google Scholar]
[7]. LC Martin, JC Share, C Peters, A Atala, Hydrocele of the spermatic cord: embryology and ultrasonographic appearancePediatr Radiol 1996 26(8):528-30. [Google Scholar]
[8]. LS Palmer, Hernias and hydrocelesPediatr Rev 2013 34(10):457-64. [Google Scholar]