PCN is the cornerstone for upper urinary diversion in varied clinical settings, where rapid surgical decompression warranted. Even though it is a vital procedure, it remains technically demanding for both resident and junior urologist. Not surprisingly, urologists trained in percutaneous access during residency are more likely to perform percutaneous procedure as compared to the untrained. Since the description of trocar nephrostomy by Goodwin et al., [1] several direct and wire guided (seldinger) methods of PCN tube placement have been described in the scientific literature. Unfortunately, we are lacking enough technical skills because a step wise method is either not or very poorly elucidated therein. The potential disadvantages of the seldinger technique over direct puncture are the requirement of a guide wire and dilators to an overall increase in procedure cost. Thus, in a developing country like India a technique of direct PCN tube placement may worthily compare to wire guided method. Again, from urological stand point a pelvicaliceal system (PCS) puncture without considering technical aspect not only lead to failure may also endanger the life of the patient. The current study aimed to focus on a new technique of direct PCN tube placement that is easy to acquire, most economical and mathematically precise.
Materials and Methods
Study Design
This was a quasi-experimental study, conducted at Urology Department, RIMS during the period from August 2011 to May 2013. Ethical approval was obtained from the Research and Ethics Committee of the Institute.
Inclusion and Exclusion Criteria
A total number of 176 patients with grade I-IV hydronephrosis requiring PCN tube placement for a variety of disease profile were included in this study, as shown in [Table/Fig-1]. Informed written consent was taken from all the study subjects.
Indications of percutaneous nephrostomy tube placement URS = Ureterorenoscopy; CA: Carcinoma
| Diseases | No of patients |
|---|
| Impacted ureteric calculus | 73 |
| Impacted pelvic calculus | 24 |
| Pyonephrosis | 49 |
| Stricture ureter | 11 |
| Failed DJ stenting | 9 |
| CA Cervix with ureteric infiltration | 2 |
| CA bladder with ureteric infiltration | 2 |
| Post URS ureteric injury | 6 |
Exclusion criteria: Non-dilated renal collecting system; bleeding diathesis; untreated urinary tract infection; pre-operative haemoglobin <10 gm/dl, patient’s unwillingness; severely co morbid patients were excluded categorically.
Pre-procedure Preparation and Steps
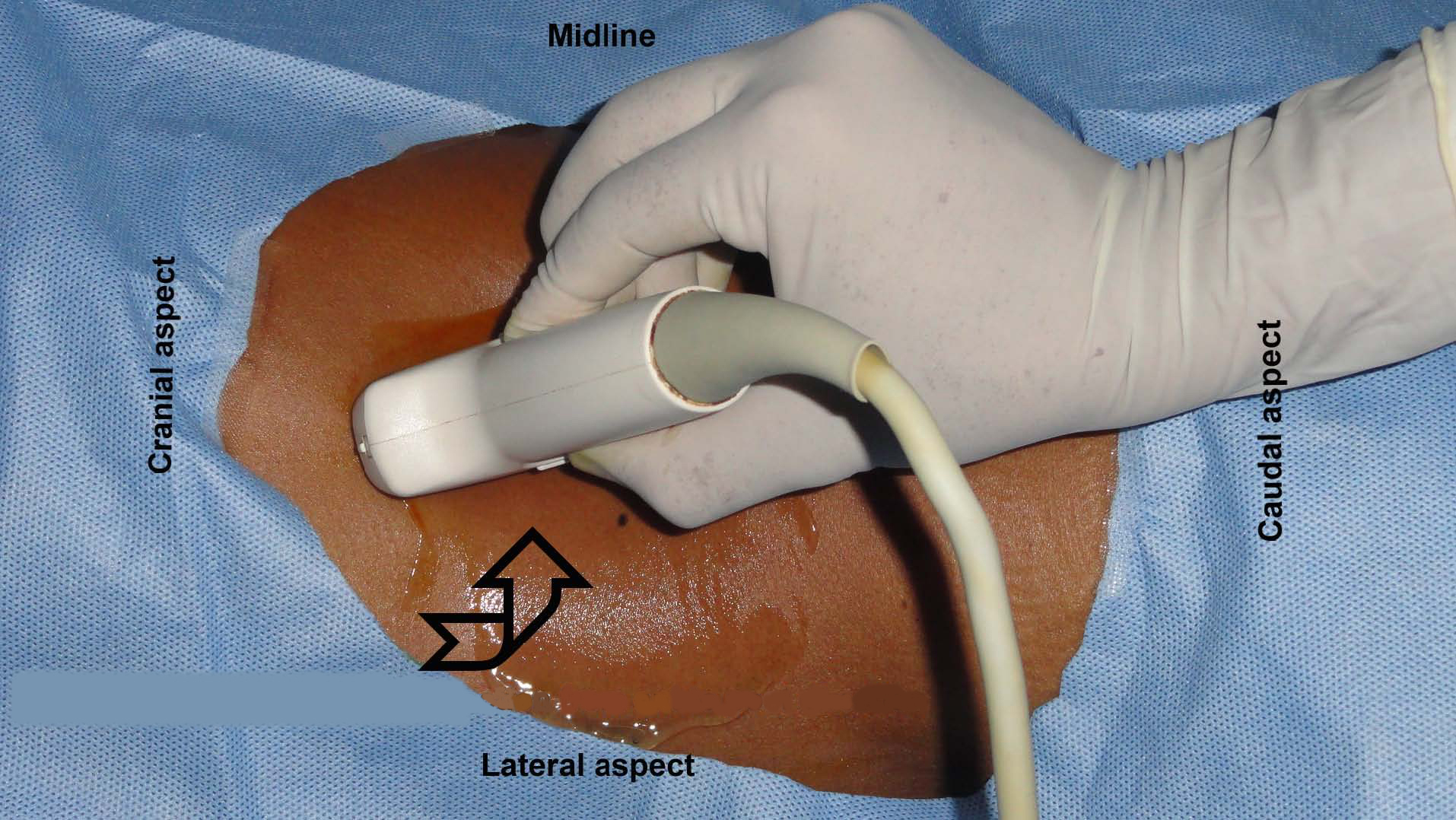
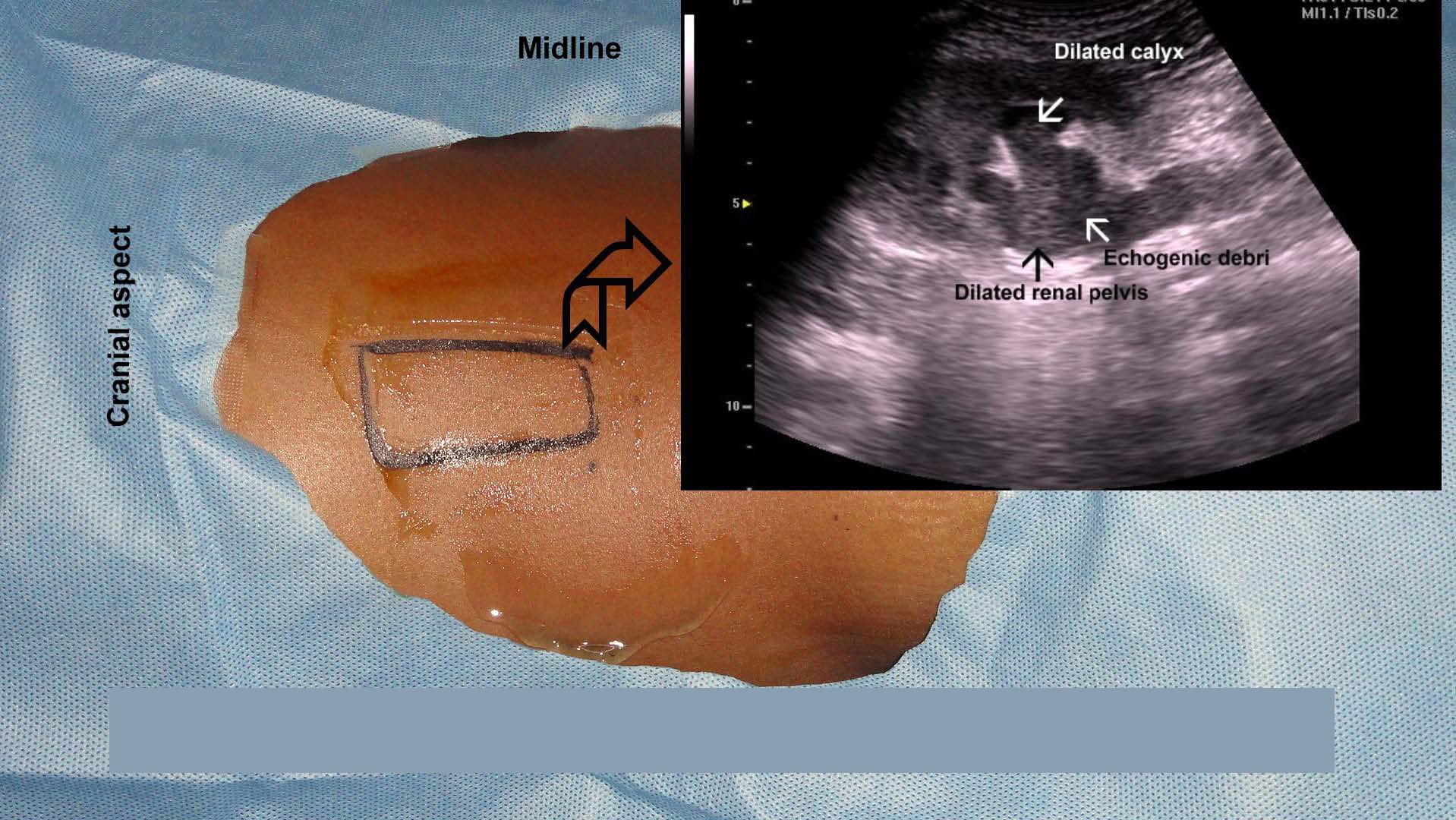
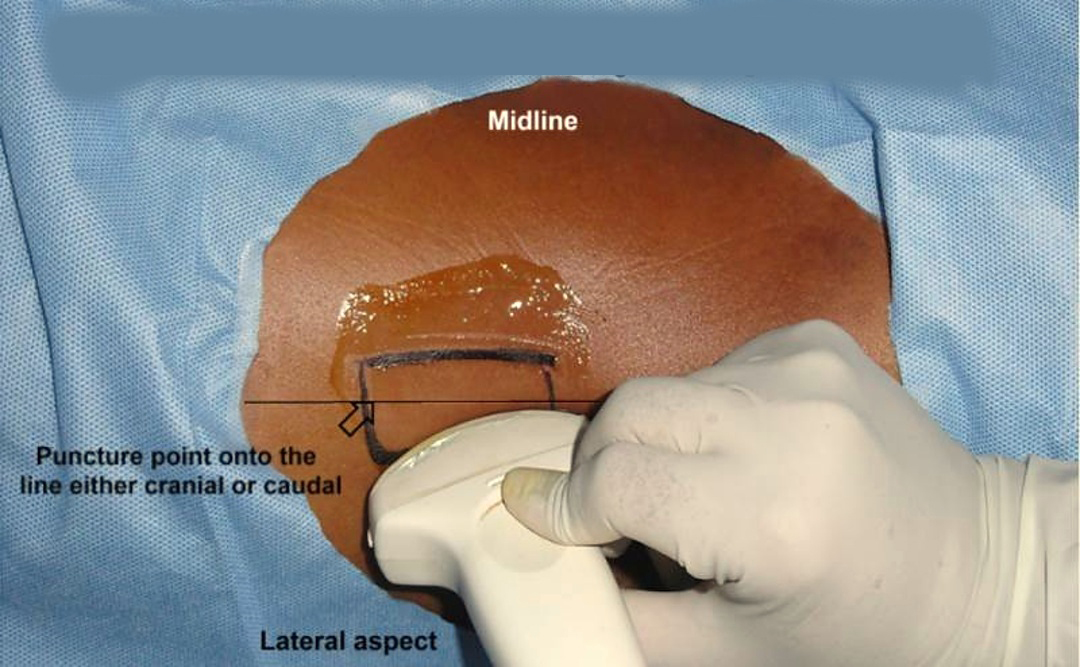
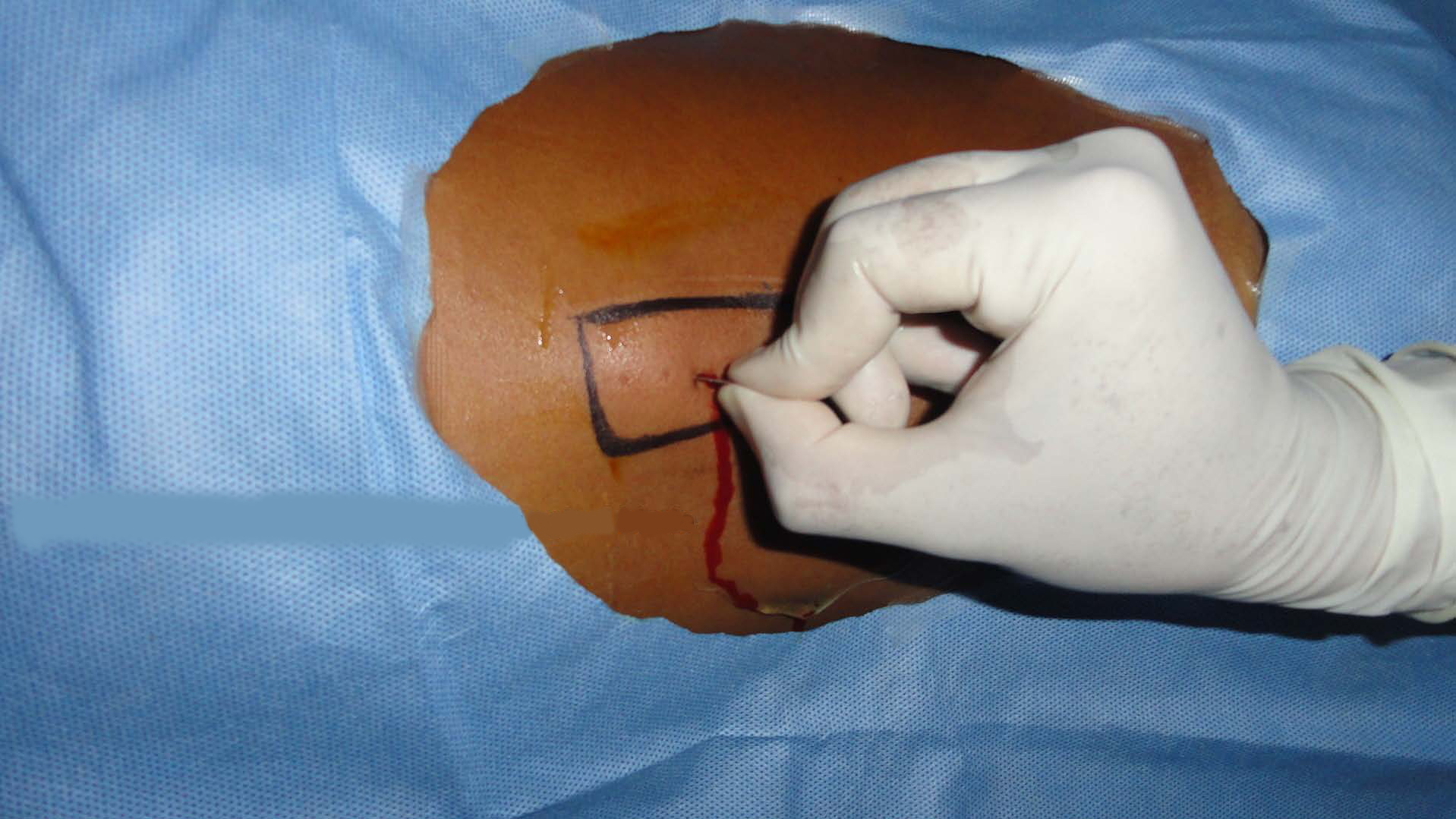
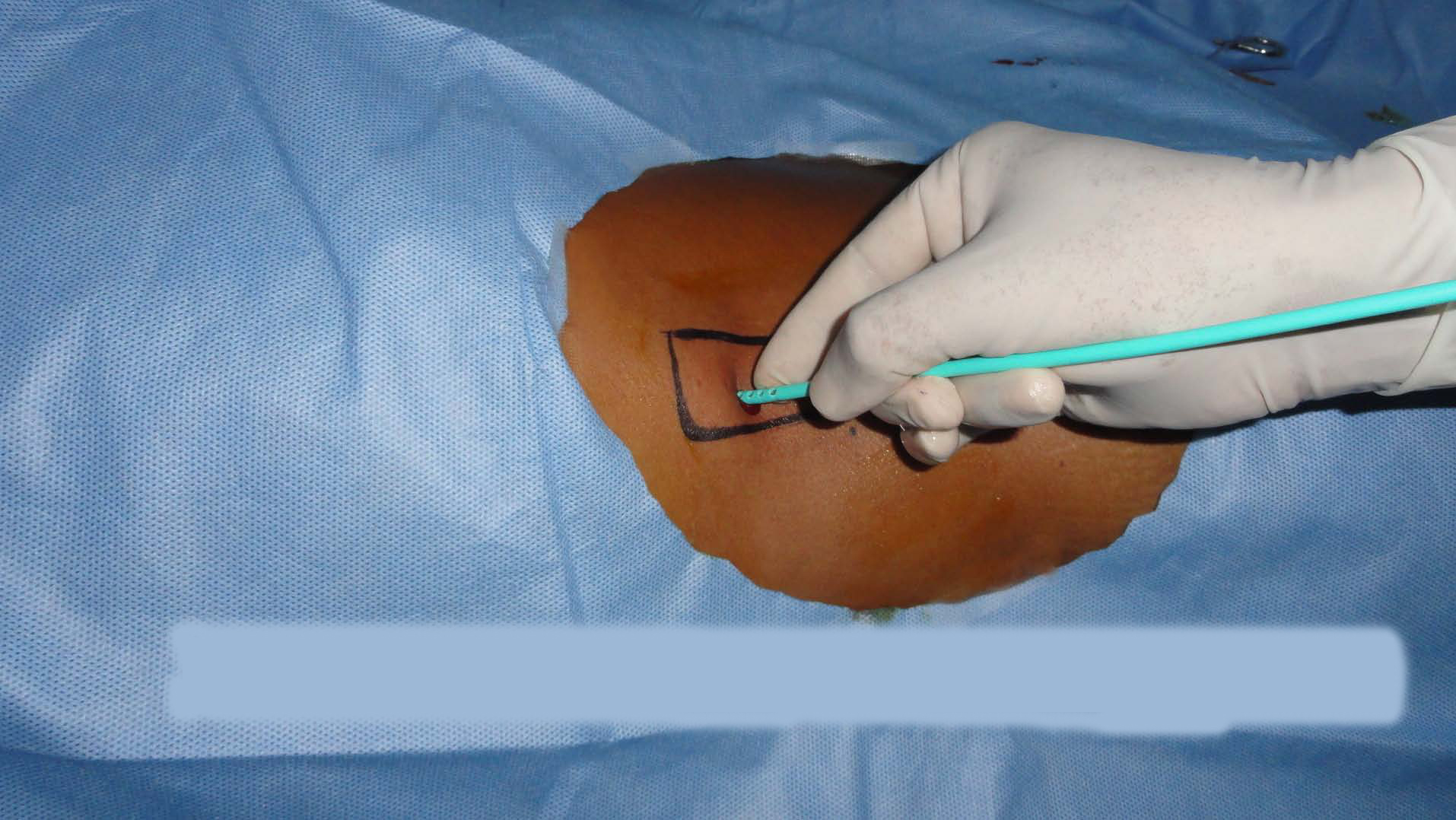
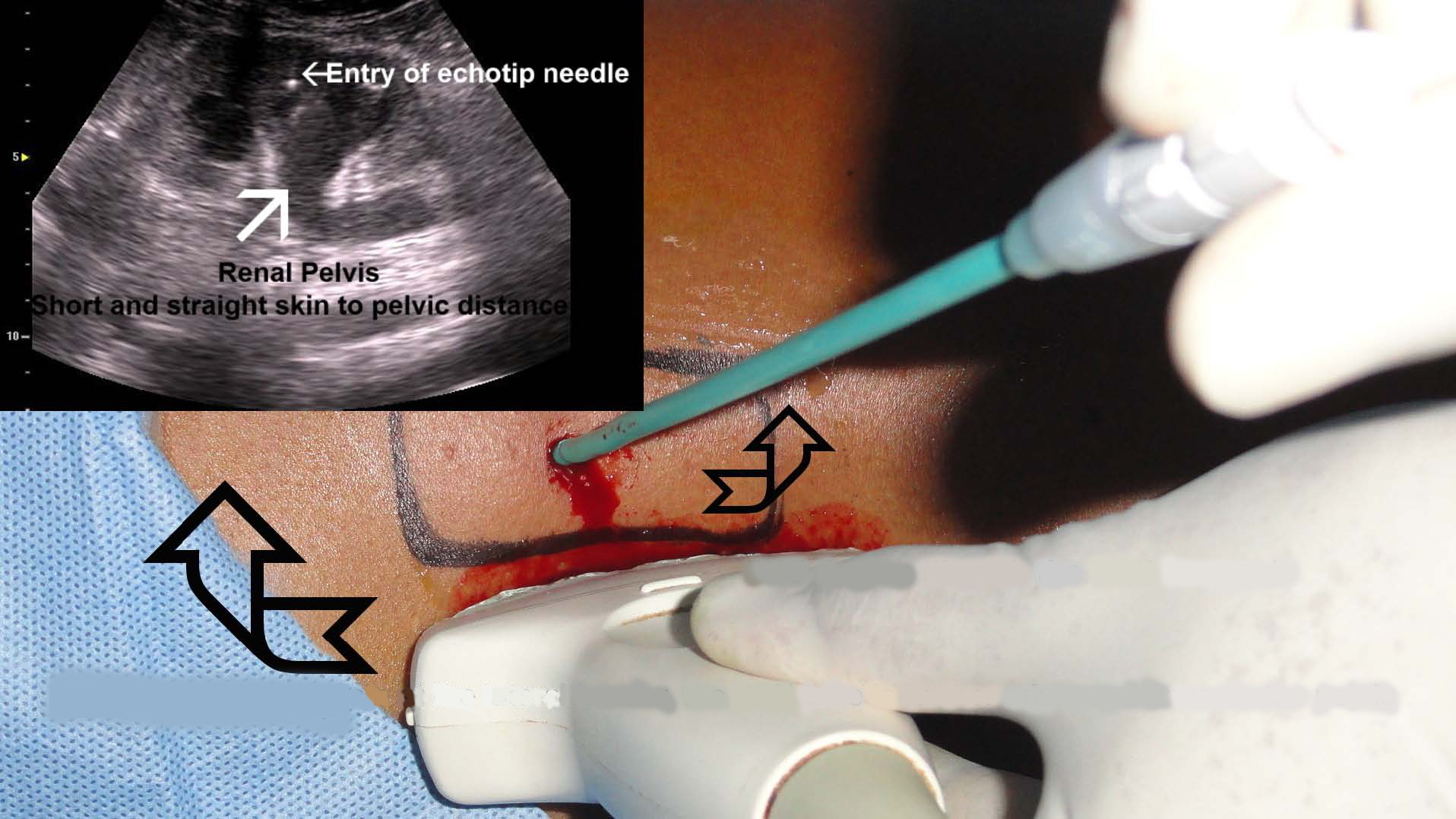
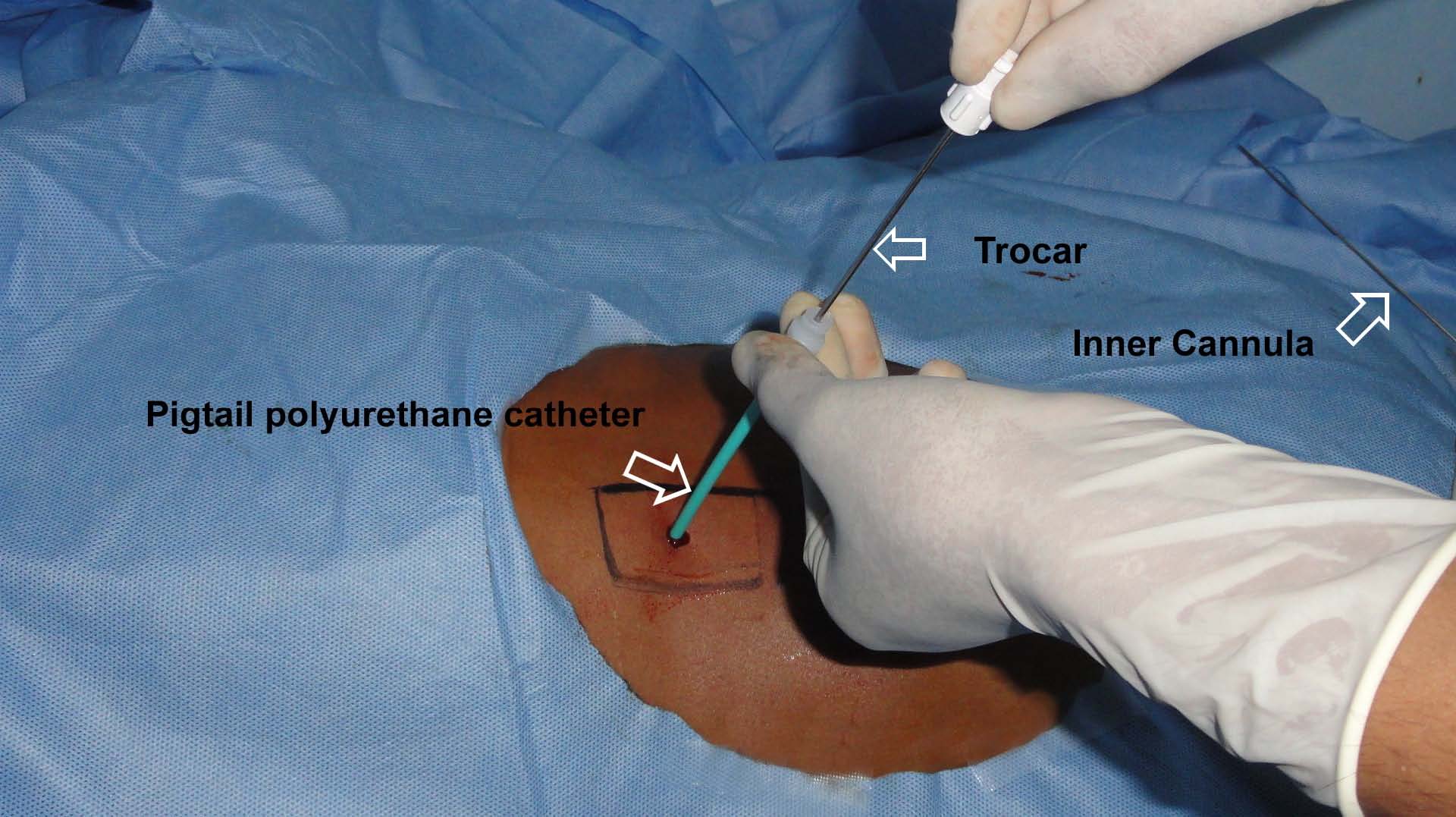
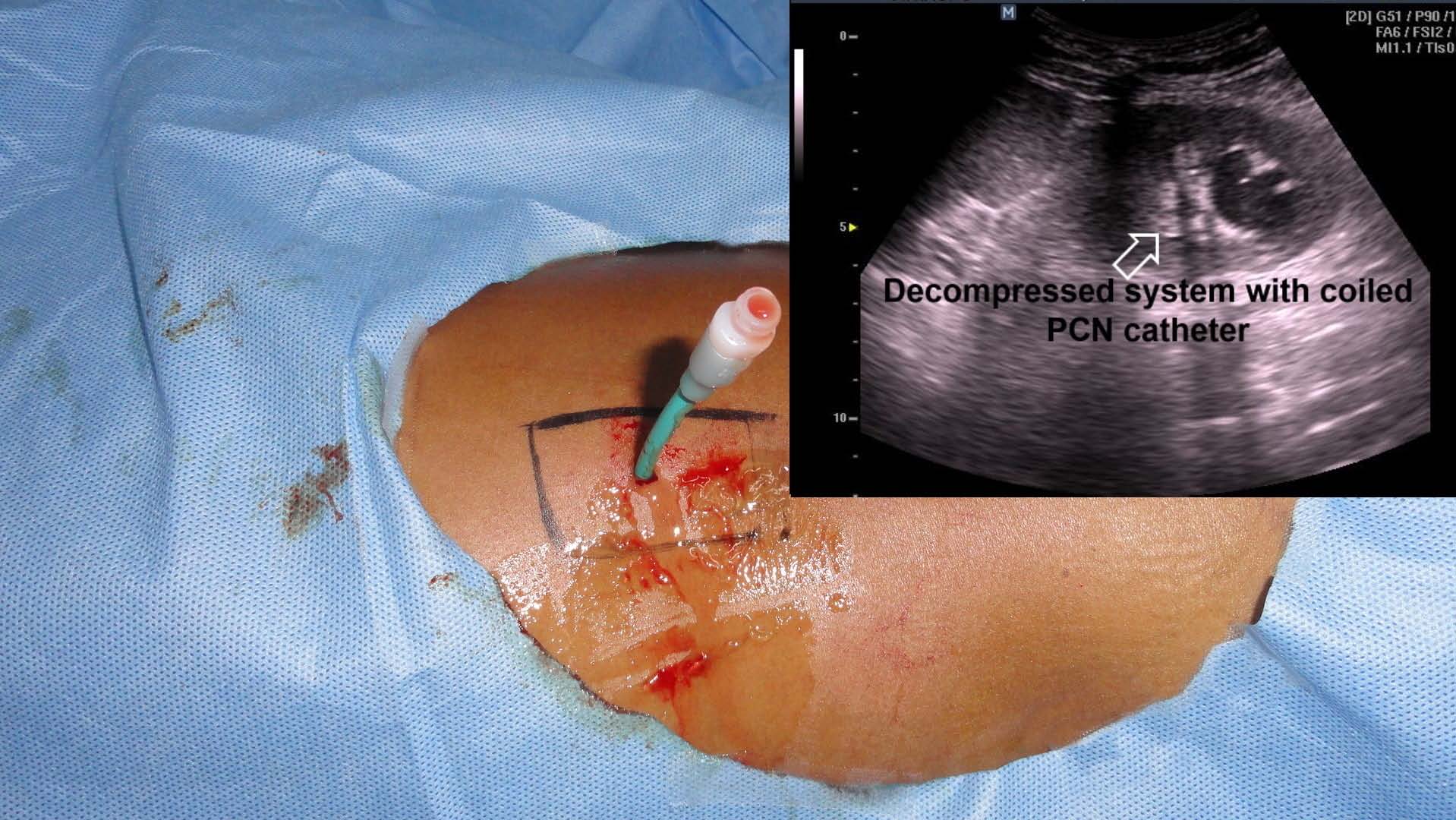
All the eligible patients were given a single oral dose of fluoroquinolone (Tab-prulifloxacin 600 mg) within one hour prior to the procedure. The patients were then placed on the ultrasound table in the prone position and the appropriate side is cleaned and draped. Ultrasonography (USG) was performed using SonoAce X6 Medison C2-8, 5.0 MHz curved array probe. A single urologist has performed all the cases using a 10 or 12-F (based on the absence or presence of pyonephrosis) 22 cm PCN pigtail catheter with echo-tip needle (Bio-Rad Medisys Pvt Ltd). Procedural steps are discussed as. Step 1: USG scans of the affected kidney in longitudinal plane from anterior to posterior direction [Table/Fig-2]. Step 2: A surface area with superior sonographic visibility of dilated renal pelvis (in Grade I HDN) and both renal pelvis and calyx (in Grade II-IV HDN) is chosen and marked [Table/Fig-3]. Step 3: Placing the probe just at the lateral border of the surface area, a puncture point centred on it and directed straight into the renal pelvis with short skin to pelvic distance is chosen [Table/Fig-4]. Step 4: After being anaesthetic infiltration with 10 ml of 2% plain injection lignocaine, the skin, fascia and muscle at the puncture point is incised with a No-11 blade [Table/Fig-5]. Step 5: PCN tube with a needle is blindly inserted for a distance of 3-4 cm that pierces skin, fascia, muscle and fat [Table/Fig-6]. Step 6: The USG probe is again placed at the lateral border of the surface area and the PCN tube is advanced making a 5-15 degree tilt with the USG long axis until the entry of the echo-tip needle into the PCS towards the renal pelvis is visualized [Table/Fig-7]. Visualization of dilated renal pelvis and calyx (if any) at a time during any step (selection of puncture site as well as advancement of needle) is the key to success. It should not happen that only the calyxes are focused but not the renal pelvis. Step 7: After confirming PCN tube entry by removing the inner cannula, the polyurethane pigtail catheter is gradually advanced keeping the trocar steady [Table/Fig-8]. Step 8: Position of PCN pigtail catheter is confirmed by USG with or without saline flush [Table/Fig-9] followed by firm suturing to the skin using silk 1-0 and adhesive strapping.
USG scans in longitudinal plane from anterior to posterior direction
Surface area having superior sonographic visibility of pelvicalyceal system is chosen
Placement of the probe just at the lateral border of the selected surface area, and a puncture point centred on it and directed straight into the renal pelvis with short skin to pelvic distance is chosen
After infiltrating the puncture point with 10 ml of 2% lignocaine, the skin, fascia and muscle at that point are incised with a No-11 blade
PCN tube with a needle is blindly inserted for a distance of 3-4 cm that pierces skin, fascia, muscle and fat
Placing the probe again at the lateral border of the surface area, the PCN tube is advanced making a 5-15 degree tilt with the USG long axis until the entry of the echo-tip needle into the PCS is visualized
Post-confirmation of the PCN tube entry, the polyurethane pigtail catheter is gradually advanced keeping the trocar steady
Ultrasound confirmation of the in situ pigtail catheter with or without saline flush
Data Collection and Statistical Analysis
To evaluate the safety and efficacy of the technique, the details of the various parameters during a pre-procedure, intra-procedure and post-procedure periods were recorded [Table/Fig-10,Table/Fig-11&12]. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS 16.0) for Windows.
Pre-procedural Parameters
| Patient Demographics |
|---|
| Age | Age Group | No. of Patients | Percentage |
|---|
| 10-29 | 13 | 7.40 |
| 30-49 | 90 | 51.13 |
| 50-69 | 56 | 31.81 |
| 70-89 | 17 | 9.66 |
| Male | 77 | 43.75 |
| Female | 99 | 56.25 |
| Normal | 103 | 58.52 |
| Overweight | 68 | 38.64 |
| Obese | 5 | 2.84 |
| Kindney related variables |
| PCN planned | Right side | 62 | 35.22 |
| Left side | 95 | 53.98 |
| Bilateral | 19 | 10.80 |
| Grade I | 23 | 13.07 |
| Grade II | 69 | 39.20 |
| Grade III | 51 | 28.98 |
| Grade IV | 33 | 18.75 |
Intra-procedural Parameters
| Variable | | No. of Patients | Percentage |
|---|
| Procedure related pain | Mild pain (VAS score 0-3) | 106 | 60.22 |
| Moderate pain (VAS score 4-7) | 52 | 29.55 |
| Severe pain (VAS score 8-10) | 18 | 10.23 |
| Nephrostomy tube placement | Successful | 170 | 96.60 |
| Unsuccessful | 6 | 3.40 |
| Evidence of significant bleeding | Collection inside PCS | 5 | 2.84 |
| Perinephric collection | 2 | 1.14 |
| Puncture attempts | Single attempt | 159 | 90.34 |
| >Single attempt | 17 | 9.66 |
| Renal pelvic perforation | 5 | 2.84 |
| Adjacent visceral injury | 0 | 0.00 |
Post-procedural Parameters
| Variables | No. of Patients | Percentage |
|---|
| Gross hematuria | 5 | 2.84 |
| Blood transfusion | 0 | 0.00 |
| Hospital stay | 3 | 1.70 |
| Wound infection | 1 | 0.56 |
| Febrile UTI | 9 | 5.11 |
| Catheter dislodgement after 3 weeks | 7 | 3.98 |
| UTI-Urinary tract infection | | |
Results
The average length of the procedure was 9.07±2.79 (6-15) minutes. Pre-procedural parameters are shown in [Table/Fig-10]. The age range of the patients was from 13 to 76 years with a mean of 40.62 ± 15.98 years. The mean body mass index of the patients was 24.17±4.68 (19-36). The majority of the patients had grade II hydronephrosis (39.20%) followed by grade III (28.98%). Intra-procedural parameters are shown in [Table/Fig-10]. Severe procedure related pain (VAS score 8-10) was observed only in 18 patients (10.23%). Nephrostomy tube placement was successful in 96.60% of cases and only 9.66% required more than single attempt [Table/Fig-11]. There was no evidence of adjacent visceral injury. Complications were few and minor thus required no transfusion in the post-procedural period. Nine patients (5.11%) developed febrile UTI and managed conservatively [Table/Fig-12].
Discussion
Ultrasound guided PCN was first performed by Pedersen JF, [2] and since then a large number of studies on USG guided PCN tube placement have been carried out with a reported success rate of up to 92-94% [3,4]. The standard ‘Seldinger’ technique uses a needle puncture, guide wire insertion followed by serial tract dilatation and nephrostomy tube placement thus overall a lengthy and costly procedure requiring additional manpower. In contrary, the direct PCN tube placement is simple, cheap, less time consuming and effective procedure. Its low cost (approximately 1,200 INR) compared to standard nephrostomy set (approximately 5,000 INR) is particularly suitable for developing countries. Therefore, if we know the technical aspect why not a direct nephrostomy tube placement? Unfortunately, there is no step wise elucidation of this technique. The majority of the urologist and Interventional radiologist uses their own technique of PCN tube placement that may not be easily acquired by trainee and junior urologist. To our knowledge, as the grade of hydronephrosis decreases the puncture difficulty increases. Therefore, we have discussed a technique that certainly follows mathematically precise steps and if followed, we deemed to have successful tube placement. In our case, high success rate (96.60%) is due to our technical precision. Again, locating and puncturing a dilated calyx is straight forward but correct placement of the catheter in a dependent position could be a difficult task. In our present study, renal pelvis directed puncture resulted in tube placement therein. The most important criteria that we learnt from our present exercise is: USG visualization of the renal pelvis (in grade I HDN) and both pelvis and calyx (in grade II-IV HDN) throughout the procedure is key to success. If in any step, only the calyxes are focused but not the renal pelvis then chances of failure is high. In this study, impacted ureteric calculus was found to be most common indication of PCN tube placement followed by pyonephrosis. Evidence of significant bleeding is noticed in seven patients and managed conservatively. Unsuccessful cases were secondary to poor visualization from pelvicalyceal haemorrhage and poor compliance from patient standpoint. The potential complications of the PCN are; sepsis, perirenal hematoma, urinoma formation, perforation of a viscus and pyopneumothorax [5]. Though there was no procedure related mortality in our case, but a figure up to 0.05-0.3% and significant bleeding requiring transfusion or surgical intervention in 1-4% has been reported [6,7]. Our classification of hydronephrosis in grade I-IV was based on Beetz R et al., [8]. Although percutaneous genitourinary intervention is considered clean-contaminated, but according to the Society of Interventional Radiology (SIR) guidelines these are most often contaminated or dirty procedures and routine antibiotic prophylaxis is recommended [9]. The major limitation we feel is the relative unfamiliarity of surgeons with the optimal operative skills of ultrasound.
Conclusion
Ultrasound guided direct PCN tube placement is a reliable, easy and cost effective technique. This procedure is particularly suitable for developing countries like India, where the majority of the patients belongs to low socio-economical status and having inadequate infrastructural facilitity. The technique is mathematically precise and if followed meticulously with all necessary instructions and precautions, the chances of achieving percutaneous access are very high.
Abbreviation: PCN-percutaneous nephrostomy; PCS-pelvicalyceal system; USG-ultrasonography; HDN-hydronephrosis; VAS-visual analogue scale; SIR-society of interventional radiology.