Bilateral Absence of Flexor Digitorum Superficialis (FDS) Tendon of the Little Finger: Clinical Significance
Amrita Gupta1, Virendra Kumar2
1PG Resident, Department of Anatomy,Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh-243202, India.
2Professor and Head, Department of Anatomy,Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly, Uttar Pradesh-243202, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Amrita Gupta, PG Resident, Department of Anatomy, Shri Ram Murti Smarak Institute of Medical Sciences, Bareilly,Uttar Pradesh-243202, India.
Phone: 9458705001,
E-mail: ag11677@gmail.com
The flexor digitorum superficialis (FDS/sublimis) is a flexor of the digits of the hand and has been reported to have varying degrees of agenesis. During routine cadaveric dissection for undergraduates at SRMS-IMS Bareilly, India, we observed bilateral absence of the FDS tendon to little finger in the upper limbs of a 45-year-old male cadaver. The muscle was normally supplied by a branch of median nerve in the forearm. Variants of the FDS muscle of the little finger have been reported in the literature. Proper knowledge of muscular variations is essential not only for anatomists but also for orthosurgeons, plastic surgeons and neurologists especially when evaluating possible tendon laceration/dysfunction. The FDS has been used as a motor for a wide variety of tendon transfer operations in the hand.
Flexor digitorum superficialis, Median nerve, Tendon transfer
Case Report
During routine dissection of the front of the forearm for undergraduate teaching in the Department of Anatomy, SRMS-IMS, Bareilly, India, we observed bilateral absence of the FDS tendon to the little finger in the upper limbs of a 45-year-old male cadaver. The muscles of the flexor compartment of both limbs were carefully dissected using Cunningham’s Manual of Anatomy. After stepwise dissection of the front of forearm, we found the normal origin of the muscle by two heads, viz., humero-ulnar and radial head. A branch of median nerve supplied the muscle. The FDS divided distally into 3 tendons (instead of 4) for the ring, middle and index fingers. Relationship with neighbouring structures was found normal and no other associated abnormalities were noticed. Also, no other variation was noted in the course and insertion of the remaining FDS tendons [Table/Fig-1,2]. The Flexor digitorum profundus (FDP) tendon for the little finger remains interconnected with ring and middle finger tendon (except for index finger tendon which seperates early) in the forearm. In the palm, it passes normally through perforated FDS tendon and is inserted to the base of terminal phalanx.
Discussion
FDS is potentially a flexor of all the joints over which it passes, i.e., proximal interphalangeal, metacarpophalangeal and wrist joints. It has independent muscle slips to all medial four fingers and is therefore, able to flex the proximal IP joints individually [1]. Various authors have reported the prevalence of absent little finger FDS in previous cadaveric studies as summarized in [Table/Fig-3].
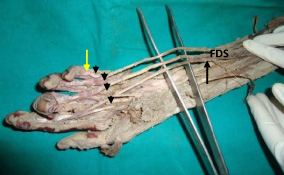
Dissection of the front of the forearm and palmar aspect of the hand (right side) showing absent flexor digitorum superficialis tendon for the little finger (yellow arrow). Flexor digitorum profundus (black arrow head)
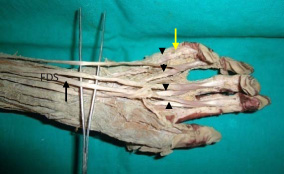
Dissection of the front of the forearm and palmar aspect of the hand (left side) showing absent flexor digitorum superficialis tendon for the little finger (yellow arrow). Flexor digitorum profundus (black arrow head)
Summary of Cadeveric study for incidence of absent little finger FDS tendon as reported in literature
| Authors | Year of Study | Sample Group | Absent Little Finger Fds Tendon |
| Furnas et al.,[2] | 1965 | 100 | 6% |
| Shrewsbury et al., [3] | 1974 | 23 | 30% |
| Ohtani et al., [4] | 1979 | 52 | 2% |
| Austin et al., [5] | 1989 | 40% | 0% |
Evolution of Flexor Digitorum Superflcialis
In the amphibians, there are two layers of forearm flexor muscles and these muscles act as wrist flexors. The fingers in amphibians are flexed by several layers of muscles originated from the palmar aponeurosis or flexor retinaculum, known as the “brevis” type of muscles. During evolution, these brevis muscles disappeared and became the FDP and FDS tendons in the mammals. These evolutionary changes reflect that the hands became a grasping device in higher mammals and became emancipated from locomotor function [6]. From above stated anatomical studies in cadavers and the evolutionary development of the FDS muscle, we postulate that the absence of little finger FDS muscle or tendon may represent an advanced evolutionary stage. This implies to our case study also.
Absence of the tendon for the little finger has been reported by Wood and Macalister [7]. Bowman et al., [8] examined the effect of FDS-absent and FDS-common presentations of the little finger on grip strength and suggested that hand therapists should expect lower results when measuring grip strength of FDS-absent or FDS-common individuals. However, in the present case, bilateral absence of the FDS little finger tendon may contribute to a diminished grip strength. Another study confirming it is by Methot et al., [9] determining the contribution of ulnar digits to overall grip strength.
Study conducted by Godwin et al., [10] suggests that independent FDS function is important for professional musicians playing at an elite level. A lower prevalence of this anatomical variation amongst adults who excel in musical ability could be interpreted as a form of natural selection against a professional musical career. The study confirms that elite violinists and viola players usually have independent FDS function. The same fact can be applied in our case with absent FDS little finger which should not preclude a young player from taking up the musical career.
Richer et al., [11]evaluated the results of transfer of the FDS to the abductor pollicis brevis for restoration of thumb abduction in thenar paralysis caused by advanced chronic Carpal Tunnel Syndrome (CTS) and found satisfactory results for patients with profound CTS and thenar paralysis. The use of the little finger superficialis as the donor motor has minor morbidity compared with other methods and has predictable improvement and patient satisfaction.
Thus, FDS has been used as a motor for a wide variety of tendon transfer operations in the hand. Most of these transfers are on the volar side of the hand and are used to restore synergistic actions (such as opposition of the thumb) or as intrinsic replacements [12]. Recognition of FDS variants is important during surgical repair of tendon lacerations. Variation in the course of the tendon may make it difficult for the operating surgeon in the identification of these tendons during such transfers, especially since tiny incisions are used over known anatomical regions for the release and withdrawal of these tendons during such procedures.
Conclusion
There are several clinical implications of the current study.
Evaluating the hand function is important in the emergency setting. When testing the functions of the finger flexors in patients with hand injury, we should perform both the standard test and the modified test for the little finger.
In patients with absolute little finger FDS function deficit, we should pay special attention when the little finger is injured. If the little finger FDP is lacerated, such a patient will lose all motion in both the PIPJ and DIPJ. Therefore, it is of special importance that the FDP tendon must be repaired to prevent any functional deficit.
The FDS tendon of the little finger can be harvested and be used as tendon graft for hand re-construction without compromising the normal hand function.
The variation reported in the present case is though common in its presentation but, acknowledgement of such variation could be useful for the clinicians, hand surgeons and plastic surgeons in tendon transfer in nerve injures, repair in lacerated injury and hand reconstruction surgeries.
[1]. D Johnson, H Ellis, Pectoral Girdle and Upper Limb: Forearm. In: Standring S, editor. Gray’s Anatomy The Anatomical Basis of Clinical Practice 2005 39th EditionPhiladelphiaElsevier Ltd:876-7. [Google Scholar]
[2]. DW Furnas, Muscle tendon variations in the flexor compartment of the wristPlast Reconstr Surg 1965 (36):320-24. [Google Scholar]
[3]. MM Shrewsbury, K Kuczynski, Flexor digitorum superficialis tendon in the fingers of the human handHand 1974 6:121-30. [Google Scholar]
[4]. O Ohtani, Structure of the flexor digitorum superficialisOkajimas Folia Anat Jpn 1979 56:277-88. [Google Scholar]
[5]. GL Austin, B.M Leslie, L.K Ruby, Variations of the flexor digitorum superficialis of the small fingerJHS (American volume) 1989 14A:262-7. [Google Scholar]
[6]. D Elliot, AR Khandwala, M Kulkarni, Anomalies of the Flexor Digitorum Superficialis MuscleJHS (British volume) 1999 24(5):570-74. [Google Scholar]
[7]. A Macalister, Additional observations on muscular anomalies in human anatomy (third series), with a catalogue of the principal musculsar variations hitherto publishedTrans. Roy. Irish Acad. Sci 1875 25:1-134. [Google Scholar]
[8]. P Bowman, L Johnson, A Chiapetta, A Mitchell, E Belusko, The clinical impact of the presence or absence of the fifth finger flexor digitorum superficialis on grip strengthJ Hand Ther 2003 16(3):245-8. [Google Scholar]
[9]. J Methot, SJ Chinchalkar, RS Richards, Contribution of the ulnar digits to grip strengthCan J Plast Surg 2010 18(1):10-4. [Google Scholar]
[10]. Y Godwin, GAC Wheble, C Feig, Assessment of the presence of independent flexor digitorum superficialis function in the small fingers of professional string players: Is this an example of natural selection?The Journal of Hand Surgery:1-9. [Google Scholar]
[11]. RJ Richer, CA Peimer, Flexor superficialis abductor transfer with carpal tunnel release for thenar palsyJ Hand Surg Am 2005 May 30(3):506-12. [Google Scholar]
[12]. Yilmaz Ali, Bozer Cuneyt, Ulucam Enis, Taskinalp Oguz, An Anomaly of Flexor Muscles of the Fifth (Little) Finger of the Hand: An Anatomical Case ReportClinics. (Sao Paulo) 2009 November 64(11):1133-35. [Google Scholar]