Psychomotor Retardation, Attention Deficit and Executive Dysfunctional in Young Non-hospitalised Un-medicated Non-psychotic Unipolar Depression Patients
Kamini Ramdas Ilamkar1
1 Assistant Professor, Department of Physiology and Government Medical College, Nagpur, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kamini Ramdas Ilamkar, Plot No. 9. Parth Apartment S.E. Rly-Colony-2, Telecom Nagar, Nagpur-440022, Maharashtra, India. Phone no. 8407910505
Background: Neuropsychological deficits have been reported in patients with Major Depressive Disorder (MDD) during an acute episode. The reaction time gives an idea about integrity and the processing ability of central nervous system. The simple reaction time task is an attention seeking task that focuses primarily on speed of processing (executive function). Psychomotor retardation (i.e., delay at the output which includes perceptual decision, planning, motor process) is a constant and probably central feature of depression.
Aims: The purpose of present study was to evaluate the neuropsychological functioning in young non-hospitalised un-medicated non-psychotic unipolar depression by focusing on tasks related to prefrontal cortex functioning.
Materials and Methods: Newly diagnosed young antidepressant-free, clinically depressed patients (20 males and 24 females, n=44) and healthy controls (24 males and 27 females, n=51) pair-wise matched on gender, age (mean age 25±4) were included in this study. All patients were diagnosed with major depressive episode according to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Both the patients and healthy controls performed a simple reaction time task with components of alerting auditory and visual orientation of attention by an instrument response analyzer.
Statistical Analysis : The performances were expressed in mean ± standard deviation of the reaction time by using the Student’s unpaired t-test.
Results: Patients with unipolar depression relative to controls were impaired on psychomotor performance and deficits in sustained attention remained significant.
Conclusions: These findings suggest deficits in sustained attention as vulnerability marker for unipolar depression. With further methodologically sound research, the changes in neuropsychological function associated with treatment response may provide a means of evaluating different treatment strategies in major depression.
Unipolar depression, Psychomotor retardation, Attention deficits, Executive dysfunction, Dorsolateral prefrontal cortex, Simple reaction time
Introduction
The time interval between the delivery of visual and auditory stimulus and motor response, is termed as the “reaction time”. It has physiological significance as being a non-invasive test for peripheral as well as central nervous system. The reaction time gives an idea about integrity and the processing ability of central nervous system. The simple reaction time task is an attention seeking task that focuses primarily on speed of processing (executive function). Psychomotor retardation (i.e., delay at the output which includes perceptual decision, planning, motor process) is a constant and probably central feature of depression. Widlocher and Hardy-Bayle [1] found that reaction time performance of depressed people was generally worse than that of non-depressed controls which indicates that a dysfunction of information processing accompanies the depression states would result from the impairment of all processing stages. Van der Molen et al., [2] proposed a 6-stage decomposition of infor- mation processing: 3 perceptual stages, stimulus pre-processing, feature analysis and stimulus identification, a central, response selection stage, and 2 motor stages, motor programming and motor adjustment. This hypothesis entails that any factor affecting reaction time should exhibit a longer effect in depressed than in non-depressed subjects thus depression impairs stimulus identification. Both logical considerations and empirical evidence suggest that stimulus intensity affects stimulus pre-processing and that stimulus-response compatibility affects response selection. The term executive function defines complex cognitive processing requiring the co-ordination of several subprocesses to achieve a particular goal. Neuropsychological evidence suggests that executive processing is intimately connected with the intact function of the frontal cortices. Executive dysfunction has been associated with a range of disorders, and is generally attributed to structural or functional frontal pathology [3].
Objectives
To determine the psychomotor retardation, attention deficits and executive dysfunction in nonpsychotic unipolar depression.
Materials and Methods
The study was conducted in the Department of Physiology, Government Medical College and Hospital, Nagpur, India, comprising of young newly diagnosed antidepressant-free, clinically depressed patients (20 males and 24 females, n=44) and healthy controls (24 males and 27 females, n=51) pair-wise matched on gender and age range (mean age 25±4). All patients were diagnosed with major depressive episode according to DSM-5 [4]. Psychopathology was measured using Hamilton Depression Scale (HDS) [5] in unmedicated non-psychotic unipolar depressive patients, minimum score of 18 on Hamilton Depression Rating Scale (HDRS) were included in the study. Patients were recruited from the in- and outpatient services of the department of psychiatry. The study was approved by the local Ethics Committee of the hospital. Informed consent was given by all the patients and healthy controls prior to participation in the study. All subjects including the patients and healthy controls performed a simple reaction time task with components of alerting auditory and visual oriention of attention by a reaction time instrument (a response analyzer) by the Yantrashilpa System, Pune, India, in a quiet room with good visibility conditions. The subjects were asked to sit comfortably on chairs in front of the table on which the response analyzer was placed. They were then explained about the details and the procedure of the test. All the subjects in the study were right handed and they responded with their right hands. Reaction times were analyzed by unpaired t-test. Both auditory and visual reaction time was slowed within depressive patients. Both patients and controls underwent a clinical examination by a physician, psychiatrist, and neurologist to exclude any neurological or psychiatric disease, alcohol or substance abuse. Screening procedures included the medical history, physical and neurological examination, Electrocardiogram (ECG), thyroid function studies, were also done to exclude cardiovascular diseases, hyperthyroidism, hypothyroidism disorder.
The inclusion criteria for MDD included:
Newly diagnosed young nonhospitalised, unmedicated, non-psychotic unipolar, and depressive patients who gave their informed consent and were not on any treatment currently.
Any psychiatric illness or any other central nervous system disorders that could interfere with the memory and the psychomotor functions, except depression.
Normal hearing and vision.
The exclusion criteria for MDD included:
The MDD patients who were unable to cooperate or understand the instructions.
The inclusion criteria for the controls included:
Normal hearing and vision.
The exclusion criteria for the controls included:
A psychiatric disorder or having a first degree relative with such a history.
Results
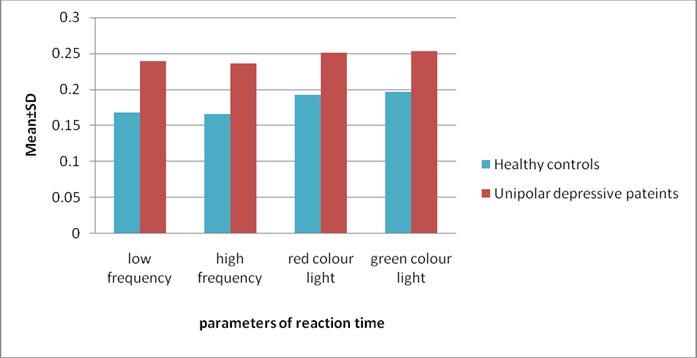
The reaction time was measured by using the following parameters: For the auditory reaction time: a low frequency sound and a high frequency sound were included and for the visual reaction time: a red colour light and a green colour light were included [Table/Fig-1 & 2]:
Showing mean value with standard deviation of unipolar depressive patients is higher than those of healthy controls and was statistically very highly significant.
| Parameters of reaction time (seconds) | Healthy controls [Mean ± SD] | Unipolar depressive patients [Mean ± SD] | p-value |
|---|
| Auditory reaction time (seconds) | low frequency sound | 0.168±0.009 | 0.239 ± 0.033 | 0.0001 |
| High frequency sound | 0.165±0.010 | 0.236 ± 0.033 | 0.0001 |
| Visual reaction time (seconds) | Red colour light | 0.192±0.010 | 0.251 ± 0.030 | 0.0001 |
| Green colour light | 0.196±0.010 | 0.253 ± 0.030 | 0.0001 |
Showing comparison and analysis between healthy controls and unipolar depressive patients for reaction time
Discussion
Results indicate that young nonhospitalised unmedicated non-psychotic unipolar depressive disorder patients show significant attention impairments on most measures of effortful attention, and the magnitude of these impairments increases as the effortful demands of the task increase [6,7]. Patients with depression have neuropsychological deficits in attention, memory, psychomotor speed, processing speed, and executive function although it is not clear, whether neurocognition in depression is impaired in a global or nonspecific way or if specific cognitive domains are selectively impaired [8–16]. The time of maximal response preparation occurred later in depressives than in controls showing clear evidence of pure retardation of mentation [17]. Depression might affect thinking, memory concentration, perception and interpretation [18]. Cognitive functioning in depressive disorders seems to be characterized by a reduced speed of information processing in automatic subtasks [19]. Depressed participants display longer reaction time then control participants and suggested that depression spares the stage of stimulus pre-processing but affects the stage of motor adjustment, i.e., depression alters the stage of response selection [20]. In major depression, particular neuropsychological domains are more strongly related to clinical state is psychomotor speed. In contrast, measures of attention and executive functioning perhaps represent more trait-like markers of major depression. With further methodologically sound research, the changes in neuropsychological function associated with treatment response may provide a means of evaluating different treatment strategies in major depression [21]. Although deficits in sustained attention remained significant [22]. Executive functions involve a set of cognitive behaviours which include: dealing with novelty, selecting strategies, inhibiting incorrect responses, monitoring performance and using feedback to adjust future responding. Unipolar depressed patients mainly exhibit cognitive inhibition deficits, problem-solving impairments and planning deficits. Cognitive inhibition deficits in depressed patients have been related to a reduction of cognitive resources and psychomotor retardation. Inhibition disturbance could lead depressed patients to process irrelevant information and consequently reduce their capacity to control transient mood changes. Brain imaging studies show that reduced blood flow, particularly in medial prefrontal cortex and dorsal anterior cingulate cortex subserve executive impairments in depression. However neuroimaging studies underscore the importance of mood-cognitive interactions in depression. A recent working model of depression implicates failure of the coordinated interactions of distributed cortical-limbic pathways in the neuropsychopathology of depression. According to this model, neocortical (prefrontal and parietal regions) and superior limbic elements (dorsal anterior cingulate) are postulated to mediate impaired attention and executive function [23]. The neurobiological implications of the present results are in accordance with the hypothesis that there is a global-diffuse impairment of brain function with particular involvement of the frontal lobes [24]. Based on clinical neuropathological and neuroimaging findings suggesting that frontostriatal dysfunctions contribute to the development of both depression and executive dysfunction and influence the course of depression. Depressive symptomatology, and especially psychomotor retardation and loss of interest in activities, contributed to disability in depression-executive dysfunction syndrome patients [25]. Prominent models of the neurobiology of depression implicate involvement of the anterior cingulate cortex (ACC) and the dorsolateral prefrontal cortex (DLPFC). The evidence from combined imaging and neuropsychological studies supports the involvement of the ACC, but is less clear in the case of the DLPFC [26]. However study of neuropsychological mechanisms in emotional disorders using functional imaging methods reviews evidence that strongly implicating the dorsolateral prefrontal cortex, particularly in the right hemisphere, as a key brain structure in emotion/cognition interactions in negative mood states, thus depression interferes with right hemisphere function in part by influencing right hemisphere arousal mechanisms [27,28].
Conclusion
The reaction time is an indirect index of the processing capability of the central nervous system and is the simple means for determining the sensory motor association and the performance of an individual. The reaction time may also be employed to determine the effects of therapy in MDD patients. It may provide an adjunct to the tests for the psychological functioning and a crucial aid to the diagnosis.
Implication
Simple Reaction Time (SRT) tasks are particularly suited for examining psychomotor retardation because they test the decision process while avoiding motivation and attention interference. Psychomotor retardation is a constant and probably central feature of depression. Means available for measuring it can be used to assess the effects of antidepressants on specific clinical dimensions. Increasing recognition of the neurologic aspects of depressive disorder has aroused new interest in the potential neuropathologic significance of “psychomotor” symptoms in depression. The exact cause of depression is not known. Many researchers believe it is caused by chemical changes in the brain. This may be due to a problem with your genes, or triggered by certain stressful events. More likely, it’s a combination of both. Some types of depression run in families. But depression can also occur if you have no family history of the illness. Anyone can develop depression, even kids.
[1]. Widlocher DJ, Hardy-Bayle MC, Cognition and control of action in psychopathologyEuropean Bulletin of Cognitive Psychology 1989 9:583-615. [Google Scholar]
[2]. Van der Molen MW, Bashore TR, Halliday R, Callaway E, Chronopsychophysiology: Mental chronometry augmented with physiological measuresHandbook of Cognitive Psychophysiology 1991 [Google Scholar]
[3]. Elliott R, Executive functions and their disordersBr Med Bull 2003 65:49-59. [Google Scholar]
[4]. Diagnostic and Statistical Manual of Mental Disorders: (Fifth Edition) DSM-5. Section II Diagnostic criteria and codes-Deprressive disorder and the “Bereavement Exclusion”American Psychiatric Association 2013 [Google Scholar]
[5]. Hamilton M, A rating scale for depressionJournal of Neurology, Neurosurgery, and Psychiatry 1960 23:56-62. [Google Scholar]
[6]. Cohen R, Lohr I, Paul R, Boland R, Impairments of attention and effort among patients with major affective disordersJ Neuropsychiatry Clin Neurosci 2001 summer 13(3):385-95. [Google Scholar]
[7]. Hammar A, Lund A, Hugdahl K, Long-lasting cognitive impairment in unipolar major depression: a 6-month follow-up studyPsychiatry Res 2003 May 30 118(2):189-96. [Google Scholar]
[8]. Hammar A, Lund A, Hugdahl K, Selective impairment in effortful information processing in major depressionJ Int Neuropsychol Soc 2003 Sep 9(6):954-9. [Google Scholar]
[9]. Gualtieri CT, Johnson LG, Benedict KB, Neurocognition in depression: patients on and off medication versus healthy comparison subjectsJ Neuropsychiatry Clin Neurosci Spring 2006 18(2):217-25. [Google Scholar]
[10]. Matthews K, Coghill D, Rhodes S, Neuropsychological functioning in depressed adolescent girlsJ Affect Disord 2008 Nov 111(1):113-8. [Google Scholar]
[11]. Caligiuri MP, Ellwanger J, Motor and cognitive aspects of motor retardation in depressionJ Affect Disord 2000 Jan-Mar 57(1-3):83-93. [Google Scholar]
[12]. Lemke MR, Motor signs of depressionNervenarzt 1999 Jul 70(7):600-12. [Google Scholar]
[13]. Dantchev N, Widlocher DJ, The measurement of retardation in depressionJ Clin Psychiatry 1998 59(Suppl 14):19-25. [Google Scholar]
[14]. Sobin C, Mayer L, Endicott J, The motor agitation and retardation scale: a scale for the assessment of motor abnormalities in depressed patientsJ Neuropsychiatry Clin Neurosci 1998 10(1):85-92. [Google Scholar]
[15]. Popescu C, Ionescu R, Jipescu Cognitive and motor retardation in depressionRom J Neurol Psychiatry 1994 Oct-Dec 32(4):201-17. [Google Scholar]
[16]. Parker G, Hadzi-Pavlovic D, Brodaty H, Boyce P, Mitchell P, Wilhelm K, Psychomotor disturbance in depression: defining the constructsJ Affect Disord 1993 Apr 27(4):255-65. [Google Scholar]
[17]. Smith MJ, Brebion G, Banquet JP, Cohen L, Retardation of mentation in depressives: Posner’s covert orientation of visual attention testJournal of Affective Disorders 1995 35:107-15. [Google Scholar]
[18]. Ahearn EP, Carroll BJ, Short term variability of mood ratings in unipolar and bipolar depressed patientsJournal of Affective Disorders 1996 36:107-115. [Google Scholar]
[19]. Den Hartog HM, Derix MM, Van Bemmel AL, Kremer B, Jolles J, Cognitive functioning in young and middle aged unmedicated out patients with major depression:testing the effort and cognitive speed hypothesesPsychol Med 2003 33(8):1443-51. [Google Scholar]
[20]. Bonin-Guillaume S, Blin O, Hasbroucq T, An additive factor analysis of the effect of depression on the reaction time of old patientsActa Psychol (Amst) 2004 117(1):1-11. [Google Scholar]
[21]. Douglas KM, Porter RJ, Longitudinal assessment of neuropsychological function in major depressionAust N Z J Psychiatry 2009 Dec 43(12):1105-17. [Google Scholar]
[22]. Weiland-Fiedler P, Erickson K, Waldeck T, Luckenbaugh DA, Pike D, Bonne O, Evidence for continuing neuropsychological impairments in depressionJ Affect Disord 2004 Oct 15 82(2):253-8. [Google Scholar]
[23]. Fossati P, Ergis AM, Allilaire JF, Executive functioning in unipolar depression: a reviewEncephale 2002 Mar-Apr 28(2):97-107. [Google Scholar]
[24]. Landro NI, Stiles TC, Sletvold H, Neuropsychological function in nonpsychotic unipolar major depressionNeuropsychiatry Neuropsychol Behav Neuroi 2001 Oct-Dec 14(4):233-40. [Google Scholar]
[25]. Thomas P, Hazif Thomas C, Billon R, Peix R, Faugeron P, Clement JP, Depression and frontal dysfunction: risks for the elderly?Encephale 2009 Sep 35(4):361-9. [Google Scholar]
[26]. Rogers MA, Kasai K, Koji M, Fukuda R, Iwanami A, Nakagome K, Executive and prefrontal dysfunction in unipolar depression: a review of neuropsychological and imaging evidenceNeurosci Res 2004 Sep 50(1):1-11. [Google Scholar]
[27]. Liotti M, Mayberg HS, The role of functional neuroimaging in the neuropsychology of depressionJ Clin Exp Neuropsychol 2001 Feb 23(1):121-36. [Google Scholar]
[28]. Liotti M, Tucker DM, Right hemisphere sensitivity to arousal and depressionBrain Cogn 1992 Mar 18(2):138-51. [Google Scholar]