In the past decade, pulmonary veins have been known to play an important role as the triggering focus of the electrical activity in atrial fibrillation [1]. Earlier, it was considered that the variations in the number and course of pulmonary veins were rare and they were confined only to few case reports [2]. Recently, however, it has been found that variations in pulmonary venous anatomy were seen in 36% of patients [3] and that they were one of the aetiologies for ectopic heart beats [4]. This greater than expected variability in pulmonary venous anatomy could substantially alter success rates of radiofrequency ablation, as ectopic foci could go untreated in variant veins. Increasingly, selective radiofrequency ablations of these arrythmogenic foci are being performed, to treat patients with refractory atrial fibrillation [5]. The successful treatment of atrial fibrillation by radiofrequency ablation of the ectopic foci can be made possible only by having accurate knowledge on the normal pulmonary venous anatomy and its measurement. Thus, the present study was done to find out the variations in the number of right and left pulmonary veins which drained into the left atrium.
Materials and Methods
The present study was done on 50 formalin fixed hearts which were obtained from the Department of Anatomy. Left atria of these hearts were studied from external aspect, for the variations in the number of pulmonary veins which drained into it. Left atrium were opened by making a midline incision along the whole length of its posterior wall and the number of pulmonary ostia which opened into the left atrium were identified and documented.
Results
Thirty-four heart specimens (68%) had normal four pulmonary veins, two from each lung which extended to the left atrium and opened into it via two separate pulmonary ostia, on either side. In 16 (32%) out of 50 specimens, variations in the number of pulmonary veins and the pulmonary ostia were observed either on one side or on both sides of the left atrium.
Following variations were recorded in our study: Seven specimens (14%) had a single pulmonary vein with a single ostium on the right side and two pulmonary veins on left side of the left atrium. Six specimens (12%) had three pulmonary veins with three ostia on the right side and two veins on the left side. Two specimens (4%) showed a single pulmonary vein and an ostium on the left side of the left atrium. The remaining 2% of the hearts presented with four separate pulmonary veins with four ostia, along with single left side pulmonary veins opening into the left atrium.
Overall, in our study, the most common variation which was observed in the number of pulmonary veins on right side was a single pulmonary vein (14%), followed by three veins in 12% specimens, a normal pattern of two veins in 4% specimens, and four pulmonary veins in 2% of specimens. In contrast to the right side, left side showed no such variants, except a single left pulmonary vein which drained into the left atrium in 50% of specimens and rest of the specimens showed a normal pattern of drainage [Table/Fig-1].
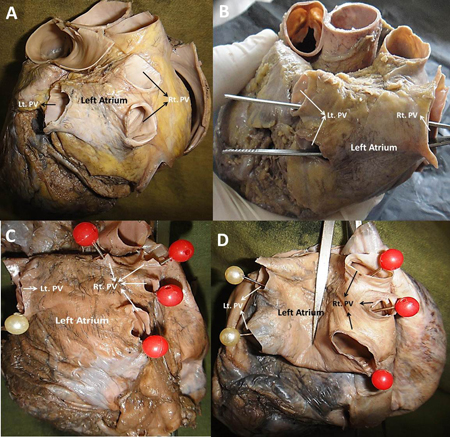
Representative photographs to show the variations in the pulmonary veins opening into the left atrium. A. Left atrium with 2 pulmonary veins in right side (Rt.PV) and one on the left side (Lt. PV). B. Left atrium with one large right pulmonary vein and two left veins C. Left atrium with 4 pulmonary veins with ostia of different dimensions and one large left pulmonary vein D. Left atrium with 3 pulmonary veins on the right side and two on the left side
Discussion
Approximately 70% of the general population has four pulmonary veins: right superior and inferior and left superior and inferior pulmonary veins, with four independent ostia [1,3,5]. Marom EM et al., divided the pulmonary vein and its drainage orifices into 6 patterns on the right side and 2 patterns on the left side [3]. According to his study, the most common drainage pattern was two pulmonary veins, each on right and left side, with two separate ostia. The next common drainage pattern on the right side was three pulmonary veins with three ostia (24%) and on the left side, they noticed a single pulmonary vein with a single ostium in14% of specimens. Earlier, it was found that, variations in the right pulmonary vein drainage were more common than those on the left [1,5]. Similarly, in the present study also, about 28% cases showed variable pulmonary veins on the right side and only 6% showed variations in the left pulmonary veins.
There were 14% samples with a single venous ostium on the right side and 6% specimens which had one venous ostium on the left side. This may have been caused by confluence of either superior pulmonary veins or both inferior pulmonary veins, or of the superior and inferior pulmonary veins on one side. The latter appeared as a single ostium and it is present in 12–25% of the general population, which is commonly seen on the left side, as was seen in this study (single left pulmonary ostium seen in 6% cases).
In a cadaveric study which was conducted by Ho SY et al., 16% of the hearts showed a single ostium for pulmonary veins 6. Marom and his co-workers, in their study which was done on CT imaging, showed 3 to 5 ostia on the right side in 26% patients and a single ostium on the left side in 14% of the patients [3]. In another study, 9% of the hearts showed five veins, 4.5% showed three veins, 3% showed two anomalies each and 0.5% showed three anomalies [7].
Congenital pulmonary venous abnormalities are related to the complex development of the venous system. The common pulmonary vein develops around the embryonic day 24, at the sinoatrial region which is to the left of the septum primum. Through a differential growth, the common pulmonary vein becomes incorporated into the left atrium and connections to the systemic veins are lost, resulting in the usual arrangement of four pulmonary veins draining into the left atrium, with separation of the systemic and pulmonary venous systems [8]. In a majority of cases, two pulmonary veins drain into the left atrium on each side. This normal arrangement occurs in 82% of the population [7]. In anatomical terms, pulmonary venous anomalies are classified as anomalous connections, anomalous drainages, or abnormal numbers of pulmonary veins [9]. The number of pulmonary veins which drain into the left atrium can vary from one to five.
Supernumerary or accessory pulmonary veins with their own ostia occur by over-incorporation of the pulmonary veins beyond their first division and such variations are usually found on the right side [3]. Similarly, the present study also showed that 12% of the cases had three ostia and that 2% of the cases had four ostia on the right side. Further, no case of supernumerary pulmonary veins was found on the left side in this study.
The pulmonary ostia receives the extension of myocardial tissue and hence, the ectopic atrial activity. Studies have revealed that such myocardial sleeves are larger in superior pulmonary veins than in their inferior counterparts. In addition to this, myocardial sleeve thickness reduces, with increasing distance from the pulmonary venous ostium [10]. These findings could invariably guide the interventionists to reach the specific location of the ectopic tissue of atrial activity and reduce the complications of radiofrequency ablation procedures.
This phenomenon should be kept in mind, as the extensions of myocardial sleeves into the pulmonary venous ostia could contract in atrial systole, thereby, reducing the reflux of left atrial blood into the pulmonary veins. Otherwise, the reflux of blood into the veins reduces the ability of the left atrium in filling the left ventricle, leading to a decreased cardiac output.
Conclusion
The anomalies of the abnormal pulmonary veins may mimic a Pulmonary Arteriovenous Malformation on roentgenographic imagings of the chest. This study’s results confirmed that there was a substantial variation in pulmonary venous anatomy, with respect to their numbers and drainage patterns. Knowledge on such variations is significantly important for radiologists and thoracic surgeons prior to the performance of procedures which directly or indirectly involve the pulmonary veins.