Cardiovascular Disease and Menopause
Rupal Dosi1, Nikita Bhatt2, Priyanki Shah3, Rushad Patell4
1 Professor, Department of Medicine, Medical CollegeBaroda, Gujrat, India.
2 Intern, Department of Medicine, Medical CollegeBaroda, Gujrat, India.
3 Ex-Senior Resident, Department of Medicine, Medical CollegeBaroda, Gujrat, India.
4 Senior Resident, Department of Medicine, Medical CollegeBaroda, Gujrat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rushad Patell, 32 Alka Society, Akota, Vadodara-390020, India.
Phone: 9824048252,
E-mail: rushadpatell@gmail.com
Aim: The aim of the study was to study the abnormalities in the cardiovascular profile in postmenopausal Indian women and to compare the same with the cardiovascular profile of pre menopausal Indian women belonging to the same age group; taken as controls. The goal was to throw some light on the cardiovascular risk in postmenopausal women of the Indian population as this population is thought to be at higher risk than their western counterparts and significant studies of the same kind in this population have been few.
Materials and Methods: A cross-sectional comparative study on 100 women who were either postmenopausal or premenopausal and were between the age group of 40 to 55 years was carried out over a period of ten months at our hospital. The variations in the cardiovascular profile between both groups were studied. All the women were subjected to a detailed history, thorough examination, investigations and imaging studies.
Results: The evaluation revealed that Coronary Artery Disease (CAD), hypertension, abnormal Body Mass Index (BMI) and abnormal Waist Hip Ratio (WHR) were significantly higher in the postmenopausal group as compared to the premenopausal group. The post menopausal women had significantly higher prevalence of abnormal lipid profiles as compared to their premenopausal counterparts. The postmenopausal women with a normal lipid profile also had increased prevalence of CAD and SAHT, which emphasizes the non-lipid cardiovascular benefits of estrogen.
Conclusion: Thus, we can conclude that cardiovascular disease was more common in postmenopausal women of age group 40-55 years as compared to those not yet achieved menopause in a population of western Indian women. And this risk was significantly associated with central obesity, an abnormal lipid profile and the postmenopausal state in itself.
Menopause, Coronary artery disease, Estrogen
Introduction
The incidence and prevalence of CAD in developing countries is increasing alarmingly [1,2]. Major differences have been demonstrated in studies on western populations in the incidence of CAD in males and pre menopausal females even when the other risk factors are matched in both the groups [3]. Hormonal factors like the cardio protective role of estrogen are thought to be responsible [4–6]. Hypertension and central obesity too play a contributory role [7–9]. Cardiovascular risk has been shown to manifest at a lower level of adiposity and abdominal obesity in Asian Indians as compared to their Western counterparts [10,11]. The data on the cardiovascular risk in postmenopausal women in Asian Indians is extremely limited. An attempt was made to find a relation between the menopausal state and increased CAD, Systemic Arterial Hypertension and abnormal lipid profile in our study of one hundred women at a tertiary hospital in western India.
Materials and Methods
This cross-sectional comparative study on 100 women who were either postmenopausal or premenopausal (50 women in each group) and were between the age group of 40 to 55 years was carried out over a period of ten months at our Hospital. The aim of the study was to study the abnormalities in the cardiovascular profile in postmenopausal women and to compare the same with the cardiovascular profile of pre-menopausal women belonging to the same age group; taken as controls. The variations in the cardiovascular profile between both groups were studied. The inclusion criterion was postmenopausal women aged 40-55 years as cases and premenopausal women of the same age group as controls. This nullified any effect of senile changes affecting the cardiovascular diseases and lipid profile abnormalities in post and premenopausal women. Women with premature/surgical menopause, renal disease, liver disease, endocrine disorders including diabetes mellitus, alcohol consumption, smokers and those with collagen vascular disease as well as women taking any form of hormone replacement therapy were excluded.
Thus, 50 cases and 50 controls satisfying the inclusion criteria were subjected to a detailed questionnaire (with special focus on cardiovascular risk factors and health) which included past history with reference to the duration, investigation and treatment of cardiac disease or hypertension, a history of major diseases like diabetes mellitus, tuberculosis, renal, liver diseases and other endocrine diseases. Family history of diabetes mellitus, hypertension, tuberculosis, and ischemic heart disease including angina, MI and sudden cardiac death was enquired into. A detailed menstrual history (to help rule out any premature or surgical menopause) and an obstetric history was noted; especially for any form of contraception used including oral contraceptive pills and their compositions. A thorough general examination was performed and anthropometric measurements of BMI, WHR, vitals and presence of signs of CCF and atherosclerosis were taken note of. A detailed system wise clinical examination with special attention to the cardiovascular system was done. The subjects underwent routine investigations like complete blood count, urinalysis and biochemical investigations like fasting and 2 hours post-glucose, blood glucose levels, blood urea, serum creatinine, lipid profile (total cholesterol, LDL-C, HDL-C, VLDL-C and triglyceride). Chest X-ray, electrocardiography and echocardiography were done in each of the subjects.
Results
The control group consists of 50 age matched premenopausal women and the case group has 50 postmenopausal women.
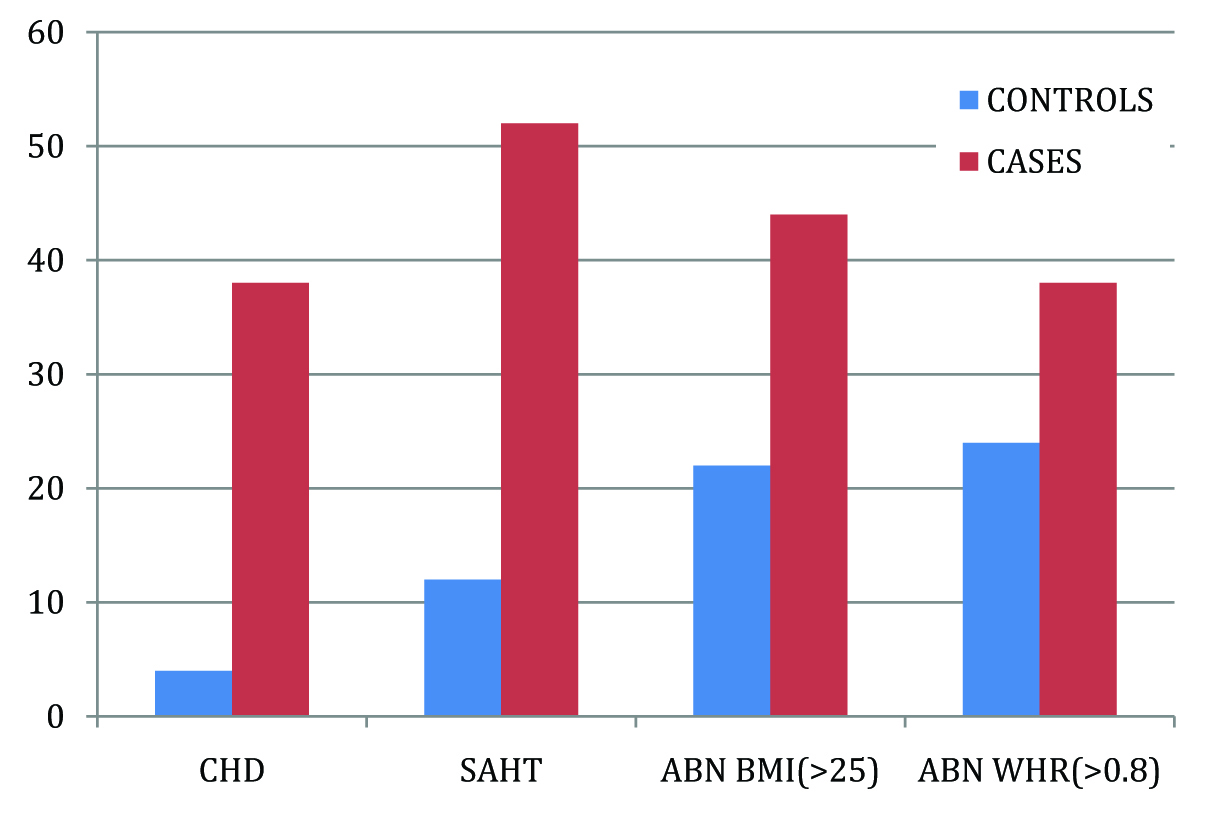
The evaluation revealed the CAD prevalence was 38% (19/50) among postmenopausal women and 4% (2/50) in the control population making the difference statistically significant (p<0.001). Hypertension was present in 52% (26/50) of the cases and 12% (6/50) of the controls, thus the prevalence of hypertension in postmenopausal women was highly significant (p <0.001). The general examination showed 44% (22/50) of the postmenopausal women to have high BMI and 22% (11/50) of the premenopausal women to have high BMI. Thus the prevalence of abnormal BMI in postmenopausal women is statistically significant (p <0.05). The WHR was abnormal in 38% cases and 24% controls (p =0.08) [Table/Fig-1].
Prevelance of CHD, SAHT, abnormal BMI and abnromal WHR in cases and controls of the Study
Abnormalities in the lipid profile as revealed by the investigations are outlined in the [Table/Fig-2].
Prevalence of cholesterol abnormalities (total cholesterol >200 mg/dL), LDL-C abnormalities (>130 mg/dL) and HDL-C abnormalities (<60 mg/dL)
| Cholesterol abnormalities | LDL-C abnormalities | HDL-C abnormalities |
|---|
| 200 to 240 mg/dL | >240 mg/dL | Total | 130 to 160 mg/dL | >160 mg/dL | Total | <40 mg/dL | 40-60 mg/dL | Total |
|---|
| No. | % | No. | % | No. | % | No. | % | No. | % | No. | % | No. | % | No. | % | No. | % |
| Case (n=50) | 10 | 20 | 20 | 40 | 30 | 60 | 11 | 22 | 20 | 40 | 31 | 62 | 13 | 26 | 29 | 58 | 42 | 84 |
| Control (n=50) | 19 | 38 | 07 | 14 | 26 | 52 | 9 | 18 | 16 | 32 | 25 | 50 | 9 | 18 | 30 | 60 | 39 | 78 |
| p-value | <0.05 | <0.01 | <0.05 | >0.05 | >0.05 | <0.05 | >0.05 | >0.05 | |
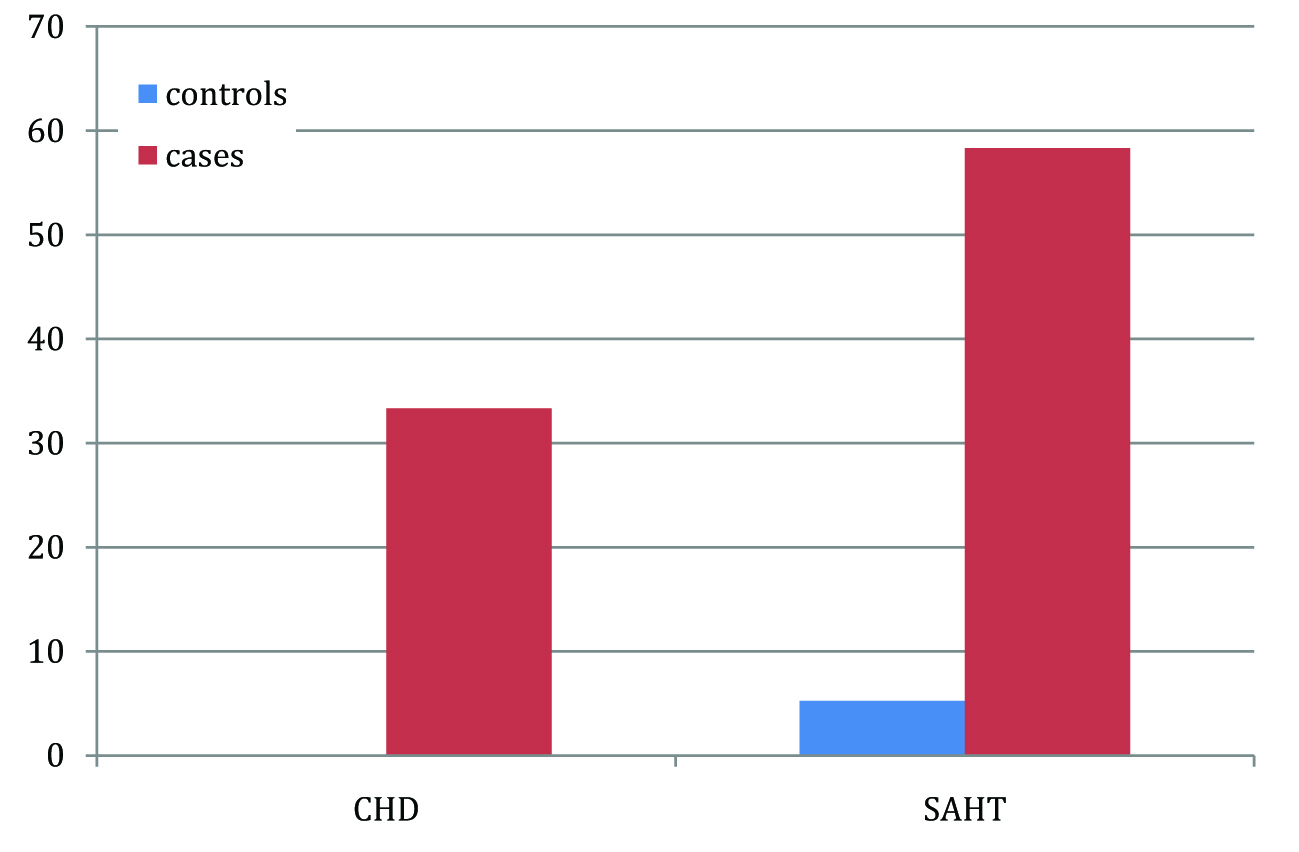
The analysis of prevalence of CAD and SAHT in women with normal lipid profile showed that hypertension was present in 58.33% (7/12) of postmenopausal women while 5.26%(1/19) of premenopausal women had hypertension. CAD prevalence in postmenopausal women with normal lipid profile was 33.33% (4/12) whereas it was 0 in the premenopausal age group. Thus, the difference in prevalence for CAD and Hypertension in pre and postmenopausal women with normal lipid profile was found to be highly significant (p <0.001); [Table/Fig-3].
Prevalence of CAD and SAHT in women with normal lipid profile
Discussion
Menopause, permanent cessation of menstruation following loss of ovarian activity, has considerable impact on social, reproductive, physical and psychological health. Women in India are prone to an earlier menopause [12–14] and all its implications on their health at an earlier age than their counterparts in the industrialized world.Estrogen has protective effects on the cardiovascular system due to which there is an increase in the prevalence of cardiovascular diseases in postmenopausal women [6] [Table/Fig-4]. Estrogen also has a favorable effect on body fat distribution and improvement in the insulin sensitivity [15]. Cardiovascular disease is one of the leading causes of death in women [16,17]. The incidence of myocardial infarction in women, although lower than in men, increases dramatically after menopause, which can be attributed mainly to the lack of estrogen and its direct and indirect cardio-protective effects.
Cardiovascular Effects Of Estrogen

Yamamoto A et al., [18] and Tchernof A et al., [19] demonstrated an increased prevalence of CAD in postmenopausal women. Trémollières FA et al, has similarly found increased prevalence of CAD up to 36% in postmenopausal women [20]. Moreover studies have also shown an increased prevalence of hypertension in this group [21]. Thus, our findings of increased prevalence of CAD and SAHT in postmenopausal women are consistent with these studies done in western populations.
Our findings with regards to a comparison of the lipid profiles between the two groups are also comparable to studies done in industrialized nations. Trémollières FA et al, have found 30.6% of postmenopausal women had an increased total cholesterol and LDL cholesterol compared to only 20.4% of premenopausal women (p<0.0005) [20]. Moreover 16.1% of postmenopausal women had an abnormally low HDL-C as compared to 13.3% of pre menopausal women [20]. However this difference was not significant. Other workers in other parts of the world reported similar findings [22,23].
Similar to our findings of higher prevalence of central obesity in postmenopausal women Tchernof A et al., [19] have also found higher prevalence of central obesity in postmenopausal women. Central obesity is now a well-established to risk factor in itself for CAD [24].
We found that postmenopausal women with a normal lipid profile also had increased prevalence of CAD and SAHT, which emphasizes the non- lipid cardiovascular benefits of estrogen. This can be attributed to the direct protective mechanism of estrogen for the vasculature involving inhibition of smooth muscle proliferation, vasodilation and protection of endothelium [6,25].
The use of estrogen and progesterone as a replacement therapy in postmenopausal women is currently limited to the management of severe vasomotor symptoms and bone disease especially in women with premature menopause [26,27] based on the findings of the Women’s Health Initiative (WHI) [28]. However evidence from more recent studies may argue that the jury is still out on the final verdict on hormone replacement therapy [29] and we may be underusing a powerful tool against a major source of morbidity and mortality in a cohort of patients that are rapidly growing in number.
Conclusion
Fifty post and premenopausal women were studied. The aim of this study was to compare the presence of coronary heart disease and hypertension as well as the risk factors associated with cardiovascular disease in postmenopausal women with similar age matched premenopausal controls in an Asian Indian population. From the results of the study we can conclude that CAD and SAHT were more common in postmenopausal women as compared to premenopausal women. Lipid profile abnormalities were more prevalent in postmenopausal women. A higher prevalence on central obesity was noted in postmenopausal women. The prevalence of CAD and SAHT was more in postmenopausal women with normal lipid profiles as compared to their premenopausal counterparts. Thus, we can conclude that cardiovascular disease in women of age group 40-55 years was significantly associated with central obesity, an abnormal lipid profile and the postmenopausal state in itself in a population of western Indian women.
[1]. Reddy K. Srinath, Yusuf Salim, Emerging epidemic of cardiovascular disease in developing countriesCirculation 1998 97:596-601. [Google Scholar]
[2]. Celermajer DS, Chow CK, Marijon E, Anstey NM, Woo KS, Cardiovascular disease in the developing world: prevalences, patterns, and the potential of early disease detectionJ Am Coll Cardiol 2012 60(14):1207-16. [Google Scholar]
[3]. Crawford SL, Johanner CB, The epidemiology of cardiovascular disease in postmenopausal womenClinical Endocr and Metabol 1999 :1803-06. [Google Scholar]
[4]. Skafar Debra F, Rui Xu, Juan Morales, Jeffrey Ram, James R Sowers, Female sex hormones and cardiovascular disease in womenJournal of Clin Endocr Metabol 1997 82(12):3913-18. [Google Scholar]
[5]. Campos H, Walsh BW, Judge H, Sacks FM, Effect of estrogen on very low density lipoprotein and low density lipoprotein subclass metabolism in postmenopausal womenJournal of Clin Endocr. Metabolism 1997 82:3955-63. [Google Scholar]
[6]. Mendelsohn ME, Karas RH, The protective effects of estrogen on cardiovascular systemNew England Journal of Medicine 1999 (340):1801-11. [Google Scholar]
[7]. Trémollières FA, Pouilles JM, Cauneille C, Ribot C, Coronary heart disease risk factors and menopause: a study in 1684 French womenAtherosclerosis 1999 142(2):415-23. [Google Scholar]
[8]. Jouyandeh Z, Nayebzadeh F, Qorbani M, Asadi M, Metabolic syndrome and menopauseJ Diabetes Metab Disord 2013 12(1) [Google Scholar]
[9]. Marjani A, Moghasemi S, The metabolic syndrome among postmenopausalwomen in GorganInt J Endocrinol 2012 :953627 [Google Scholar]
[10]. Mohan V, Rao GHR, Type 2 Diabetes in South Asains 2007 1st edNew DelhiSouth Asian Society on Atherosclerosis and Thrombosis [Google Scholar]
[11]. Misra A, Khurana L, The metabolic syndrome in South Asians: Epidemiology, clinical correlates and possible solutionsInternational Diabetes Monitor 2009 21:92-101. [Google Scholar]
[12]. Bagga A, Age and symptomatology of Menopause: A case studyObstet Gynaecol Today 2004 10:660-6. [Google Scholar]
[13]. Singh M, Early age of natural menopause in India, a biological marker for early preventive health programsClimacteric 2012 15(6):581-86. [Google Scholar]
[14]. Willett W, Stampfer MJ, Bain C, Lipnick R, Speizer FE, Rosner B, Cigarette smoking, relative weight and menopauseAm J Epidemiology 1983 117:651 [Google Scholar]
[15]. Effects of estrogen or estrogen/progestin regiments on heart disease risk factors in postmenopausal women. The postmenopausal estrogen/progestin interventions (PEPI). Trial the writing group for PEPI trialJAMA 1995 273:199 [Google Scholar]
[16]. Papadopoulou SA, Kaski JC, Ischemic heart Disease in the Aging WomanBest Practice & Research Clinical Obstetrics & Gynaecology 25 March 2013 [Google Scholar]
[17]. Roger VL, Jacobsen SJ, Pellikka PA, Miller TD, Bailey KR, Gersh BJ, Gender differences in use of stress lasting and coronary disease mortality: A population based study in Olmsted country, MinnesotaJ Am Coll Cardiol 1998 32:345 [Google Scholar]
[18]. Yamamoto A, Horibe H, Mabuchi H, Kita T, Matsuzawa Y, Saito Y, Analysis of Serum lipid levels in Japanese men and women according to B.M.I Increase in risk of atherosclerosis in postmenopausal women. Research group on serum surveyAtherosclerosis 1999 143(1):55-73. [Google Scholar]
[19]. Tchernof A, Calles-Escandon J, Sites CK, Poehlman ET, Menopause, central body fatness and insulin resistance. Effects of hormone replacement therapyCoronary A disease 1998 9(8):503-11. [Google Scholar]
[20]. Trémollières FA, Pouilles JM, Cauneille C, Ribot C, Coronary heart disease risk factors and menopause: a study in 1684 French womenAtherosclerosis 1999 142(2):415-23. [Google Scholar]
[21]. Perry AC, Applegate EB, Allison ML, Miller PC, Signorile JF, Relation between anthropometric measures of fat distribution and cardiovascular risk factors in overweight pre and post-menopausal womenAmerican J Clin Nutr 1997 66(4):829-35. [Google Scholar]
[22]. Matthews KA, Kuller LH, Sutton-Tyrrell K, Chang YF, Changes in cardiovascular risk factors during premenopausal and postmenopausal and carotid artery atherosclerosis in healthy womenStroke 2001 32(5):1104-11. [Google Scholar]
[23]. de Aloysio D, Gambacciani M, Meschia M, Pansini F, Bacchi Modena A, Bolis PF, The effect of menopause on blood lipid and lipoprotein levels the Icarus study groupAtherosclerosis 1999 147(1):147-53. [Google Scholar]
[24]. Robert HEckel, The Metabolic Syndrome. In Longo DL, Kasper MD, Jameson JL, Fauci AS, Hauser SL, Localzo J, editorsHarrison’s Principles of Internal Medicine 2012 Vol. 218th edNew YorkMcGraw Hill:3040-45. [Google Scholar]
[25]. De Ziegler D, Cardiovascular physiology of ovarian hormonesSchweizRundsch Med 1997. Jan. 28 86(5):138-44. [Google Scholar]
[26]. Taylor HS, Manson JE, Update in hormone therapy use in menopauseJ Clin Endocrinol Metab 2011 96:255 [Google Scholar]
[27]. Main C, Knight B, Moxham T, Gabriel Sanchez R, Sanchez Gomez LM, Roqué I, Hormone therapy for preventing cardiovascular disease in post-menopausal womenCochrane Database Syst Rev 2013 :4 [Google Scholar]
[28]. Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trialJAMA 2002 288:321 [Google Scholar]
[29]. Schierbeck LL, Rejnmark L, Tofteng CL, Stilgren L, Eiken P, Mosekilde L, Effect of hormone replacement therapy on cardiovascular events in recently postmenopausal women: randomised trialBMJ 2012 345:e6409 [Google Scholar]