In the normal heart, oxygenated blood is supplied by two coronary arteries that arise from the ascending aorta. The LMCA originates from the left posterior aortic sinus and it runs towards left, under the left auricle. After a short course, it divides into two vessels, left anterior descending artery and circumflex artery [1]. The left coronary artery trunk presents a wide variability in it’s morphological expression with regards to it’s length, level of origin and number of terminal branches. Even the angiographic measurements of coronary artery length are probably less accurate than those seen in post-mortem pathologic studies, due to their under estimation by the effects of rotation angulation and foreshortening [2]. There is a correlation between the length of the main left coronary artery and the atherosclerosis present in it’s branches or the presence of a complete left bundle branch block [3]. Thus, the knowledge on such variations is important for evaluation of percutaneous coronary artery interventions, coronary artery surgeries or prosthetic valve replacements and last but not the least, for its academic value among upcoming clinicians.
Materials and Methods
From the Department of Forensic Medicine, IPGMER, Kolkata,India. hundred specimens of heart were collected by cutting ribs and sterna and opening of thoracic cavities of the cadavers. The great vessels, ascending aortas and pulmonary trunks were ligated by using threads at two places and they were then cut in between the two ligatures. The parietal pericardium was incised and the heart, along with the proximal part of the great vessels, was taken out of the pericardial cavity. Then, the aorta and the pulmonary trunk were excised about 2 cm above the supravalvular ridge. All the collected samples were kept in 10% formalin. After a gradual separation and retraction of the myocardial fascicule, the left coronary artery was exposed. The length of the main trunk was measured by using a vernier calliper as has been described in [Table/Fig-1] and the branching patterns were noted. The ascending aorta was cut longitudinally (near the Rt posterior non coronary sinus) to check the position, number and level of the left coronary ostium. A statistical analysis was performed by using SPSS (Statistical Package for Social Sciences), version 15.0. The values were represented in number (%) and Mean±Standard deviation.
Level of left coronary ostium
| Level of Left Coronary Ostium | Numbers | Percentage |
|---|
| Below STJ | 33 | 33% |
| At STJ | 31 | 32% |
| Above STJ | 34 | 35% |
| Total | 98 | 100% |
Results
Among 100 samples, 2 were discarded due to severe putrefaction. On dissecting the rest of the cadaveric heart samples, the left coronary artery trunk was found to originate from left posterior aortic sinus in all the cases. The level of ostium was different in relation to STJ (junctional zone between sinuses and tubular part of ascending aorta), which has been shown in [Table/Fig-2]. From the table, it is evident that in a large number of cases (35%), it originated above the level of STJ. In relation to the branching pattern of LMCA, we found bifurcations in 57 samples, i.e., 56% cases, trifurcations in 39 cases, i.e., 40% and in 2 cases, quadrifurcations were seen. In our samples, we did not find any pentafurcations. The mean length of the left coronary artery trunk was found to be 11.42±4.98 mm, the range being 0.5–21.5 mm [Table/Fig-3].
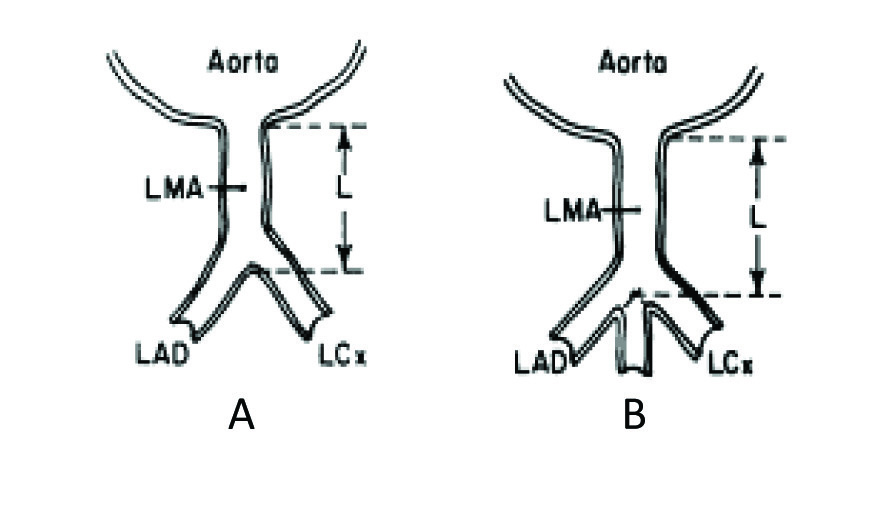
Short length of left main coronary artery

Schematic diagrams of cross section through ascending aorta and left coronary artery.In A length (L) of left main coronary artery(LMA) is from outer aortic wall to site of bifurcation into Left ant descending (LAD) and left circumflex (LCX) branches. In B, length of LMA when trifurcation occurs
Discussion
Sound knowledge on basic anatomy of LCA has recently been emphasized due to increasing use of diagnostic and therapeutic interventional procedures.
The location and level of the ostia are very important for the successful performance of a coronary angiogram during manipulation of the catheter tips. Difficulties may arise more considerably in patients in whom the ostium is above the level of sinotubular ridge (Taylor and Thorne) [4]. Banchi A [5] reported that the LCA arose at the level of free margin of aortic cusps in 48% cases, above it in 34% cases and below it in 18% cases. A study done by Kalpana R [6] revealed that the ostium was below the STJ in 80% cases and at STJ level in 20% cases. A study done by Dombe DD et al., [7] found that the level of ostium was below STJ in quite a large number of specimens (around 79.7%), whereas it was at the same level as it in 17.2% cases and above its level in only 3.1% cases. In our study, it was found that the level of ostia above the STJ was 35%, at 32% and that its level below STJ was 33%. Slit like ostia were seen in a number of cases. There have been reported cases of sudden deaths which had occurred in young individuals, where during autopsy, left sided ostial opening was found to be slit like [8].
Normally, there is only one ostium in the left posterior aortic sinus for the LCA [Table/Fig-4a,4b]. But multiple ostia were reported in the left posterior aortic sinus. Cavalcanti [9] described that in about 1.82% of the specimens, the circumflex artery and anterior descending artery arose directly from the aorta. Study done by Dombe DD et al., also showed separate origins of these two branches in one sample [7]. Topaz O et al., [10] suggested that recognition of this coronary ostial anomaly was necessary to ensure an accurate angiographic interpretation and that it was important for patients who underwent cardiac surgeries, where there would be selective perfusions of these separate vessels during performances of cardiopulmonary bypass. In our study, we found single ostia at the left posterior aortic sinus in all the specimens which were studied.


In the present study, the mean length of the LMCA was 11.42±4.98 mm, the range being .5 mm to 21.5 mm. Similar study done by Green GE et al., [11] showed that in 48% cases, the LMCA were 10mm or less in length and that in the remaining 52%, the length was upto 25 mm. A study done by Reig and Petit [12] revealed that the average length of the main trunk was 10±5.52mm (range being 2-23 mm). Gazetopoulos N et al., [3] studied the relation between the length of the main left coronary artery and the degree of atherosclerosis in it’s branches by post-mortem examination and suggested that in cases with a short main left coronary artery, the atherosclerotic lesions in the anterior descending and circumflex branches appeared earlier, progressed faster at higher levels of severity and led more frequently to myocardial infarction than in cases with a long left coronary artery. During aortic valve surgeries, myocardial perfusion depends on the positioning of one or more cannulas in the coronary arteries. In this regards, the length of LMCA is important, because when catheter is inserted into one of the terminal branches, the opacification of the other branch will not occur and thus, an incomplete image of coronary artery tree will be found.
The division of LMCA also shows wide variations. A comparative study was done along with other previous studies and it’s results have been depicted in [Table/Fig-5].
Comparative study of branching pattern of LMCA
| Authors and year | Specimen | Branching Pattern |
|---|
| Baptista CA et al., [13] | 100 | B:60%; T:38.18% Direct LAD & LCx from ostium:1.8% |
| Cavalcanti JS [9] | 100 | B:47%; T:40%; Q:11%; P:1% |
| Reig and Petit [12] | 100 | B:62%Tor Q:38% |
| Ballesteros and Ramirez [14] | 154 | B:52%; T:42.2%; Q:5.8% |
| Das H [15] | 100 | B:60%; T:35%; Q:5% |
| Dombe DD et al., [7] | 64 | B:54.7%; T:35.9%; Q:7.8% Direct LAD & LCx from ostium:1.6% |
| Present study | 98 | B:60%,T:38%Q:2% |
So, this study done on eastern region population of India showed similar branching pattern of left coronary artery trunk as was seen in previous studies, but it showed a high origin of LCA trunk in a significant number of cases.