Pneumococcal Infections at a Rural Tertiary Care Hospital: A Seven Year Study on Isolation Rate, Clinical Spectrum and Antibiogram
Anitha Deva1, Subba Rama Prasad2, Beena Parvangada Madappa3, Krishnappa Junjegowda4, Raghavendra Prasad Narayanaswamy Bachu5
1 Tutor, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
2 Professor, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
3 Professor and Head, Department of Microbiology, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
4 Associate Professor, Department of Paediatrics, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
5 Professor and Head, Department of General Medicine, Sri Devaraj Urs Medical College, Kolar, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Prasad S.R., Professor, Department of Microbiology, Sri Devaraj Urs Medical College, Tamaka, Kolar-563101, Karnataka, India.
Phone: 07760259210,
E-mail: subbaramaprasad@gmail.com
Background: Invasive pneumococcal infections such as pneumonia, bacteraemia and meningitis are severe and often fatal. In recent years, pneumococcal resistance to penicillin has been a problem in many countries. We, in this retrospective study analysed the case records of culture proven pneumococcal infections seen over a period of seven at a rural tertiary health care centre in Karnataka and studied the antibiotic resistance pattern of the isolates.
Aims: To know the spectrum of illness caused by pneumococci, isolation rate from the specimens and the antibiogram of pneumococci isolated from patients admitted at a rural tertiary care centre.
Methods: The laboratory records were searched for isolations of pneumococci from different samples from 2006-2012. The isolation rate from different specimens was calculated. The case records of the patients whose samples yielded pneumococci were analysed for demographic and clinical details. The antibiotic sensitivity pattern of the isolates was studied.
Results: During the study period of seven years, pneumococci were isolated from 34 (0.092%) of the 37,070 samples processed. Samples of blood, pleural fluid, sputum and CSF obtained from patients with bacteraemia, community acquired pneumonia and meningitis accounted for 31(91.2%) of the 34 pneumococcal isolations. All the isolates (100%) were sensitive to penicillin; they were also sensitive to erythromycin, chloramphenicol, vancomycin and linezolid. The sensitivity to gentamicin, ciprofloxacin and tetracycline varied from 79.4% to 88.2%. Only 50% of the isolates were sensitive to cotrimoxazole. Among the patients who yielded pneumococci, 21(61.76%) were children. The patients were treated with a combination of β-lactam and aminoglycoside antibiotics. Eighteen (90%) of the 20 patients, whose outcome was known, recovered completely.
Conclusion: Majority of the isolations of pneumococci over a period of seven were made from samples obtained from patients with invasive pneumococcal diseases such as community acquired pneumonia, bacteraemia and meningitis. Children contributed 2/3rd of the pneumococcal isolations. All the isolates were sensitive to penicillin, erythromycin, chloramphenicol, vancomycin and linezolid, where as 50% of the isolates were resistant to cotrimoxazole. Ninety percent of the patients recovered completely after appropriate antibiotic therapy.
Streptococcus pneumoniae, Antibiogram of pneumococci, Isolation rate, Spectrum of Pneumococcal disease
Introduction
Pneumococcus (Streptococcus pneumoniae) causes a spectrum of illness ranging from mild otitis media to fatal meningitis and is the most common cause of community acquired pneumonia [1,2]. Extremes of age and certain underlying illnesses like asplenia, sickle cell anaemia, diabetes are risk factors for Pneumococcal disease [1].
Pneumococcal disease causes morbidity and mortality throughout the world. World Health Organization, in 2005, estimated that annually world over 1.6 million deaths occurred due to pneumococcal infections and among them were 0.7 to 1 million children below 5 years [3]. In India, during 2005,136,000 children were estimated to have died of pneumococcal disease; more than 50% of this mortality is thought to have occurred in central and eastern states of India: Madhya Pradesh, Uttar Pradesh, Rajasthan and Bihar [4]. Further, as pneumococcal resistance to penicillin is being reported more and more in the recent years, it becomes important to monitor the antibiotic susceptibility pattern of the isolates [2,5,6] and develop efficient vaccines.
There are very few reports on the pneumococcal disease, its clinical spectrum and antibiotic susceptibility pattern of pneumococci from India. In this study, we report the isolation rate, associated clinical conditions and antibiotic susceptibility pattern of pneumococcal isolates made over a period of seven years (2006-2012) at a tertiary care centre at Kolar, Karnataka, India.
Materials and Methods
Laboratory records of patients admitted from 2006 through 2012 at R.L. Jalappa hospital, Kolar, Karnataka, were searched for the isolation of Streptococcus pneumoniae (S. pneumoniae) from samples received at the microbiology laboratory such as sputum, blood, pleural fluid, cerebrospinal fluid, peritoneal fluid, pus, conjunctival and ear swabs. All the samples processed were considered for the study. Ethical clearance from the Institutional Ethics committee was obtained before the start of the study. Identification of S. pneumoniae was done by standard methods [7] and antibiotic sensitivity pattern was determined by Kirby-Bauer disc diffusion method using the following antibiotic discs obtained from Hi-Media, Mumbai: Penicillin-G (10 units), Erythromycin (15 mcg), Chloramphenicol (30 mcg), Vancomycin (30 mcg), Linezolid (30 mcg), Tetracycline (30 mcg), Ciprofloxacin (5 mcg), Gentamicin (10 mcg) and Cotrimoxazole (25 mcg). Clinical details of patients from whom S.pneumoniae was isolated, was obtained by reviewing hospital records. The data is presented as frequencies, in tables with percentages, and in the bar chart.
Results
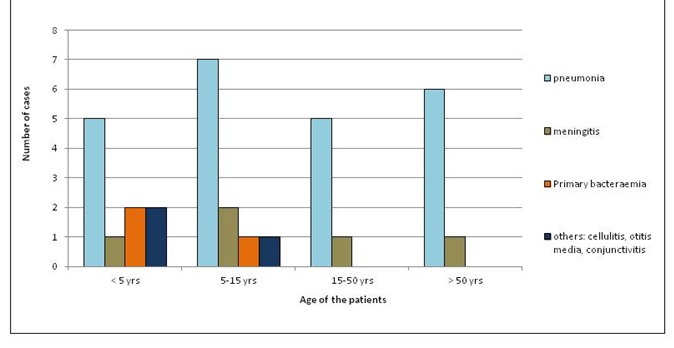
During the period of study, pneumococci were isolated from 34 patients. Twenty one (61.76%) were children and 13(38.24%) were adults. Twenty five (73.5%) were males and 9(26.5%) were females. The different clinical syndromes in which pneumococcus was isolated is presented in [Table/Fig-1]. Both in adults and children, pneumonia and meningitis were the most common conditions from which pneumococcal isolations were made. However, conditions such as primary bacteraemia, conjunctivitis, otitis media and cellulitis were also associated with pneumococcal isolations, but this was only among children.
Clinical conditions coused by S. pneumoniae in different age groups
The isolation rate of pneumococci from different samples is presented in [Table/Fig-2]. S. pneumoniae was isolated from 34 of a total of 37,070 samples. This accounted for an isolation rate of 0.092%. The isolation rate of pneumococci in different samples varied widely from 0.012% to 10% depending upon the type of sample. Among the 34 isolates of pneumococci,14(41.17%) were from body fluids (9 from pleural fluid and 5 from CSF). There were 9(26.47%) isolates from blood: 6(66.66%) of them were obtained from patients who had concurrent pneumonia (secondary bacteraemia) and 3(33.33%) of them from patients with no particular foci of infection (primary bacteraemia). Most of the patients were treated with β-lactam and aminoglycoside antibiotics. The information on the outcome of illness was available only in 20 patients. Out of 20 patients, 18(90%) patients recovered completely after treatment with appropriate antibiotics and 2 (10%) patients expired; one of them died of meningitis and the other of septicaemia.
Isolation of S. pneumoniae from different clinical samples during 2006-2012
| Sample | No. tested | No. of isolations (%) | Clinical diagnosis |
|---|
| Blood | 18,822 | 9 (0.05%) | Bacteraemia |
| Pus | 8194 | 1 (0.012%) | Cellulitis left leg |
| Sputum | 5412 | 8 (0.14%) | Pneumonia |
| Fluids | 4364 | 14 (0.32%) 9-pleural fluid 5-CSF | Pleural effusion and meningitis |
| Conjunctival swab | 10 | 1 (10%) | Conjunctivitis |
| Ear swab | 278 | 1 (0.35%) | Ear discharge |
| Total | 37,080 | 34 (0.092%) | |
Antibiogram of the isolates of pneumococci is presented in [Table/Fig-3]. All the isolates (100%) were sensitive to penicillin, erythromycin, chloramphenicol, vancomycin and linezolid. Sensitivity to gentamicin, ciprofloxacin and tetracycline varied from 79.4% to 88.2%. Only 50% of the isolates were sensitive to cotrimoxazole.
Antibiotic susceptibility pattern of the isolates (n=34)
| Antibiotic | No. sensitive (%) |
|---|
| Penicillin | 34(100) |
| Erythromycin | 34(100) |
| Chloramphenicol | 34(100) |
| Vancomycin | 34(100) |
| Linezolid | 34(100) |
| Tetracycline | 30(88.2) |
| Ciprofloxacin | 29(85.3) |
| Gentamicin | 27(79.4) |
| Cotrimoxazole | 17(50) |
Preponderance of a single pattern of resistance was not noticed. Resistance to gentamicin, ciprofloxacin, tetracycline, or cotrimoxazole, was observed among the isolates singly or in combination throughout the study period. However, isolates sensitive to all the antibiotics tested were also encountered throughout the study period. An isolate which was resistant to all the 4 antibiotics: gentamicin, ciprofloxacin, tetracycline and cotrimoxazole, was encountered for the first time in the year 2012.
Discussion
In this retrospective analysis of pneumococcal infections, as proven by isolation of pneumococci that occurred over aperiod of seven years at a rural tertiary care hospital at Kolar, Karnataka (in southern India), we found that over the years, S. pneumoniae was isolated from 0.092% of the specimens from patients suspected of pneumococcal infections. This means, there were nine pneumococcal isolations for every 10,000 relevant samples processed. The isolation rate from clinical specimens is a reflection of incidence of the disease. This isolation rate is less when compared to other studies in India. A multicentre study from India reported an isolation rate of 2.5% [2]. Another study exclusively conducted among children admitted to hospitals at Bangalore, India, documented an isolation rate of 1.14% [8]. Prior administration of antibiotics is known to reduce the isolation rate of pneumococci [9]. This factor might also have influenced our isolation rate. We could not assess the impact of prior antibiotic administration on the isolation rate, as history of prior antibiotic administration was not consistently recorded in the case sheets. Antigen detection methods will increase the detection rate; however antibiotic sensitivity pattern cannot be determined.
Pneumococcal infections are more common in children and our data also supports this observation [10]. Pneumococci colonize and establish themselves as commensals in the upper respiratory tract of children. When predisposing factors are found, the organisms overgrow and cause conditions such as sinusitis, conjunctivitis and otitis media. The organisms become blood borne when there is a loss of integrity in the mucous membrane of the upper respiratory tract and may cause meningitis and other clinical syndromes which are more common in children [1]. Pneumococcal bacteraemia can be primary or secondary being associated with pneumonia or other focal lesions in the body [1,7]. In our study, 9 patients had bacteraemia. Among them, 3 had primary bacteraemia and 6 were secondary bacteraemic cases.
All the isolates of pneumococci (100%) in our study were sensitive to penicillin, erythromycin, chloramphenicol, vancomycin and linezolid. Resistance to penicillin among pneumococci isolated in India appears to be low; it has been reported to vary between 1 to12% according to different studies [6,11–13]. This contrasts with the situation in neighbouring Southeast Asian countries and Srilanka where the resistance to penicillin is as high as 40 to 70% among the isolates [14]. The low prevalence of penicillin resistance among pneumococci in India is thought to be due to the absence of dissemination of penicillin resistant clones [15]. Our isolates tested were from a rural population and this could explain the high susceptibility to penicillin. However, as we have not determined the minimum inhibitory concentration (MIC) to penicillin, we might have missed the organisms with intermediate resistance to penicillin [2]. As India presents a unique situation with respect to resistance to penicillin, vigilance is required; the spread of the resistant clones from neighbouring countries may pose therapeutic difficulties in treating the patients.
Other studies from India have also recorded low prevalence of pneumococcal resistance to erythromycin and chloramphenicol similar to our observations [6,11,12]. We found that 50% of our isolates were resistant to cotrimoxazole, 20% were resistant to gentamicin, 15% to ciprofloxacin and 12% to tetracycline. Similar prevalence of resistance to these antibiotics has been reported in other studies in India [2,6].
In the recent years, there has been considerable effort in preventing invasive pneumococcal infections using polyvalent pneumococcal vaccines. A conjugate pneumococcal vaccine with a cocktail of antigens from 13 serotypes of pneumococci is available in India [16] and is indicated for use among children, elderly and patients with special risk. We may hope that the burden of invasive pneumococcal infections will be drastically reduced with active vaccination.
Conclusion
The present study from a hospital situated in a rural area of Karnataka shows that pneumococcal infections are relatively less common. Over a period of seven years, 34 isolations of pneumococci were made from patients’ samples. Infections were more common among children than adults. All the strains isolated were sensitive to penicillin as well as to erythromycin, chloramphenicol, vancomycin and linezolid. The resistance pattern to gentamicin, ciprofloxacin and cotrimoxazole were similar to that reported from other studies in India.
[1]. Mandell GL, Bennett JE, Dolin R, Mandell, Douglas and Bennett’s Principles and Practice of Infectious Diseases 2010 7th edPhiladelphiaElsevier Health Sciences [Google Scholar]
[2]. Invasive Bacterial Infection surveillance (IBIS) group and International clinical epidemiology network (INCLEN)Prospective multicentre hospital surveillance of Streptococcus pneumoniae disease in IndiaLancet 1999 353:1216-21. [Google Scholar]
[3]. World Health Organization (WHO)Pneumococcal conjugate vaccine for childhood immunization—WHO position paperWkly Epidemiol Rec 2007 82:93-104. [Google Scholar]
[4]. Johnson HL, Bassani DG, Perin J, Levine OS, Cherian T, O’brien KL. Burden of childhood mortality caused by Streptococcus pneumoniae in India. (Internet) 2012 (cited 2013 Dec 4) available from :http://www.jhsph.edu/research/centers-and-institutes/ivac/resources/isppd8/H_Johnson Burden_of_Child_Mortality_by_Strep_Pneumo_in_India.pdf [Google Scholar]
[5]. Legori M, Special article on Streptococcus pneumoniaeJ Acad Clin Microbiol 2006 8:27-29. [Google Scholar]
[6]. Chawla K, Gurung B, Mukhopadhyay C, Bairy I, Reporting Emerging Resistance of Streptococcus pneumoniae from IndiaJ Glob Infect Dis 2010 2:10-14. [Google Scholar]
[7]. Forbes BA, Sahm DF, Weissfeld AS, Bailey and Scott’s Diagnostic Microbiology 2007 12th edSt.LouisMosby [Google Scholar]
[8]. Shah AS, Nisarga R, Ravikumar KL, Hubler R, Herrera G, Kilgore PE, Establishment of population-based surveillance for invasive pneumococcal disease in Bangalore, IndiaIndian J Med Sci 2009 63:498-507. [Google Scholar]
[9]. Mortensen EM, Restrepo MI, Pugh JA, Anzueto A. Impact of prior out patient antibiotic use on mortality for community acquired pneumonia: a retrospective cohort study. BMC Res Notes (Internet) 2008, (cited 2013 Dec 6) 1:120 doi: 10.1186/1756-0500-1-120. Available from: www.biomedcentral.com/1756-0500/1/120/ [Google Scholar]
[10]. Cornick JE, Everett DB, Broughton C, Denis BB, Banda DL, Carrol ED, Invasive streptococcus pneumonia in children, Malawi, 2004-2006Emerg Infect Dis 2011 17:1107-09. [Google Scholar]
[11]. Veeraraghavan B, Thomas K, Penicillin resistant Streptococcus pneumoniae in India: Effects of new clinical laboratory standards institute break point and implicationsIndian J Med Microbiol 2011 29:317-18. [Google Scholar]
[12]. Thomas K, Kesavan LM, Veeraraghavan B, Jasmine S, Jude J, Shubankar M, Invasive pneumococcal disease associated with high case fatality in IndiaJ Clin Epidemiol 2013 16:36-43. [Google Scholar]
[13]. Kanungo R, D’Lima D, Rajalakshmi B, Badrinath KS, Emerging antibiotic resistant pneumococci in invasive infections in south India: Need for monitoringIndian J Pharmacol 2002 34:38-43. [Google Scholar]
[14]. Song JH, Jung SI, Ko KS, Kim NY, Son JS, Chang HH, High prevalence of antimicrobial resistance among clinical Streptococcus pneumoniae isolates in Asia (an ANSORP study)Antimicrob Agents Chemother 2004 48:2101-07. [Google Scholar]
[15]. Balaji V, Thomas K, Joshi HH, Beall B, Increasing invasive disease due to penicillin resistant S. pneumoniae in IndiaIndian J Med Sci 2008 62:492-95. [Google Scholar]
[16]. Amdekar YK, Lalwani SK, Bavdekar A, Balasubramanian S, Chhatwal J, Bhat SR, Immunogenicity and safety of a 13-valent pneumococcal conjugate vaccine in healthy infants and toddlers given with routine vaccines in IndiaPaediatr Infect Dis J 2013 32:509-16. [Google Scholar]