Right Double Inferior Vena Cava (IVC) with Preaortic Iliac Confluence – Case Report and Review of Literature
C.S. Ramesh Babu1, Rekha Lalwani2, Indra Kumar3
1Associate Professor, Department of Anatomy,Muzaffarnagar Medical College, Muzaffarnagar, (U.P), India.
2Associate Professor, Department of Anatomy,A.I.I.M.S., Saket Nagar, (M.P)–462024, India.
3Associate Professor, Department of Anatomy,Hind Institute of Medical Sciences, Safedabad Barabanki (UP)-225003, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. C.S. Ramesh Babu, Associate Professor of Anatomy, Muzaffarnagar Medical College, N.H. 58, Opp. Beghrajpur Industrial Area, Muzaffarnagar, (UP), India.
Phone: +91 9897249202,
E-mail: csrameshb@gmail.com
Anomalies of the inferior vena cava (IVC) are uncommon and most of them remain asymptomatic. Though rare, anomalies of IVC can lead to severe hemorrhagic complications especially during aortoiliac surgery. Prior knowledge of these variations facilitates proper interpretation of radiological images and safe performance of interventional procedures and surgeries. During routine anatomical dissection of abdomen in a female cadaver we observed the presence of right sided duplication of IVC. Both IVCs were present on the right side of abdominal aorta, one ventral and the other more dorsal in position and named ventral right IVC and dorsal right IVC. The ventrally and medially placed IVC, which appeared to be the main IVC was formed by the union of two common iliac veins in front of the right common iliac artery (Preaortic iliac confluence-“Marsupial Cava”). The right external iliac vein continued as the more dorsally and laterally placed dorsal right IVC. The right internal iliac vein after receiving a transverse anastomotic vein from the external iliac continued as the right common iliac vein. This transverse anastomosis was present behind the right common iliac artery. The narrower dorsal right IVC joined the wider ventral right IVC just below the level of renal veins to form a single IVC. The abdominal aorta presented a convexity to the left.
Double inferior vena cava, Marsupial cava, Inferior vena caval anomalies
Case Report
During routine anatomical dissection of retroperitoneum, a very rare anomaly of right sided duplication of IVC with preaortic iliac venous confluence was observed in a female cadaver. Both IVCs were present on the right side of the abdominal aorta, one more ventrally and medially and the other more dorsally and laterally. These two IVCs were designated as ventral right IVC (VRIVC) and dorsal right IVC (DRIVC). The wider VRIVC, which appeared to be the main IVC, was formed by the union of two common iliac veins anterior to the right common iliac artery [Table/Fig-1]. This pattern of formation of IVC in front of right common iliac artery or aortic bifurcation is called “Preaortic iliac confluence” or “Marsupial Cava”. Both common iliac veins were present posteromedial to the respective common iliac arteries. The right common iliac vein was formed by the union of internal iliac vein and an anastomotic vein from external iliac vein passing posterior to the right common iliac artery. The right external iliac vein continued lateral to right common iliac artery as the dorsally and laterally placed DRIVC. Both IVCs joined to form a single trunk just below the level of renal veins[Table/Fig-2]. It appeared that the right common iliac artery was passing through a venous ring [Table/Fig-3]. Right ovarian vein drained into VRIVC. The left renal vein received left ovarian and left suprarenal veins. The abdominal aorta presented a slight convexity to the left. Right ureter was normal in its position and relations lying lateral to both vena caval channels and crossing the bifurcation of common iliac artery [Table/Fig-3].
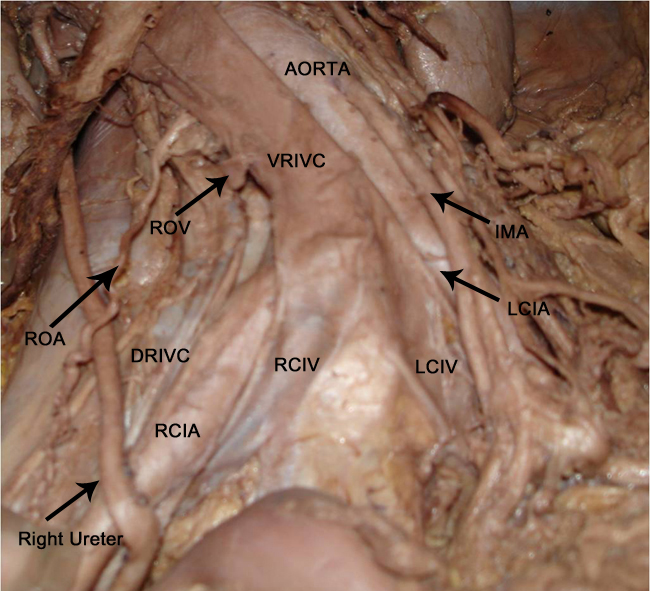
Right double inferior vena cava with preaortic iliac vein confluence. Note the formation of ventral right IVC (VRIVC) by preaortic confluence of right common iliac vein (RCIV) and left common iliac vein (LCIV). The dorsal right IVC (DRIVC) ascend lateral to right common iliac artery (RCIA) in a more dorsal position. Right ureter descends lateral to both IVCs and cross bifurcation of RCIA. AA-Abdominal aorta; LCIA-left common iliac artery; IMA-inferior mesenteric artery; ROA-Right ovarian artery; ROV-Right ovarian vein (cut)
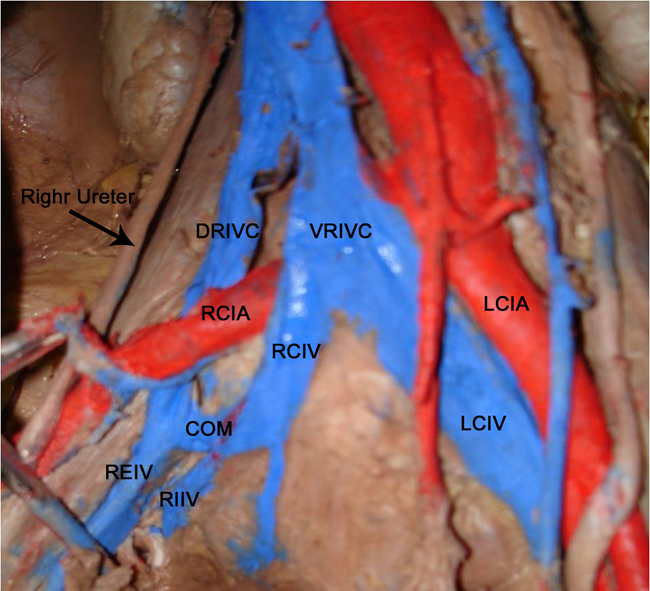
Right external iliac vein (REIV) ascend as the dorsal right IVC (DRIVC) after giving a communicating branch (COM) which joins with right internal iliac vein (RIIV) to form right common iliac vein (RCIV). Larger ventral right IVC (VRIVC) is formed anterior to aortic bifurcation by the union of RCIV and left common iliac vein (LCIV). Right common iliac artery is pulled aside and Internal iliac artery is cut to show the formation of RCIV.
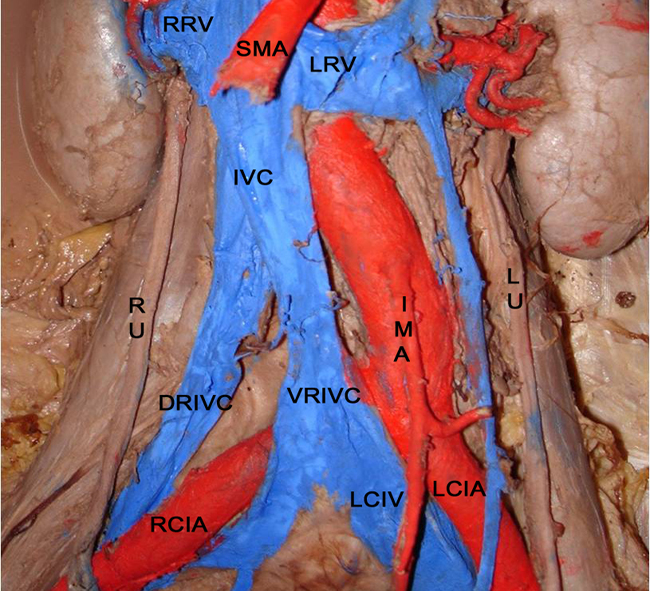
Right common iliac artery (RCIA) appear to pass through a venous ring between ventral right IVC (VRIVC) and dorsal right IVC (DRIVC). Formation of VRIVC by preaortic iliac venous confluence is also seen. Both ureters are crossing bifurcation of common iliac arteries. Right ureter (RU) is lateral to both IVCs. LU-Left ureter; LRV-Left renal vein; RRV-Right renal vein; SMA-Superior mesenteric artery; IMA-Inferior mesenteric artery; LCIV-Left common iliac vein; LCIA-Left common iliac artery
Features of cases of preaortic iliac venous confluence
| Sl. No. | Name of author and year | No. of cases | Modality of finding | Remarks |
| 1 | McClure & Huntington, 1929 [5] | 2 | NA) | ------ |
| 2 | Gladstone, 1929 [6] | 1 | Postmortem anatomic dissection | |
| 3 | Brener et al., 1974 [8] | 1 | Intraoperative | Infrarenal abdominal aortic aneurysm (AAA) |
| 4 | Baldridge et., al. 1987 [9] | 1 | Intraoperative | Ruptured AAA |
| 5 | Vohra & Leiberman, 1991 [10] | 1(F) | Intraoperative | Retropsoas right common iliac artery |
| 6 | Harman & Kopecky, 1992 [11] | 1 | CT | ---- |
| 7 | Panicek et al., 1992 [7] | 1(F) | CT postoperative | Operated for mesodermal mixed ovarian tumor |
| 8 | Ruemenapf et al., 1998 [1] | 2(M) | Intraoperative | AAA. Venous anomaly not detected in preoperative CT & Angiography |
| 9 | Schiavetta et al., 1998[12] | 1(M) | Intraoperative | Ruptured AAA. Not detected in CT |
| 10 | Shindo et al., 1999 [13] | 1(M) | CT | Infrarenal AAA. Retrocaval ureter. |
| 11 | Natsis et al., 2003 [14] | 1 | Anatomic dissection | ---- |
| 12 | Rocha et al., 2008 [15] | 4 (F-3; M-1) | MDCT | 2 cases with renal mass. |
| 13 | Masood et al., 2008 [16] | 1(M) | Intraoperative | Aneurysmal repair |
| 14 | Rhissassi et al., 2011 [17] | 2 (M-1; F-1) | Intraoperative | Preoperative CT could not detect the anomaly. AAA. |
| 15 | Present case, 2013 | 1(F) | Anatomic dissection | Right double inferior vena cava with ventral IVC showing preaortic iliac confluence. . |
Features of cases of right double inferior vena cava
| Sl. No. | Name of author and year | No. of cases | Sex | Comparison of size of two IVCs. (Ventral = V Dorsal = D) | Level of confluence of the two IVCs from renal veins confluence | Drainage site of right gonadal vein | Remarks |
| 1 | Doyle et al., 1992 [19] | 1 | M | V > D | At the level of renal veins | NA | ------ |
| 2 | Meyer et al., 1998 [20] | 1 | NA | V > D | Caudal to renal veins | NA | Spiral CT |
| 3 | Nagashima et al., 2006[22] | 5 | M-2 F-3 | V > D – 3 V < D – 1 V = D -1 | Caudal to renal veins | V.IVC – 4 IVC -1 | CT. Left common iliac vein continued as Ventral IVC crossing ventral to aortic bifurcation or right common iliac artery. Right common iliac vein continued as Dorsal IVC. No interiliac communication. |
| 4 | Senecail et al., 2004 [21] | 1 | F | V < D | Caudal | V.IVC | CT. VIVC continuation of LCIV. DIVC formed by RCIV with an anastomotic branch from LCIV |
| 5 | Tagliafico et al., 2007 [18] | 1 | M | V < D | Caudal to renal veins | V.IVC | US, CT. Venous ring encircling right common iliac artery. |
| 6 | Ng and Ng, 2009 [23] | 1 | F | NA | At renal veins level | NA | US, MRI. Left common iliac vein passed behind aorta and ascended as double IVC. |
| 7 | Gong et al., 2011 [24] | 1 | F | NA | Midsegment duplication | NA | Partial right double IVC with circumcaval ureter |
| 8 | Present Case, 2013 | 1 | F | V > D | Caudal to renal veins | V.IVC | Ventral IVC showing Preaortic iliac venous confluence; Dorsal IVC continuation of right external iliac vein |
Discussion
Congenital anomalies of the IVC occur in approximately 2% to 3% of patients[1] and are detected incidentally since most of them are clinically silent. The incidence of double IVC or duplication of IVC was reported to be 0.2 % - 3 % [2]. Ipsilateral duplication of IVC is extremely rare. Review of 1788 contrast enhanced spiral CT scans of abdomen revealed an incidence of 0.39 % for duplication of IVC and not a single case of preaortic iliac vein confluence and right sided duplication was found in this retrospective review [3] Anomalies of IVC are unusual manifestations of a complex process of embryogenesis involving anastomosis between three paired venous channels (posterior cardinal, supracardinal and subcardinal) with enlargement and consolidation of some vessels due to hemodynamic changes and regression of others.
Normally the IVC is formed by the union of the two common iliac veins posterior to right common iliac artery. Formation of IVC anterior to right common iliac artery or aortic bifurcation is named as Preaortic iliac confluence [4]. Earliest reports of such anomalous formation appeared in the year 1929 [5-6]. This anomaly is very rare in humans but normal in Marsupial animals and hence the term “Marsupial Cava [7]. Many cases of this anomaly reported in the literature were detected incidentally during abdominal aortic aneurysm surgery [8-13]. Natsis et al.,[14] described an anatomical finding of a case of preaortic iliac confluence and Rocha et al., [15] detected four such cases and including them counted 17 such cases till 2008. Later 3 more cases were reported thus making a total of 20 cases [16-17]. In most of these cases preaortic iliac confluence formed a normal orthotopic IVC in a right lateroaortic position [Table/Fig-4].
Tagliafico et al., [18] described a case of double right IVC in which a venous ring encircled the right common iliac artery. Though the authors did not use the term preaortic iliac confluence, the formation of ventral IVC appeared to be preaortic iliac venous confluence. To the best of our knowledge this is the first case report of right double IVC associated with preaortic iliac confluence.
Among the anomalies of IVC, the most common is double IVC with an incidence of 0.2% - 3 % [2]. Classically the double IVC indicates the presence of right and left IVC on either side of the abdominal aorta representing the persistence of both right and left supracardinal veins. Ipsilateral duplication of IVC is very rare. Right double IVC is defined as the presence of two infrarenal IVCs lying to the right of the abdominal aorta. Doyle et al., [19] first reported ipsilateral duplication of IVC and later two more reports of right sided duplication of IVC were published [20-21]. Nagashima et al., [22]described five cases of right double IVC with a ventral and dorsal relationship between the two IVCs. All five cases also exhibited preaortic left common iliac vein which continued as ventrally placed IVC and the right common iliac vein continued as dorsally placed IVC without any interiliac anastomosis. Ng and Ng [23] reported a right sided double IVC by MR imaging with the passage of left common iliac vein behind the aorta and ascending as double IVC. Both right sided IVCs generally unite to form a single trunk at or below the level of renal veins. A partial double right IVC with a circumcaval ureter passing through the split between them was also reported but the ipsilateral duplication involved only the mid portion of the IVC with cranial and caudal segments being single [24] [Table/Fig-5].
Reporting a case of double IVC in a male cadaver, Tsuyoshi et al., [25] described the continuation of left external iliac vein as the left IVC lying to the left of abdominal aorta and the formation of a normal right IVC by the union of both common iliac veins. The left common iliac vein was formed by the union of internal iliac and a branch from the external iliac. Similarly in the present case also the right external iliac vein after giving a communicating branch to the internal iliac continued as the more dorsally placed right IVC.
Speculating the development of right double IVC, Nagashima et al., [22] argued that the ventral vessel originates from the right subcardinal vein and the dorsal vessel from the right supracardinal vein because embryologically the right subcardinal vein lies ventral to the right supracardinal vein and the right gonadal vein derived from the right subcardinal drained into the ventral vessel. The ureter must course laterally with respect to the double right IVC channels to rule out the persistence of right posterior cardinal vein [26]. Persistent right posterior cardinal vein would have resulted in the retrocaval ureter. In the present case, ureter was placed lateral to both right sided IVC channels suggesting that the double right IVC was due to the persistence of both right supracardinal and right subcardinal veins. Embryologically the preaortic iliac confluence probably represents the persistence of the ventral limb of circumumbilical venous ring which surrounds the future common iliac arteries on each side and regression of dorsal limb of the venous ring. Normally the ventral portion of the venous ring disappears. This conformation is similar to the normal formation of left renal vein but occurs in a more caudal location at the level of aortic bifurcation.
Conclusion
Anomalies of IVC are rare and clinically asymptomatic and may remain undetected. These anomalies are important entities to the radiologists and vascular surgeons. Since some of the venous anomalies are frequently overlooked during preoperative evaluation, intraoperative awareness is most essential to avoid unexpected surgical hazards. Most important clinical consequences of double IVC with preaortic iliac confluence are observed in abdominal aortic aneurysm surgery, reptroperitoneal surgeries, placement of IVC filters and surgical ligation of IVC. Thrombosed double IVC may be mistaken for lymphadenopathy or a retroperitoneal mass. The importance of awareness of these venous anomalies cannot be undermined because of their rarity.
[1]. G Ruemenapf, H Ruppracht, H Schweiger, Preaortic iliac confluence: A rare anomaly of the inferior vena cavaJ Vasc Surg 1998 27(4):767-71. [Google Scholar]
[2]. JM Giordano, HH Trout, Anomalies of the inferior vena cavaJ Vasc Surg 1986 2:924-28. [Google Scholar]
[3]. B Aljabri, PS Mac Donald, R Satin, LS Stein, DI Obrand, OK Steinmetz, Incidence of major venous and renal anomalies relevant to aorto- iliac surgery as demonstrated by computed tomographyAnn Vasc Surg 2001 15(6):615-18. [Google Scholar]
[4]. EA Edwards, Clinical anatomy of lesser variations of the inferior vena cava: a proposal for classifying the anomalies of this vesselAngiology 1951 2:85-99. [Google Scholar]
[5]. CFW Mc Clure, GS Huntington, The mammalian vena cava posterior: an ontogenic interpretation of the atypical forms of the vena cava posterior (inferior) found in adult domestic cat (Felis domestica) and in manAm Anat Memoir 1929 15:1-55. [Google Scholar]
[6]. RJ Gladstone, Development of the inferior vena cava in the light of recent research, with especial reference to certain abnormalities and current description of the ascending lumbar and azygos veinsJ Anat 1929 64:70-93. [Google Scholar]
[7]. DM Panicek, PV O’Moore, RA Castellino, Preaortic iliac venous confluence (“Marsupial cava”): a rare anomaly of the inferior vena cavaUrol Radiol 1992 14(3):188-90. [Google Scholar]
[8]. BJ Brener, RC Darling, PL Frederick, RR Linton, Major venous anomalies complicating abdominal aortic surgeryArch Surg 1974 108:159-65. [Google Scholar]
[9]. Jr Baldridge ED, AJ Canos, Venous anomalies encountered in aortoiliac surgeryArch Surg 1987 122(10):1184-88. [Google Scholar]
[10]. R Vohra, DP Leiberman, An anomalous right iliac artery presenting as iliac stenosisEur J Vasc Surg 1991 5:209-11. [Google Scholar]
[11]. JT Harman, KK Kopecky, Preaortic iliac confluence: 2D and 3D CT findingsComput Med Imaging Graph 1992 16:51-53. [Google Scholar]
[12]. A Schiavetta, R Cerruti, C Cantello, P Patrone, “Marsupial Cava” and ruptured abdominal aortic aneurysm. A case report and review of the literatureJ Vasc Surg 1998 28:719-22. [Google Scholar]
[13]. S Shindo, M Kobayashi, S Kaga, H Hurukawa, K Kubota, A Kojima, Retrocaval ureter and preaortic iliac venous confluence in a patient with an abdominal aortic aneurysmSurg Radiol Anat 1999 21(2):147-49. [Google Scholar]
[14]. K Natsis, G Iordache, P Xepoulias, P Tsikaras, Preaortic iliac Venous confluence. Marsupial vena cava. Case ReportMorphologie 2003 87(277):21-23. [Google Scholar]
[15]. MDS Rocha, RB Lourenco, YS Chang, EM Gebrim, Cerri GG.-Preaortic iliac confluence (Marsupial vena cava): report of 4 casesJ Comput Assist Tomogr 2008 32(5):706 [Google Scholar]
[16]. M Massod, WD Neary, S Ashley, Preaortic confluence of the common iliac veins complicating elective abdominal aortic aneurysm surgeryEur J Vasc Endovasc Surg 2008 36(2):245 [Google Scholar]
[17]. B Rhissassi, A Bahnini, E Kieffer, Preaortic left primitive iliac vein: Two case studiesAnn Vasc Surg 2011 25(2):269-3. [Google Scholar]
[18]. A Tagliafico, E Capaccio, I Rosenberg, C Martinoli, LE Derchi, Double right inferior vena cava associated with an anomalous venous ring encircling the right common iliac artery: Report of one case with CT and USEur J Radiol Extra 2007 64(3):111-15. [Google Scholar]
[19]. AJ Doyle, MG Melendez, MA Simons, psilateral duplication of the inferior vena cavaJ Clin Ultrasound 1992 20:481-85. [Google Scholar]
[20]. DR Meyer, R Andresen, M Friedrich, Right sided double inferior vena cava and common iliac vein: imaging with spiral computerized tomographyAktuelle Radiol 1998 8(3):148-50. [Google Scholar]
[21]. B Senecail, T Josseaume, J Bobeuf, Right sided duplication of the inferior vena cavaMorphologie 2004 88(283):183-87. [Google Scholar]
[22]. T Nagashima, J Lee, K Andoh, T Itoh, K Tanohata, M Arai, Right double inferior vena cava: Report of 5 cases and literature reviewJ Comput Assist Tomogr 2006 30(4):642-45. [Google Scholar]
[23]. WT Ng, SSM Ng, Double inferior vena cava: a report of three casesSingapore Med J 2009 50(6):e211-e13. [Google Scholar]
[24]. J Gong, H Jiang, T Liu, Q Yuan, L Sun, J Yang, Imaging of partial right double vena cava with ureter crossing through its split, confirmed at surgeryClin Imaging. 2011 35(2):148-50. [Google Scholar]
[25]. S Tsuyoshi, K Sadaharu, W Koichi, Y Akira, S Hiroko, H Takeshi, A case of the double inferior vena cava with hepatofugal collateralJ Kurume Med Assoc 2005 68((11/12)):339-45. [Google Scholar]
[26]. I Pedrosa, E Zeikus, DE Green, MV Gosselin, System Venous, In “CT and MR Angiography Comprehensive Vascular Assessment” GD Rubin and NM Rofsky (Ed). Wolters Kluwer / Lippincott Williams & Wilkins,Clin Imaging 2009 Philadelphia:1189-92. [Google Scholar]