Epidemiology of Premenstrual Syndrome (PMS)-A Systematic Review and Meta-Analysis Study
Ashraf Direkvand-Moghadam1, Kourosh Sayehmiri2, Ali Delpisheh3, Satar Kaikhavandi4
1 PhD Student, Psychosocial Injuries Research Center, Ilam University of Medical Sciences, Ilam, Iran.
2 Research Group, Psychosocial Injuries Research Center, Ilam University of Medical Sciences, Ilam, Iran.
3 Research Group, Psychosocial Injuries Research Center, Ilam University of Medical Sciences, Ilam, Iran.
4 Research Group, Psychosocial Injuries Research Center, Ilam University of Medical Sciences, Ilam, Iran.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Satar Kaikhavandi, Psychosocial Injuries Research Center, Ilam University of Medical Sciences, Ilam, Iran. Tel/Fax: 0098-841- 2227126,
E-mail: skaikhavani@yahoo.com
Background and Objectives: Premenstrual Syndrome (PMS) is a common health problem in women in reproductive age. The present study aimed to investigate the prevalence of PMS using meta-analysis method.
Methods: This meta-analysis systematically reviewed the prevalence of PMS. A search was conducted using keywords Premenstrual Syndrome, PMS, prevalence PMS and symptom of PMS in reliable English articles. The initial search 53 articles were available. After review of full-text articles, 17 articles were selected for analysis. Data were combined using meta-analysis (random effects model). Data were analyzed using STATA software, Version 11.1
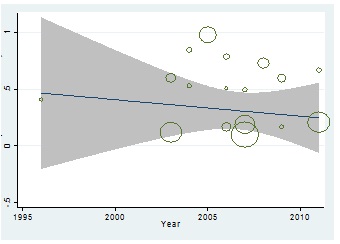
Results: Overall, 17 studies met our inclusion criteria. The pooled prevalence of PMS was 47.8% (95% CI: 32.6-62.9). The lowest and highest prevalence were reported in France 12% (95% CI: 11-13) and Iran 98% (95% CI: 97-100) respectively. However, meta-regression scatter plot showed an increasing trend in the prevalence of PMS during 1996-2011 but correlation between prevalence of PMS and year of study was not significance (p= 0.797).
Interpretation and Conclusions: Considering that different tools have been used in studies and many studies have been designed based on a limited sample, therefore, future research needs to consider the prevalence of PMS in different countries of world.
Prevalence of Premenstrual Syndrome, Meta-regression model, Symptom of Premenstrual Syndrome
Introduction
Today, research on women’s health has greatly improved [1,2]. PMS is a common health problem in women in reproductive age and defined as a collection of emotional symptoms, with or without physical symptoms, related to a woman’s menstruation cycle [3]. PMS is occur during the luteal phase of menses, however, it disappear with menstrual flow. The prevalence of PMS has been reported in 20 to 32 % of premenopausal [4] and 30-40% of the reproductive female population [5].
There are several different symptoms have been associated with PMS [6]. The symptoms are cyclic and recurrent. The symptoms can change in extent and strength during different cycles [7].
Different etiologies have been suggested for the PMS. The abnormal function of hypothalamic-pituitary-adrenal axis (HPA), which leads to defect in adrenal hormone secretion, nutritional defects and environmental factors are the main factors for PMS [8]. The endocrine systems is one of the theories for explaining the physiopathological mechanism of PMS [7].
PMS affects women’s quality of life, economic and social performance. In other study, about 23- 31 % of reproductive aged women experience PMS to a degree that affects their daily lives [9].
PMS can cause mood disorders and its complications [10]. Therefore, during the last 2 decades; several studies have been conducted on various treatment options regarding PMS [11–14].
Due to side effects of PMS, the present study aimed to investigate the prevalence of PMS using meta-analysis method.
Methods
Search strategy
This originally meta-analysis reviewed the world wide prevalence of PMS. We electronically searched the English-language medical literature published between 1996 -2011 using the available databases including Pub Med and Medline. The protocol was designed using widely recommended methods and reported according to PRISMA [15]. Using the medical subject headings (MeSH), we searched “Premenstrual Syndrome”, “Epidemiology of PMS” and “prevalence of Premenstrual Syndrome” including all subheadings.
Study Selection and Data Extraction
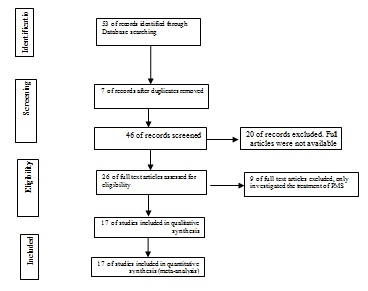
Two researchers independently screened the titles of all recode citations, removing duplicate records and distinguishing potentially relevant studies for inclusion. Abstracts from selected citations were then independently reviewed by two researchers for further relevance, with full text manuscripts retrieved as appropriate. In the disagreement cases, a third consultant acted as an intervener. This search selected 53 abstracts. The following data was extracted from included studies: first author, study population, type of data collection, sampling methods, type of study and main findings. The eligible studies were those which reported the “Premenstrual Syndrome” and “prevalence of Premenstrual Syndrome”. However, studies which included treatment of PMS were excluded. Out of 53 abstracts, 26 papers were categorized as potentially eligible for meta-analysis and systematic review. In the last stage 17 full text articles were used in the review [Table/Fig-1].
Results of the systematic literature search
Statistical Analysis
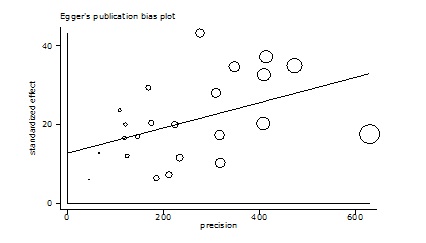
Data synthesis occurred through meta-analyses using the random effect model of Mantel-Haenszel, with available data presented in a Forest plot. Variance for each study was calculated using the binomial distribution formula. The presence of heterogeneity was determined by the chi-square test with a significance level of <0.1 combined with an I2 statistic for estimates of inconsistency within the meta-analyses. The I2 statistic estimates the percent of observed between-study variability due to heterogeneity rather than to chance and ranges from 0 to 100 percent. (Values of 25%, 50% and 75% were considered representing low, medium and high heterogeneity, resp.). For this review we determined that I2 values above 75 percent were indicative of significant heterogeneity warranting analysis with a random effect model as opposed to the fixed effect model to adjust for the observed variability. This heterogeneity was further explored through subgroup analyses and meta-regression. A univariate and multivariate approach were employed to assess the causes of heterogeneity among the selected studies and the Egger test was conducted to examine potential publication bias [Table/Fig-2].
Eggers publication bias plot
Meta-regression was used to examine the relationship between the prevalence of PMS and study’s year and sample size. All analyses were conducted using Stata version 11.2 (Stata Corp LP, College Station, Texas).
Results
During the search of resources a total of 53 articles were found. After exclusion of duplicate, finally 17 papers were selected for analysis [Table/Fig-1]. In total, 18,803 individuals were participants in the studies. The description of studies that met our eligibility criteria are presented in [Table/Fig-3 and 4].
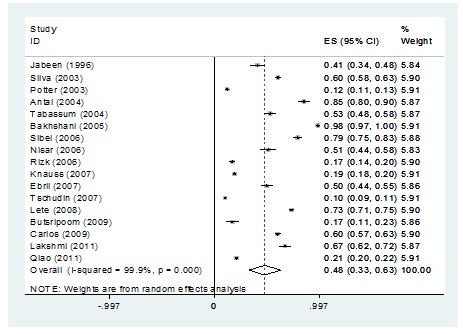
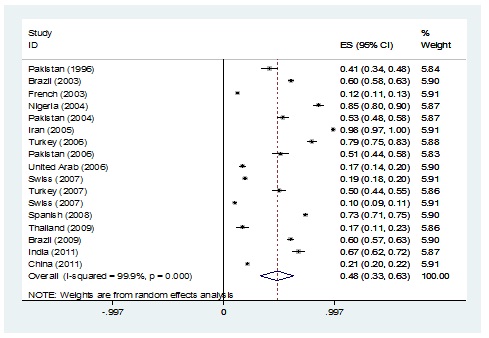
The prevalence of premenstrual syndrome. Squares represented effect estimate of studies with their 95% confidence intervals with size of squares proportional to the weight assigned to the study in the meta-analysis. The diamond represents the overall results and 95% confidence interval of the random effect of the meta-analysis
The description of studies that met our eligibility criteria*Number of participants**Prevalence*** Confidence Interval
| Researcher | Year | n* | locations | p** (%) | CI 95%*** |
|---|
| Jabeen | 1996 | 200 | Pakistan | 41 | 34-48 |
| Silva | 2003 | 1395 | Brazil | 60 | 58-63 |
| Potter | 2003 | 2863 | France | 12 | 10.8-13.2 |
| Antai | 2004 | 200 | Nigeria | 85 | 80.1- 89.9 |
| Tabassum | 2004 | 384 | Pakistan | 53 | 47.8-58.2 |
| Bakhshani | 2005 | 300 | Iran | 98.2 | 96.7-99.7 |
| Sibel | 2006 | 1992 | Turkey | 79 | 74.9-83.1 |
| Nisar | 2006 | 172 | Pakistan | 51 | 43.5-58.5 |
| Rizk | 2006 | 700 | United Arab Emirates | 16.8 | 14-19.6 |
| Knauss | 2007 | 3518 | Switzerland | 19 | 17.7-20.3 |
| Erbil | 2007 | 300 | Turkey | 49.7 | 44-55.4 |
| Tschudin | 2007 | 3913 | Switzerland | 10 | 9.1-10.9 |
| Lete | 2008 | 2018 | Spain | 73 | 70.8-75.2 |
| Butsripoom | 2009 | 161 | Thailand | 16.8 | 10.9-29.7 |
| Carlos | 2009 | 1053 | Brazil | 60 | 57-63 |
| Lakshmi | 2011 | 300 | India | 67 | 61.7-72.3 |
| Qiao | 2011 | 947 | China | 21 | 19.8-22.2 |
| Total | | 18803 | | 47.8 | 32.6-69.9 |
The prevalence of PMS is presented in 17 articles. The pooled of PMS rate is 48% (95% CI: 33- 63). The prevalence of PMS according to continent is presented in [Table/Fig-5]. The prevalence of PMS has been studies in Asia in compared with other continents. [Table/Fig-6] show the prevalence of PMS according to Country. Based the retrieved studies Iran has been the highest prevalence of PMS.
The prevalence of PMS according to continent. Squares represented effect estimate of studies with their 95% confidence intervals with size of squares proportional to the weight assigned to the study in the meta-analysis. The diamond represents the overall results and 95% confidence interval of the random effect of the meta-analysis
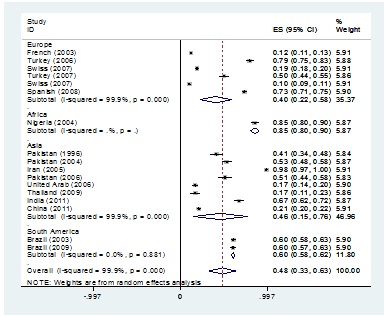
The prevalence of PMS according to Country. Squares represented effect estimate of studies with their 95% confidence intervals with size of squares proportional to the weight assigned to the study in the meta-analysis. The diamond represents the overall results and 95% confidence interval of the random effect of the meta-analysis
Meta-regression scatter plot did indicated a significant correlation between the sample sizes and the prevalence of PMS (p= 0.013) [Table/Fig-7].
Meta-regression plot of the prevalence of PMS based on year of study

However, meta-regression scatter plot showed an increasing trend in the prevalence of PMS during 1996-2011 but correlation between prevalence of PMS and year of study was not significance (p= 0.797) [Table/Fig-8].
Meta-regression scatter plot of the prevalence of PMS based on sample size
Discussion
Main Findings
This study evaluated the prevalence of PMS in different areas in world wide. Based our results, the pooled prevalence of PMS was 47.8% (95% CI: 32.6-62.9). The lowest and highest prevalence were reported in France 12% (95% CI: 11-13) and Iran 98% (95% CI: 97-100) respectively.
Interpretation in Light of Previous Studies
Present study reported the pooled prevalence of PMS was 47.8 percent in world wide. This study is the first systematic review and meta-analysis of PMS. Based on searches in scientific databases, the impact of some factors on treatment of PMS have been studied using a meta-analysis but any studies have been reported the prevalence of PMS [16,17].
Different studies have reported a wide range of PMS in various countries. So that, the PMS rate has been reported 10 percent in Switzerland [18] and 98 percent in Iran [19].
We evaluated the prevalence of PMS according to continent. The result shows the highest and lowest prevalence in Asia and Europe respectively. In subgroups, the lowest frequency of PMS was reported in Switzerland’s study. In this study participated 3913 women aged 15-54. Results showed that 10 percent of all participants experienced some symptoms of PMS [18].
There are several factors affecting on prevalence of PMS such as age [20], aerobic exercise [21,22] and nutrition [23]. The articles that we’ve entered into the meta-analysis, populations studied were different in terms of age, physical activity and nutrition. Therefore, the difference in study population is an effective factor on reported prevalence .The use of various tools of measurement is other main factor for the differences in the reported prevalence. In tree study conducted in Pakistan have used of different tools. Jabeen et al., evaluated the prevalence of PMS among housewives and working women by 4th ed Diagnostic and Statistical manual of mental from American Psychiatric [24]. While Nisar et al., were examined the Prevalence of PMS among the 172 medical students. The researcher applied the daily record of severity of problems (DRSP) includes 21 items grouped into 11 domains and three occupational productivity questions [20]. However, another study conducted in Pakistan (Tabassum et al.,) investigated the medical students, but the tool of data collection was different from other studies [25].
Meta regression scooter plot shows the increase in sample size is associated with a reduced incidence of PMS. This difference is statistically significant. However, the year of study has no effect on increasing the frequency of PMS. Studies reported the prevalence of PMS in 10% of 3913 participants [26] and 12% of 2863 participants [27]. In contrast, studies with low sample size have shown the higher frequency of the PMS [28].
Strengths and Limitations
Our study has several potential Strengths. This study is the first systematic review and meta-analysis of PMS in Iran. Based on searches in scientific databases, the impact of some factors on the prevalence of PMS has been studied using a meta-analysis but any studies have been reported prevalence of PMS.
Our systematic review and meta-analysis study has several limitations. The International databases have not appropriate of quantity (number of papers have been recorded) and quality (tool). This databases do not include all the journals. On the other hand, much of the scientific researches in worldwide are thesis projects. Unfortunately, there is no comprehensive and coherent national database to cover up the thesis projects.
Conclusion
Based our results the global prevalence of PMS is high and about half of women of reproductive age who experience this symptoms. Considering that different tools have been used in studies and many studies have been designed based on a limited sample, therefore, future research needs to consider the prevalence of PMS in different countries of world.
[1]. Direkvand-Moghadam A, Khosravi A, Evaluating Shirazi (Thymus vulgaris) on menstrual pain using verbal multidimensional scoring system (VMS)Afr J Pharm Pharmacol 2012 6(39):2766 [Google Scholar]
[2]. Direkvand-Moghadam A, Khosravi A, The impact of a novel herbal Shirazi Thymus Vulgaris on primary dysmenorrhea in comparison to the classical chemical IbuprofenJ Res Med Sci 2012 17(7):668-70. [Google Scholar]
[3]. Ussher JM, Perz J, PMS as a process of negotiation: women’s experience and management of premenstrual distressPsychol Health 2013 28(8):909-27. [Google Scholar]
[4]. Biggs WS, Demuth RH, Premenstrual syndrome and premenstrual dysphoric disorderAm Fam Physician 2011 84(8):918-24. [Google Scholar]
[5]. Baker LJ, O’Brien PM, Premenstrual syndrome (PMS): a peri-menopausal perspectiveMaturitas 2012 72(2):121-5. [Google Scholar]
[6]. Dickerson LM, Mazyck PJ, Hunter MH, Premenstrual syndromeAm Fam Physician 2003 67(8):1743-52. [Google Scholar]
[7]. Silva CM, Gigante DP, Carret ML, Fassa AG, [Population study of premenstrual syndrome]Rev Saude Publica 2006 40(1):47-56. [Google Scholar]
[8]. Girman A, Lee R, Kligler B, An integrative medicine approach to premenstrual syndromeAm J Obstet Gynecol 2003 188(5 Suppl):S56-65. [Google Scholar]
[9]. Hylan TR, Sundell K, Judge R, The impact of premenstrual symptomatology on functioning and treatment-seeking behavior: experience from the United States, United Kingdom, and FranceJ Womens Health Gend Based Med 1999 8(8):1043-52. [Google Scholar]
[10]. Bowen R, Bowen A, Baetz M, Wagner J, Pierson R, Mood instability in women with premenstrual syndromeJ Obstet Gynaecol Can 2011 33(9):927-34. [Google Scholar]
[11]. McNeil J, Doucet E, Possible factors for altered energy balance across the menstrual cycle: a closer look at the severity of PMS, reward driven behaviors and leptin variationsEur J Obstet Gynecol Reprod Biol 2012 163(1):5-10. [Google Scholar]
[12]. PMS: what it is and what you can do about itAm Fam Physician 2011 84(8):929-30. [Google Scholar]
[13]. Steiner M, Peer M, Palova E, Freeman EW, Macdougall M, Soares CN, The Premenstrual Symptoms Screening Tool revised for adolescents (PSST-A): prevalence of severe PMS and premenstrual dysphoric disorder in adolescentsArch Womens Ment Health 2011 14(1):77-81. [Google Scholar]
[14]. Halbreich U, Selective serotonin reuptake inhibitors and initial oral contraceptives for the treatment of PMDD: effective but not enoughCNS Spectr 2008 13(7):566-72. [Google Scholar]
[15]. Moher D, Liberati A, Tetzlaff J, Altman DG, Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statementJ Clin Epidemiol 2009 62(10):1006-12. [Google Scholar]
[16]. Kleinstauber M, Witthoft M, Hiller W, Cognitive-behavioral and pharmacological interventions for premenstrual syndrome or premenstrual dysphoric disorder: a meta-analysisJ Clin Psychol Med Settings 2012 19(3):308-19. [Google Scholar]
[17]. Shah NR, Jones JB, Aperi J, Shemtov R, Karne A, Borenstein J, Selective serotonin reuptake inhibitors for premenstrual syndrome and premenstrual dysphoric disorder: a meta-analysisObstet Gynecol 2008 111(5):1175-82. [Google Scholar]
[18]. Forrester-Knauss C, Zemp Stutz E, Weiss C, Tschudin S, The interrelation between premenstrual syndrome and major depression: results from a population-based sampleBMC Public Health 2011 11:795 [Google Scholar]
[19]. Bakhshani NM, Mousavi MN, Khodabandeh G, Prevalence and severity of premenstrual symptoms among Iranian female university studentsJ Pak Med Assoc 2009 59(4):205-8. [Google Scholar]
[20]. Nisar N, Zehra N, Haider G, Munir AA, Sohoo NA, Frequency, intensity and impact of premenstrual syndrome in medical studentsJ Coll Physicians Surg Pak 2008 18(8):481-4. [Google Scholar]
[21]. Vishnupriya R, Rajarajeswaram P, Effects of aerobic exercise at different intensities in pre menstrual syndromeJ Obstet Gynaecol India 2011 61(6):675-82. [Google Scholar]
[22]. Ravindran LN, Woods SA, Steiner M, Ravindran AV, Symptom-onset dosing with citalopram in the treatment of premenstrual dysphoric disorder (PMDD): a case seriesArch Womens Ment Health 2007 10(3):125-7. [Google Scholar]
[23]. Sayegh R, Schiff I, Wurtman J, Spiers P, McDermott J, Wurtman R, The effect of a carbohydrate-rich beverage on mood, appetite, and cognitive function in women with premenstrual syndromeObstet Gynecol 1995 86(4 Pt 1):520-8. [Google Scholar]
[24]. Musarrat J, Fouzia G, Frequancy of premenstrual syndrome in working women vs housewives in PishavarJPMI 2007 21(9):92-8. [Google Scholar]
[25]. Tabassum S, Afridi B, Aman Z, Tabassum W, Durrani R, Premenstrual syndrome: frequency and severity in young college girlsJ Pak Med Assoc 2005 55(12):546-9. [Google Scholar]
[26]. Tschudin S, Bertea PC, Zemp E, Prevalence and predictors of premenstrual syndrome and premenstrual dysphoric disorder in a population-based sampleArch Womens Ment Health 2010 13(6):485-94. [Google Scholar]
[27]. Potter J, Bouyer J, Trussell J, Moreau C, Premenstrual syndrome prevalence and fluctuation over time: results from a French population-based surveyJ Womens Health (Larchmt) 2009 18(1):31-9. [Google Scholar]
[28]. Ozturk S, Tanrıverdi D, Erci B, Premenstrual syndrome and management behaviours in TurkeyAustralian Journal of Advanced Nursing 2011 28(3):54-60. [Google Scholar]