Neonatal Gastric Teratoma: A Rare Entity
Bikram Kharga1, Vijay Kumar2, P. Santosh Prabhu3, Sundeep P.T4, Sijo K John5
1Registrar, Department of Paediatric Surgery,Kasturba Medical College, Manipal, Karnataka, India.
2Professor & HOD, Department of Paediatric Surgery,Kasturba Medical College, Manipal, Karnataka, India.
3Associate Professor, Department of Paediatric Surgery,Kasturba Medical College, Manipal, Karnataka, India.
4Associate Professor, Department of Paediatric Surgery,Kasturba Medical College, Manipal, Karnataka, India.
5Registrar, Department of Paediatric Surgery,Kasturba Medical College, Manipal, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bikram Kharga, Registrar, Department of Paediatric Surgery, KMC, Manipal, Karnataka, India – 576104
Phone: 9986762982,
E-mail: bik786@yahoo.co.in
Gastric Teratoma is an extremely rare neoplasm seen in children. It is mostly benign and predominantly seen in males presenting with an abdominal mass. The lung and stomach are very unusual sites for teratoma. Gastric teratoma accounts for less than 1% of all teratomas, less than 100 cases are reported in literature. We report a case in a 20-day-old infant who presented with large abdominal mass; our case is an addition to the few limited known gastric teratomas reported in the world literature.
Teratoma, Exploratory Laprotomy
Case Report
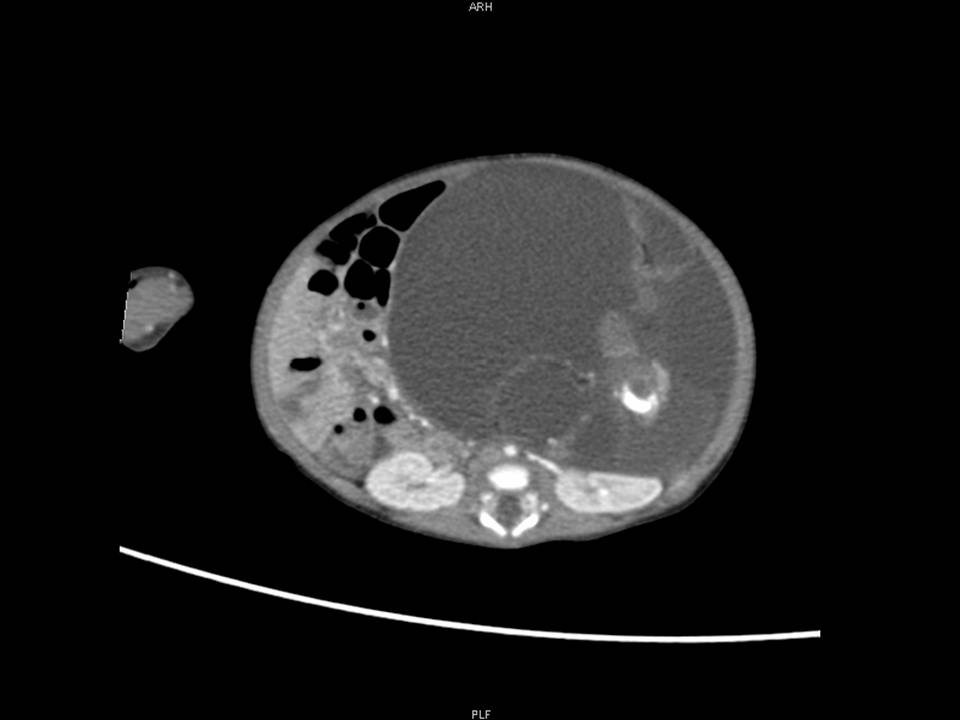
A twenty-day old male infant presented with mass abdomen since birth. He was referred to us with ultrasound findings suggestive of left gross hydronephrosis. Other than mass abdomen the infant was asymptomatic. On abdominal examination, a non-tender cystic mass felt extending from epigastrium, left hypochondrium down to pelvis crossing the midline. All the laboratory investigations were normal including serum alpha-fetoprotein (AFP) and beta-human chorionic gonadotropin (hCG). Ultrasound showed a huge complex cystic mass with multiple septations and solid components, both the kidneys were normal. CT scan [Table/Fig-1] revealed a large cystic lesion of 11.6 × 9cms, with enhancing solid component multiple septations and calcifications within the left hemi-abdomen extending from left hemi-diapharagm to pelvis crossing the midline. Preoperative working diagnosis was abdominal teratoma.
On exploratory laparotomy [Table/Fig-2], a large cystic tumour (14x10x10cm) was seen arising from lesser curvature of stomach occupying whole lesser sac and abdominal cavity. Tumour was densely adherent to lesser curvature of stomach but was completely excised [Table/Fig-3] and sent for histopathology, rest of viscera was normal. The histopathology was reported as mature teratoma, post-operative course was uneventful. There has been no evidence of recurrence during the follow-up period of one year.
Intra-operative picture of gastric Teratoma


Discussion
Teratomas are neoplasms that originate in pluripotent cells and are composed of a wide variety of tissues foreign to the organ or anatomic site in which they arise. Teratomas most often occur in a para-axial or midline location from the brain to the sacral area, as well as, in the gonads. Gastric teratoma is an extremely rare tumour in pediatric age-group, accounting for less than 1% seen in this age-group. To date, less than 100 cases have been reported in literature [1-2], vast majority being benign.
The frequently occurring teratoma in paediatric patients comprise of sacrococcygeal teratoma followed by those originating from mediastinum, gonads, presacral, rarely retroperitoneal, intracranial and cervical. Gastric teratoma is believed to arise from the pluripotent cells of the gastric visceral wall [3]. It can be mature or immature based on the presence and differentiation of neuroglial tissues. Majority of them are benign and immature, found exclusively in males, and often detected during the first year of life.
Gastric teratoma was described for the first time by Eusterman and Sentry in 1922 [4].The site of gastric teratoma is variable most commonly from greater curvature and posterior wall of the stomach, however, in our patient it was seen arising from lesser curvature which is less common [5]. Majority of tumours are exogastric, but sometimes a small endogastric component or mixed variety may be present. The clinical features depend upon the site of origin, size, and endogastric component. The usual clinical features are abdominal distension, vomiting, constipation and respiratory distress. In case of intramural extension the patients may present with hematemesis or melena.
The investigating modalities include abdominal radiograph, ultrasonography, and CT/MRI scan. The monitoring of AFP and beta hCG reflect the treatment response after excision and may be of significant value where chemotherapy is recommended in immature teratomas. Most of the gastric teratomas are benign, but malignant cases have been reported, also peritoneal gliomatosis is seen following removal of teratoma during follow-up.
The treatment is complete excision of tumour and long term followup [6]. The surgical treatment is dictated by the type and involvement of stomach being partial, subtotal or total gastrectomy.
Conclusion
Gastric teratoma is an extremely rare embryonic neoplasm, majority being benign. Complete surgical excision and long term follow-up with AFP and beta hCG depending on the type is the standard protocol to be adopted.
[1]. MS Cairo, JL Grosfeld, RM Weetman, Gastric teratoma: Unusual cause for bleeding of the upper gastrointestinal tract in the newbornPediatrics 1981 :67-721. [Google Scholar]
[2]. NA Muñoz, H Takehara, N Komi, K Hizawa, Immature gastric teratoma in an infantActa Paediatr Jpn 1992 (34):483-8. [Google Scholar]
[3]. KB Logani, A Tayal, S Bhan, M Choudhary, G Uma, Gastric teratoma in infants-a report of two cases.Indian J Cancer 1983 30:34-37. [Google Scholar]
[4]. GB Eustermann, EG Sentry, .Benign tumours of the stomach: Report of 27 casesSurg Gynecol Obstet 1992 34:372-8. [Google Scholar]
[5]. SK Ratan, R Kulshreshtha, Immature gastric teratoma in an infantIndian Pediatr 1999 36:847-9. [Google Scholar]
[6]. YS Ko, LH Lin, DF Chen, Abdominal teratomas in childrenActa Pediatr Sin 1995 36:342-45. [Google Scholar]