A Heart with Multiple Coronaries Anomalies: Myocardial Bridging, Left Dominance and High Takeoff of Ostia-An Autopsy Case
Lokesh Haswani1, Harendra Kumar M.L2, J Kiran3
1Resident, Department of Pathology,Sri Devaraj Urs Medical College, Tamaka, Kolar, Karnataka, India.
2Professor and HOD, Department of Pathology,Sri Devaraj Urs Medical College, Tamaka, Kolar, Karnataka, India.
3Professor and HOD, Department of Forensic Medicine,Sri Devaraj Urs Medical College, Tamaka, Kolar, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lokesh Haswani, Resident, Department of Pathology, Sri Devaraj Urs Medical College Tamaka, Kolar-563101, Karnataka, India.
Phone: 9036882781,
E-mail: drlokesh.haswani@gmail.Com
Myocardial bridging is a segment of coronary artery that runs intramurally through the myocardium. Though it is commonly seen in the anterior interventricular artery and less commonly in right coronary artery, it can cause limitation in the blood flow, which leads to myocardial ischaemia. Left dominance increases cardiac mortality because of association with the congenital bicuspid aortic valve and myocardial infarction. An earlier study has shown the correlation of myocardial bridging with left coronary circulation and it is rare in relation with right coronary and left dominance. Manifestations of high takeoff of the coronary ostia are highly debatable, with varied opinions given by various authors. It has been believed that myocardial bridging is congenital and that it also causes limitation of blood flow to the myocardium. Cardiac muscles have a unique capability to adapt in response to decreased blood supply, which is in the form of coronary collateral circulation. So, is their any correlation between myocardial bridging and dominance? Herein, we are reporting an unusual autopsy case of myocardial bridging on its right main coronary artery, left coronary dominance and high take off of left main coronary artery in the same heart.
Myocardial bridging, Left dominance, High takeoff, Coronary artery
Introduction
Myocardial bridge is defined as small band of myocardium which overlies the intramural segment of coronary artery, which deviates from its usual course [1-2]. It may be congenital and it is known to cause variety of cardiac complications which may result in sudden death [3] There is wide difference in the incidences of myocardial bridging in autopsy studies (15-45%) as compared to those in angiographic studies (0.5-2.5%) [4] Though majority of population in south India have right coronary dominance, only 11% of population have left dominance [5]. People with left coronary dominance are known to be associated with congenital heart disease [6] and myocardial ischaemia, which result in increased morbidity and mortality [7]. Pathological significance of high takeoff of coronary ostia has been debated, wherein some authors report this to be as associated with myocardial ischaemia, while others report this as a benign condition [8]. It can also create problems for surgeons during catheter cannulations [8]. Herein, we report an unusual autopsy case of myocardial bridging on its right main coronary artery, left coronary dominance and high takeoff of left main coronary artery.
Case Report
A 24-year-male patient who died of poisoning was brought to mortuary. After taken consents of his immediate relatives, autopsy was conducted. The relatives gave the history that, he was agriculturist by occupation, non-smoker, non-alcoholic, and that he did not have any systemic illness. Autopsy was done by following standard protocols and external examination was unremarkable. His heart weighed 250 grams, it was dissected according to “inflow outflow technique” and following findings were noted:
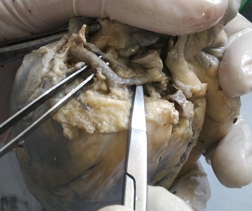
(a) Right coronary artery showed a band of myocardium which was 15 mm long and 3 mm deep, which lay perpendicular to the artery [Table/Fig-1,2].
(b) Left coronary dominance i.e circumflex artery continued as a posterior interventricular artery[Table/Fig-3].
(c)Left coronary artery ostia were 10 mm above the sinotubular junction [Table/Fig-4].
Shows ulcer over thigh and inguinal region

Shows ulcer over thigh and inguinal region

Shows ulcer over thigh and inguinal region
Shows ulcer over thigh and inguinal region

Discussion
Autopsy studies on heart are rarely being done now-a-days, though they are of real value if they are done efficiently. Myocardial bridging was first described by Rymann et al., in autopsy 2 and it is associated with varieties of cardiac complications in the form of angina pectoris, myocardial infarction, coronary spasms, ventricular septal perforations, cardiac arrhythmias and sudden cardiac deaths [3]. The possible pathology for vascular dysfunction is at the level of endothelial or smooth muscle cells which are proximal to the myocardial bridge, not at the level or after the bridge, which can result in coronary spasms [3]. Further, the degree of obstruction caused due to myocardial bridge depends on factors such as location, thickness and length of the muscle bridge [2].
Incidence of dominance of coronary circulation varies in different geographical and ethnic groups [9]. Knowledge on dominance is important for patients undergoing coronary artery interventions and cardiac surgeries [10]. Left dominance produces significantly higher cardiac complications like congenital bicuspid aortic valve and aortic stenosis, [6] myocardial bridging, atherosclerotic coronary disease and total plaque burden, which result in increased cardiac mortality [10].
The significant correlation between left coronary dominance and myocardial bridging was hypothesized by Eren et al., [10] Lokus et al., had found that myocardial bridge in left circulation association was more common with left dominance [11]. Myocardial bridging may be congenital and it may also cause limitation of the blood supply to myocardium which is distal to bridge [3]. Heart has unique property of making a collateral source of blood supply in response to decreased blood flow [12], though myocardial bridging also causes limitation of blood supply. So, there may be some correlation between left dominance and myocardial bridge on opposite vessel. In this case, we found that young male patients had left dominant circulation with myocardial bridge is on right circulation suggestive of the relation between each other
It has been hypothesized that high take off of coronary ostia impairs coronary blood flow due to formation of acute angle with ostial ridge [8]. High take off of coronary ostia, when it is associated with other ostial abnormalities, may result in ischaemia [8]. When it occurs alone, its clinical importance is not documented. However, more haemodynamic studies have to be done to prove the same.
Conclusion
Myocardial bridging which occurs with left coronary dominance has clinical and surgical implications, as it may be associated with cardiac morbidity or mortality. Careful radiographic and angiographic studies should be done in all cardiac patients, especially in those who undergo cardiac interventions, as it may not be benign condition always. More studies on haemodynamics should be done in the patients with high takeoff of coronary ostia, to know its significance.
[1]. M Bandyopadhyay, P Das, K Baral, P Chakroborty, Morphological study of myocardial bridge on coronary arteriesIndian J Thorac Cardiovasc Surg 2010 26:193-97. [Google Scholar]
[2]. Mj Thej, R Kalyani, J Kiran, Atherosclerosis and myocardial bridging: Not a benign combination. An autopsy case reportJ Cardiovasc Dis Res 2012 3:176-8. [Google Scholar]
[3]. T Hayashi, K Ishikawa, Myocardial bridging: harmful or harmlessInt Med 2004 43:1097-8. [Google Scholar]
[4]. MG Bourassa, A Butanaru, J Lesparance, JC Tardiff, Symptomatic myocardial bridges: overview of ischemic mechanisms and current diagnostic and treatment strategiesJ Am Coll Cardiol 2003 41:351-9. [Google Scholar]
[5]. V Reddy, S Lokanadham, Coronary dominance in south Indian populationInt J Med Res Health Sci. 2013 2(1):78-82. [Google Scholar]
[6]. B Chandrasekar, G Sudarshan, KA Abraham, Aortic valve disease and left dominant coronary system a significant associationJ Assoc Physicians India 2000 48(2):210-2. [Google Scholar]
[7]. CE Veltman, FR de Graaf, JD Schuijf, JM van Werkhoven, JW Jukema, PA Kaufmann, Prognostic value of coronary vessel dominance in relation to significant coronary artery disease determined with non-invasive computed tomography coronary angiographyEur Heart J 2012 33:1367-77. [Google Scholar]
[8]. RL Rosenthal, IA Carrothers, JM Schussler, Benign or malignant anomaly? Very high take off of the left main coronary artery above the left coronary sinusTex Heart Inst J 2012 39(4):538-41. [Google Scholar]
[9]. H Das, G Das, DC Das, K Talukdar, A study of coronary dominance in the population of assamJ Anat Soc India 2010 59(2):187-91. [Google Scholar]
[10]. S Eren, E Bayram, F Fil, M Koplay, M Sirvanci, C Duran, An investigation of the association between coronary artery dominance and coronary artery variations with coronary arterial disease by multidetector computed tomographic coronary angiographyJ Comput Assist Tomogr 2008 32:929-33. [Google Scholar]
[11]. M Loukas, B Curry, M Bowers, RG Louis Jr, A Bartczak, M Kiedrowski, The relationship of myocardial bridges to coronary artery dominance in the adult human heartJ Anat 2009 :43-50. [Google Scholar]
[12]. C Seiler, The human coronary collateral circulationEur J Clin Invest 2010 40(5):465-67. [Google Scholar]