Small Cell Neuroendocrine Carcinoma of the Cervix: A Rare Entity
Pavithra V1, C.N. Sai Shalini2, Shanmuga Priya3, Usha Rani4, S Rajendiran5, Leena Dennis Joseph6
1Assistant Professor, Department of Pathology,Sri Ramachandra Medical College and Research Institute, Chennai, India.
2Assistant Professor, Department of Pathology,Sri Ramachandra Medical College and Research Institute, Chennai, India.
3Assistant Professor, Department of Pathology,Sri Ramachandra Medical College and Research Institute, Chennai, India.
4Professor, Department of Obstetrics and Gynaecology,Sri Ramachandra Medical College and Research Institute, Chennai, India.
5Professor, Department of Pathology,Sri Ramachandra Medical College and Research Institute, Chennai, India.
6Professor, Department of Pathology,Sri Ramachandra Medical College and Research Institute, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Pavithra V., No. 895, 69th Street,11th Sector, K.K. Nagar, Chennai-600078, India.
Phone: 9840379393,
E-mail: pavith81@yahoo.co.in
Small cell carcinoma of the cervix is a rare and a very aggressive tumour. Once being considered to be a rare type of squamous cell carcinoma, evidence has proven that most of the tumours express one or more markers of neuroendocrine differentiation. The behaviour of this rare malignancy is different from that of squamous cell carcinomas, with a high propensity for nodal and distant metastases. Hence, there is a need to highlight this histopathological entity.
Small cell, Neuroendocrine, Cervix
Case Report
A 40-year-old woman presented to the Gynaecology Out Patients Department with intermittent lower abdominal pain which was there since past six months. The pain was dragging in nature and it increased over the past two weeks. Her past history and family history were uneventful. On examination, her general condition and laboratory investigations were found to be within normal limits. Per vaginal examination revealed a bulky cervix.
Histopathology
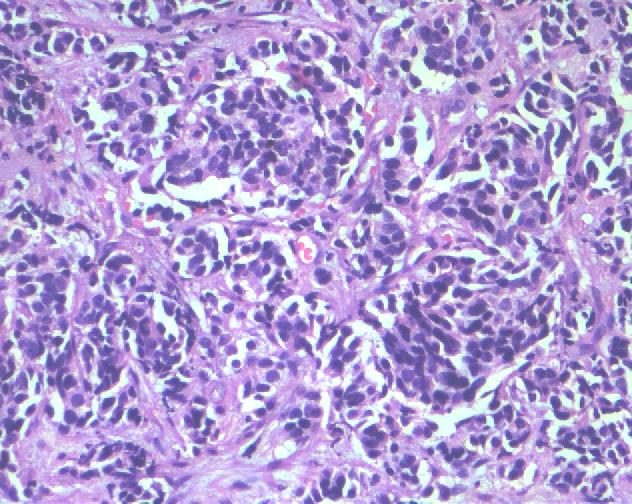
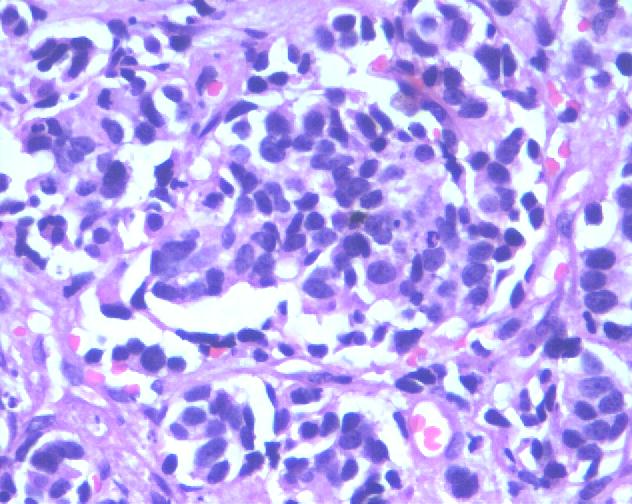
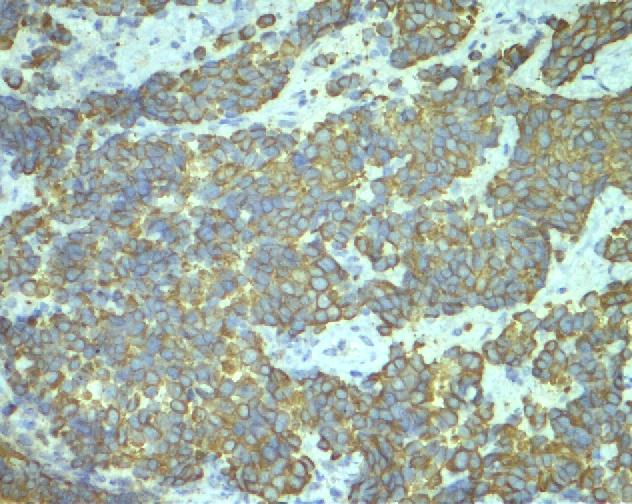
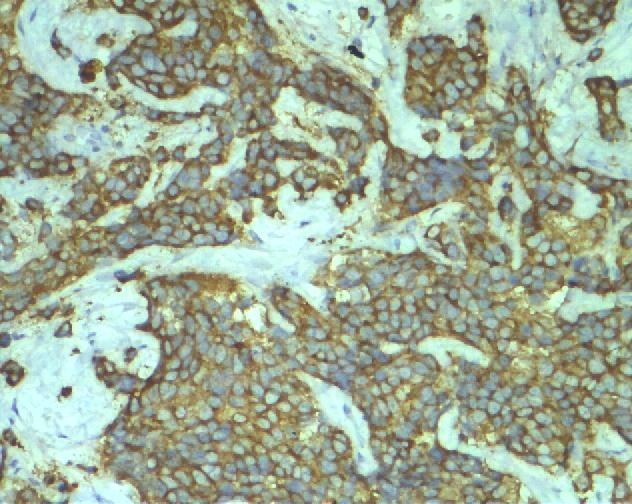
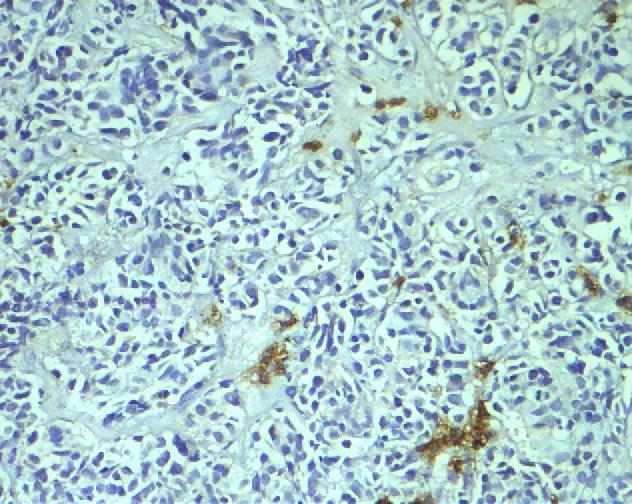
A cervical biopsy was submitted for histopathological examination. On light microscopy, the cervical tissue showed dense infiltration of monotonous round atypical cells, some of which were arranged in a nesting pattern and focally in sheets [Table/Fig-1]. The nuclei of most of the cells showed a salt and pepper chromatin with inconspicuous nucleoli [Table/Fig-2]. On immunohistochemistry, the tumour cells showed positivity for cytokeratin [Table/Fig-3] and synaptophysin [Table/Fig-4] and negativity for chromogranin and CD45 [Table/Fig-5]. The histopathological appearance and immunohistochemical findings led to the diagnosis of small cell carcinoma of the cervix and the patient was referred to the oncologist for further management.
Cervix – Small round blue cells (H&E 200x)
Cervix –Small round blue cells (H&E 400x)
Cervix-Cytokeratin positivity (IHC 200x)
Cervix-Synaptophysin positivity (IHC 200x)
Cervix – CD 45 negativity (IHC 200x)
Discussion
Neuroendocrine cells have been identified within normal epithelium throughout the female genital tract [1]. Neuroendocrine tumours of the female genital tract, probably originating from these cells, present as uterine small cell carcinomas or ovarian carcinoids. Small cell neuroendocrine carcinomas occur rarely in the cervix, vulva and vagina [2].
Small cell carcinoma of the cervix was once considered to be a rare, highly aggressive subtype of squamous cell carcinoma, but evidence has accumulated that most of the tumours express one or more markers of neuroendocrine differentiation. Hence, they have been placed under a separate entity of small cell neuroendocrine carcinoma of the cevix [2].
Review of literature has reported 280 cases of cervical small cell carcinomas, with the mean age of presentation being around the fifth decade, usually with bleeding and an obvious mass in most of the cases.
A clinical evidence of hormone production with or without a biochemical evidence has included cases of Cushing’s syndrome, Carcinoid syndrome, SIADH, and hypoglycaemia.
Histopathologically, the tumours are recognized by their microscopic resemblance to pulmonary small cell carcinomas (oat cell or intermediate types). On immunohistochemistry, these tumours have been found to be immunoreactive for cytokeratin, epithelial membrane antigen, carcino embryonic antigen, NSE, Leu 7, synaptophysin, chromogranin and a variety of peptide amine hormones. Electron microscopy may demonstrate dense core granules in most of the cases.
Multiple studies have demonstrated the presence of Human Papilloma Virus type 18 DNA or messenger RNA in almost two thirds of cases and perhaps more often in tumours in which a neuroendocrine differentiation has been shown [3,4].
Patients with small cell neuroendocrine cervical cancer have a poor prognosis and a predilection for nodal and distal metastases is very high. Common sites of metastasis included the lung, liver and bone. 75% of the patients have been in clinical stages I or II at the time of diagnosis. But in many low stage cases, metastases were found in lymph node samplings[5]. Mc Cusker et al., has found that at all stages of disease, survival was worse for women with endocrine tumours as compared to women with squamous cell carcinomas [6]. The disease free survival period is usually short, with most of the recurrences occurring within the first year.
Vishwanathan et al., analyzed the sites of relapse and overall survival in women with neuroendocrine marker positive small cell carcinomas of the cervix. They also concluded that patients with small cell neuroendocrine carcinomas of the cervix had a poorer prognosis. Their course is frequently characterized by the development of wide spread haematogenous metastasis [7].
The cervical biopsy of our case, on H and E staining, showed a histological resemblance to pulmonary oat cell carcinoma and the overlying squamous epithelium appeared unremarkable. So, our differential diagnosis included small cell variant of squamous cell carcinoma, small cell neuroendocrine carcinoma and Non–Hodgkin’s Lymphoma. Immunohistochemically, the tumour cells were strongly positive for synaptophysin and cytokeratin. The cells were negative for chromogranin and CD45. Small cell variant of squamous cell carcinoma may show complete negativity for neuroendocrine markers [3] while small cell neuroendocrine carcinoma may show variable positivity for cytokeratin [2]. Hence, a final diagnosis of small cell neuroendocrine carcinoma was made. The lymph node status at the time of diagnosis was not known and the patient was lost to further follow up due to financial and economic reasons.
Conclusion
This case has been highlighted for us to be familiarized with the histopathological differentials of small cell tumours of the cervix and to stress on the poor prognosis and aggressive nature of the tumour.
[1]. F Fetissof, MP Dubois, PU Heitz, Endocrine cells in the female genital tractInternational Journal of Gynaecological Pathology 1986 5:75-87. [Google Scholar]
[2]. Eichhorn John H, Young Robert H, Neuroendocrine tumors of the genital tract pathology and patterns review. AmericanJournal of Clinical Pathology 2001 115:94-112. [Google Scholar]
[3]. RA Ambros, J Park, ShahK Evaluation of histologic, morphometric, and immunohistochemical criteria in the differential diagnosis of small cell carcinoma of the cervix with particular reference to human papilloma virus types 16 and 18Modern Pathology 1991 4:586-93. [Google Scholar]
[4]. MH Stoler, SE Mills, DJ Gersell, Small cell neuroendocrine carcinoma of the cervix: a human papillomavirus type 18-associated cancerAm J Surg Pathol 1991 15:28-32. [Google Scholar]
[5]. EE Sheets, ML Berman, CK Hrountas, Surgically treated early-stage neuroendocrine small-cell cervical carcinomaObstet and Gynecol 1988 71:10-14. [Google Scholar]
[6]. ME McCusker, TR Cote, LX Clegg, FJ Tavassoli, Endocrine tumours of the uterine cervix: incidence, demographics, and survival with comparison to squamous cell carcinomaGynecol Oncol 2003 88(3):333-9. [Google Scholar]
[7]. AN Viswanathan, MT Deavers, A Jhingran, RT Ramirez, C Levenback, Eifel PJ. Small cell Neuroendocrine carcinoma of Cervix: Outcome and patterns of recurrenceGynecol. Oncol 2004 93(1):27-33. [Google Scholar]