Nosocomial Infections (NI) occur worldwide and affect both developed and developing countries. Infections acquired in health care settings are among the major causes of death and increased morbidity among hospitalized patients. These infections result in substantial morbidity, mortality and increased financial burden. NI are also important public health problems in developing countries as well as in developed countries. The socio-economic impact, i.e., prolongation of hospitalization, mortality and cost, of these infections adversely affects patients and nation’s economic well-being [1,2]. A incidence survey was conducted under the auspices of World Health Organization (WHO) in 55 hospitals of 14 countries representing four WHO Regions (Europe, Eastern Mediterranean, South-East Asia and Western Pacific) showed an average of 8.7% of hospital patients had NI. At any time, over 1.4 million people worldwide suffer from infectious complications acquired in hospital [3]. The highest frequencies of NI were reported from hospitals in the Eastern Mediterranean and South-East Asia Regions (11.8 and 10.0% respectively), with a incidence of 7.7 and 9.0% in the European and Western Pacific Regions respectively [4].
Risk factors for the development of NI in the Surgical Intensive Care Unit (SICU) setting include poor nutritional status, exposure to multiple antibiotics, indwelling central venous catheters, mechanical ventilation and length of Intensive Care Unit stay [5]. The most common resistant gram-positive organisms encountered in the hospital setting are methicillin-resistant Staphylococcus aureus (MRSA) and Vancomycin-Resistant Enterococci (VRE). Among nosocomial gram-negative pathogens, Extended-Spectrum Beta-Lactamase (ESBL)-producing Enterobacteriaceae, multidrug-resistant Pseudomonas aeruginosa, and multidrug-resistant Acinetobacter baumannii are most prevalent.
The present study was carried out to investigate the incidence of NI and type of bacteriological isolates among the patients admitted in the medical and surgical wards of a non-teaching secondary care hospital in northern India.
Materials and Methods
Study Design
This was a cross-sectional hospital based study conducted in a non-teaching secondary care hospital between January 2011 to December 2012.
Study Site
Wards of General Medicine, General Surgery and Orthopaedic departments of the hospital.
Patients
The patients were admitted in the department for various surgical procedures, without evidence of initial infection, were included in the study.
Nosocomial Infection
Patients who had no infection or they had not been in incubation period on the basis of signs and symptoms; at the admission time and had positive culture after third day of admission, were defined as patients with NI in the present study [6].
Data Collection
Pus, blood, urine, sputum and swabs from various lesions if present among study patients was taken after 48 hour of admission and followed till discharge from the hospital.
Strain Identification
Bacterial strain was identified with the help of gram staining and biochemical tests. Mainly, facultative anaerobes and aerobic bacteria such as Staphylococcus aureus, Streptococcus facealis, Bacillus subtilis, E. coli, Klebsiella, Proteus species, Pseudomonas species and Clostridium species was taken into consideration as per guidelines of CDC [7].
Statistical Analysis
The data collected was entered in the Microsoft Excel computer program and checked for any inconsistency. The results are presented in proportions/percentages. The Chi-square test was used to assess the associations. The p-value <0.05 was considered as significant. All the analysis was carried out by using SPSS 16.0 version.
Ethical Consideration
Ethical clearance was taken from the Ethical Committee of the hospital. The consent was taken from each patients included in the study.
Results
A total of 176 patients were included in the study, of which 82 were from Medical and 94 from Surgical ward. [Table/Fig-1] describes the bio-social characteristics of the patients. Overall incidence of NI was found to be 26.1%. The incidence of NI was higher among the patients of medical (28%) ward than surgical (24.5%) ward, however, the difference was statistically insignificant (p=0.58) [Table/Fig-2].
Distribution of patients by bio-social characteristics
| Bio-social characteristics | Medical (n=82) | Surgical (n=94) | Total (n=176) |
|---|
| no. | % | no. | % | no. | % |
|---|
| Age Group | | | | | | |
| <15 | 4 | 4.9 | 4 | 4.3 | 8 | 4.5 |
| 15-25 | 12 | 14.6 | 12 | 22.3 | 33 | 18.8 |
| 26-35 | 15 | 18.3 | 15 | 12.8 | 27 | 15.3 |
| 36-45 | 14 | 17.1 | 14 | 19.1 | 32 | 18.2 |
| 46-55 | 19 | 23.2 | 19 | 11.7 | 30 | 17.0 |
| >55 | 18 | 22.0 | 18 | 29.8 | 46 | 26.1 |
| Sex | | | | | | |
| Male | 45 | 54.9 | 65 | 69.1 | 110 | 62.5 |
| Female | 37 | 45.1 | 29 | 30.9 | 66 | 37.5 |
| Religion | | | | | | |
| Hindu | 74 | 90.2 | 89 | 94.7 | 163 | 92.6 |
| Muslim | 8 | 9.8 | 5 | 5.3 | 13 | 7.4 |
| Cast | | | | | | |
| General | 16 | 19.5 | 18 | 19.1 | 34 | 19.3 |
| Backward | 22 | 26.8 | 23 | 24.5 | 45 | 25.6 |
| Scheduled | 44 | 53.7 | 53 | 56.4 | 97 | 55.1 |
| Education | | | | | | |
| Illiterate | 53 | 64.6 | 57 | 60.6 | 110 | 62.5 |
| < High school | 12 | 14.6 | 16 | 17.0 | 28 | 15.9 |
| High school-Intermediate | 12 | 14.6 | 17 | 18.1 | 29 | 16.5 |
| Graduate+ | 5 | 6.1 | 4 | 4.3 | 9 | 5.1 |
| Occupation | | | | | | |
| Service | 26 | 31.7 | 31 | 33.0 | 57 | 1.7 |
| Professional | 0 | 00 | 3 | 3.2 | 3 | 7.4 |
| Agriculture | 11 | 13.4 | 2 | 2.1 | 13 | 26.7 |
| Housewife | 28 | 34.1 | 19 | 20.2 | 47 | 21.6 |
| Unemployed | 13 | 15.9 | 25 | 26.6 | 38 | 10.2 |
| Labour | 4 | 4.9 | 14 | 14.9 | 18 | 10.2 |
| SES | | | | | | |
| II | 6 | 7.3 | 9 | 9.6 | 15 | 8.5 |
| III | 6 | 7.3 | 9 | 9.6 | 15 | 8.5 |
| IV | 5 | 6.1 | 11 | 11.7 | 16 | 9.1 |
| V | 65 | 79.3 | 65 | 69.1 | 130 | 73.9 |
Prevalence of Nosocomial Infection (NI) in different wards of the hospitals *p=0.58
| Wards | Nosocomial infection |
|---|
| No. screened | No. with NI | % with NI |
|---|
| Medical* | 82 | 23 | 28.0 |
| Surgical* | 94 | 23 | 24.5 |
| Total | 176 | 46 | 26.1 |
Acinetobacter baumannii was isolated in 89.1% patients. The isolation rate of Acinetobacter baumannii was (p=0.15) higher among the patients of medical ward (95.7%) than surgical ward (82.6). Escherichia coli was isolated in 89.1% and no significant difference was observed between medical and surgical wards. Klebsiella pneumoniae was isolated in 50% patients and was almost similar (p=0.37) in medical surgical wards. The isolation rate of Pseudomonos aeruginosa, Enterococcus faecalis, Staphylococcus aureus and Coagulase negative staphylococci were 43.5%, 73.9%, 34.8% and 17.4% respectively. A significant difference was observed in the isolation rate of Enterococcus faecalis (p=0.007) and Coagulase negative staphylococci (p=0.002) between medical and surgical wards [Table/Fig-3].
Distribution of different types of organism among patient’s biological specimen *Multiple responses, 1Between tertiary and secondary care hospitals, *Significant
| Type of hospital/organism* | Nosocomial infection | p-value1 |
|---|
| Medical patient with organism (n=23) | Surgical patient with organism (n=23) | Total patient with organism (n=46) |
|---|
| Enterococcus faecalis | No | 21 | 13 | 34 | 0.007* |
| % | 91.3 | 56.5 | 73.9 |
| Acinetobacter baumannii | No | 22 | 19 | 41 | 0.15 |
| % | 95.7 | 82.6 | 89.1 |
| Escherichia coli | No | 13 | 8 | 21 | 0.13 |
| % | 56.5 | 34.8 | 45.7 |
| Pseudomonos aeruginosa | No | 10 | 10 | 20 | 1.0 |
| % | 43.5 | 43.5 | 43.5 |
| Staphylococcus aureus | No | 9 | 7 | 16 | 0.53 |
| % | 39.1 | 30.4 | 34.8 |
| Klebsiella pneumoniae | No | 10 | 13 | 23 | 0.37 |
| % | 43.5 | 56.5 | 50.0 |
| Coagulase- negative staphylococcus | No | 0 | 8 | 8 | 0.002* |
| % | 0.0 | 34.8 | 17.4 |
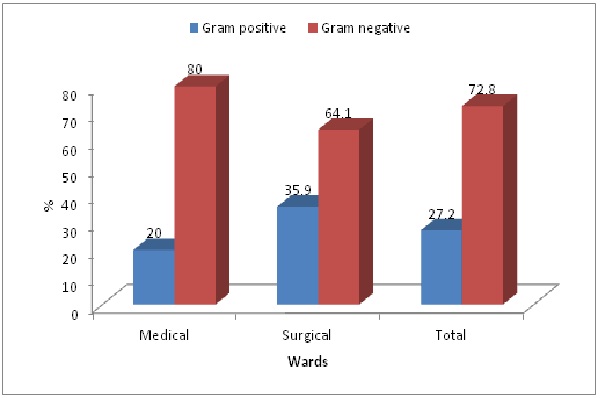
Overall, among the patients who developed NI, 27.2% patient’s bacterial isolates were Gram positive and 72.8% patient’s bacterial isolates were Gram negative. The Gram negative bacterial isolates were lower in surgical ward (64.1%) than medical ward (80%) [Table/Fig-4].
Distribution of Gram positive and Gram negative bacterial isolates among patient’s biological specimen
Discussion
NI are infections acquired during hospital cares which are not present or incubating at admission. Infections occurring more than 48 hours after admission are usually considered nosocomial. Definitions to identify NIs have been developed for specific infection sites (e.g., urinary, pulmonary). These are derived from those published by the Centers for Diseases Control and Prevention (CDC) in the United States of America [8,9] or during international conferences [10] and are used for surveillance of NI. They are based on clinical and biological criteria, and include approximately 50 potential infection sites. NI may also be considered either endemic or epidemic. Endemic infections are most common. Epidemic infections occur during outbreaks, defined as an unusual increase above the baseline of a specific infection or infecting organism.
In the present study, overall incidence of NI was found to be 26.1%. The incidence of NI was higher among the patients of medical (28%) ward than surgical (24.5%) ward, however, the difference was statistically insignificant (p=0.58). Similar finding was seen by Kamat US et al., [11], which is higher than the previous studies in which Infection rate were 16.4% [12] and 13% [13] and lower than following studies where NI rate was 27.4% [14].
Incidence of NI is increasing day by day. The factor that can account for the higher infection rate may be the availability of high number of visitors, lack of knowledge and proper monitoring and setup of the hospital. This slight increase in the incidence of NI in this hospital may paralleled to paying attention to well established processes for decontamination and cleaning of soiled instruments and other items, followed by sterilization and high-level disinfection processes and improving safety in operating rooms and other high-risk areas where the most serious and frequent injuries and exposures to infectious agents occur.
In other studies, the commonest bacterial organisms were Escherichia coli (51.0%), Klebsiella species (19.6%) and Proteus mirabilis (10.0%) [15]. Gram negative bacilli accounts for 194 (54.34%), Klebsiella pneumoniae 60 (31%) was the commonest [16] and Acinetobacter baumannii accounted for 41.8% (n=18) of all the infections [17]. In another study the most common microorganisms were Escherichia coli (64.3%), coagulase negative staphylococci (11.2%) and Klebsiella (8.1%) [18]. In this study, the isolation rate of Pseudomonos aeruginosa, Enterococcus faecalis, Staphylococcus aureus and Coagulase negative staphylococci were 43.5%, 73.9%, 34.8% and 17.4% respectively. These findings are almost in agreement with other studies.
Gram negative bacteria causes thousands of hospital acquired infections each year. It is estimated that approximately 30% of all the hospital acquired infections are caused by Gram negative bacteria, and that they are responsible for approximately 70% of all hospital acquired infections contracted in the Intensive Care Unit [19]. In the present study, Overall, among the patients who developed NI, 27.2% patient’s bacterial isolates were Gram positive and 72.8 percent patient’s bacterial isolates were Gram negative. The Gram negative bacterial isolates were lower in surgical ward (64.1%) than medical ward (80%). Vanitha Rani N et al., [20] reported that in most of the studies, Gram-negative bacilli have taken over the Gram positive organisms, especially in hospital settings and Gram negative bacteria were predominant (58%). Another study reported the incidence of 80.96% for Gram-negative and 18% for Gram-positives [21].
Conclusion
The incidence of NI is increasing in the hospitals, so that the more care has to be taken in the cleaning the wards of the hospitals.