DOMS has post exercise onset of 8-10 hours with soreness peaking 24-48 hours post exercise [1–3]. DOMS often develops after resistance training especially after the intensity and volume of training are increased, the order of exercise is changed or a new training regime is performed [4]. Numerous interventions aimed at alleviating DOMS has been proposed like Transcutaneous Electrical Nerve Stimulation (TENS) [5], ultrasound [6] and the administration of aspirin and other anti-inflammatory drugs [7], steroids [8] and vitamin C and other antioxidants [9].
Vibration therapy improves muscular strength, power development and kinesthetic awareness [10], improve muscle performance and preventing sarcoma disruption. Vibration therapy effectively improve muscle performance which may prevent DOMS through preventing sarcoma disruption [11–13]. Massage can reduce the tension on the muscle tendon unit that affects the visco-eleastic component of the tissue leading to an increase in competence of the muscle and improvement of muscular flexibility reducing muscle stiffness and also increasing blood flow [14]. Researchers have demonstrated that massage has preventive effects ,decrease muscle soreness and other symptoms [15–19].
Considering all the facts and discussions the aim of the present study is to compare the effect the vibration therapy and massage in preventing DOMS and to evaluate the change in muscle soreness, ROM, MIF, 1RM, Serum CK level and LDH level.
Methods
The study was approved by Institutional Ethical Committee of Jamia Millia Islamia. Pre-test and Post-test Control-Group Design was used, 45 healthy female non athletic subjects were randomly assigned to the three equal groups. After the subject’s initial condition was measured experimental groups received vibration therapy or massage therapy intervention and control group received no treatment, just prior to the eccentric exercise.
Subjects were undergoing the following measurements to evaluate the changes in the muscle condition (without bold in continuation with the earlier lines).
Muscle soreness (pain perception), ROM, MIF, 1 RM, LDH and C K level. All the parameters except LDH, CK and 1RM were measured before, immediately post intervention, immediately post exercise, 24 hours post exercise, 48 hours post exercise and 72 hours post exercise. LDH, CK and 1RM were measured before and 48 hours post exercise.
Vibration Therapy
Subject was in supine position on treatment table with arm resting by the side. The mechanical vibration of 50 Hz was used to apply the vibrations on the belly and the tendons of biceps brachii for five minutes, before eccentric exercise for induction of DOMS.
Massage Therapy
The subject was in supine position on treatment table with arm resting by the side. Each therapeutic massage technique was replicated through the watch (set timer) to control the amount of time spent per stroke as well as to control the depth of the massage. Total time for therapeutic massage was 15 minutes [20].
Exercise Protocol for DOMS Induction
General arm movement wewre performed for five minutes before the exercise for induction of DOMS. After that, subjects were seated on the stool with their back supported against the wall. All subjects performed eccentric exercise of elbow flexor muscles using a dumbbell. Weight of the dumbbell was 80% of the pre exercise MIF. Subjects were instructed to lower the dumbbell from elbow flexed (50 degrees) to an elbow extended position (170 degrees) in 4-5 seconds, keeping the velocity as constant as possible by following the examiner counting ‘0’ for the beginning and ‘1, 2, 3, 4, 5’ during movement. After each eccentric action the examiner removed the load and them arm was returned to the starting position. The movement was repeated after every 45 seconds for 30 repetitions. This long interval between the repetitions minimized the effect of fatigue. Subjects were verbally guided to lower the dumbbell for constant velocity for the whole ROM [21].
Dependent Variables
Muscle soreness
Muscle soreness was evaluated using a visual analog scale [21]. The subjects were asked to indicate his perceived level of muscle pain (soreness) in the non dominant elbow flexor muscle on the line when an investigator extended the elbow joint.
Elbow joint angles and ROM
Subject was in the standing position. The goniometer was placed on the subject arm with the center located at the elbow joint. Two elbow angles were measured. Flexed elbow joint angle (FANG) was determined when subjects were asked to fully flex the elbow joint by touching their palm to shoulder without raising the elbow. For placements of goniometer semipermanent marker was used to identify the lateral middle point of the humerus, the lateral axis point of elbow joint. Relaxed elbow joint angle (RANG) represented the angle with the arm relaxed along the side of the body during standing. RANG was determined when subjects relaxed the arm allowing it to hang down by the side. For placements of goniometer a semipermanent marker was used to identify the lateral middle point between radius and ulna. FANG and RANG were measured three times for each time point using a plastic goniometer, and the average of the three measurement was calculated, and ROM was defined as the angle subtracting the mean FANG from the mean RANG [21].
Maximal Isometric Force
Subject were tested while supine lying on a padded mat on the treatment couch / treatment table. Their designated non dominant upper extremity were positioned with the shoulder abducted about 30degree, the elbow flexed 90 degree and forearm supinated with their feet against their wall [11]. Strength was measured with the help of a strain gauge (mounted on a wall). Height of strain gauge was adjusted according to the length of the subject’s forearm. Instruction to the subjects were to take 1-2 sec to come to maximum force generation along with pulling strain gauge and then continue flexing the elbow as hard as possible for 5 second. Consistently verbal encouragement and command was provided throughout every effort. Three measurements were taken for each subject and consequent measurement was separated by 2 minutes rest. The mean values of three measurements were used for the analysis [11].
One Repetition Maximum (1RM)
The 1 RM is the ability of a person to lift a certain weight once. The EN-TreeM 24 kg (Enraf Nonius) software calculates 1RM with the aid of the 1RM protocol. Subjects were in a sitting position and perform Scott-curl on ENTree pulley. Instruct the subject to inhale during flexing the elbow and exhale during extending it. The subjects are to perform a controlled, smooth and well coordinated movement. The test was stopped as soon as the subject cannot perform the movement well coordinated any longer. Strong verbal encouragement was provided during the measurement. The mean values of two measurements were used for the analysis.
Blood sampling, CK, and LDH
1 ml sample of venous blood was collected from the cubital fossa region of the dominant arm. The blood was allowed to clot for 30 minutes at room temperature and centrifuged for 10 minutes to obtain serum. After separation, all serum samples were stored at –20°C until analysis for CK and LDH activity [21]. Serum CK activity was determined spectrophotometrically by using a test kit CK (NAC act.) kit (Mod. IFCC Method) CORAL, Goa, INDIA and LDH (P-L) kit (Mod. IFCC Method) CORAL, Goa, INDIA.
Statistical Analysis
All the data obtained from three groups was tabulated. Statistical analysis was performed using Stata 11 software. One way ANOVA was done to find difference between three groups and corresponding Post-hoc analysis (Bonferroni test) was done to find pair wise difference.
Results
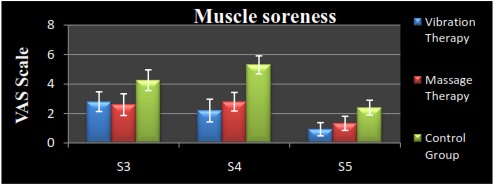
Muscle Soreness
Muscle soreness developed after exercise in all three groups but significantly less for experimental (vibration and massage) group (p=0.000) as compared with control group at 24, 48, and 72 hours of post-exercise. Vibration shows early recovery compare to massage at 24 hours (p=0.031) [Table/Fig-1].
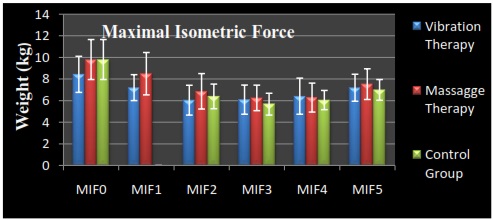
Maximal Isometric Force (MIF)
No significant difference in per exercise MIF (p=0.4189) was found between experimental and control group. Experimental and control group did not shows any significant difference immediate (p=0.2898), 24 hours (p=0.4173), 48 hours (p=0.752) and 72 hours (p=0.5297) of post-exercise [Table/Fig-2].
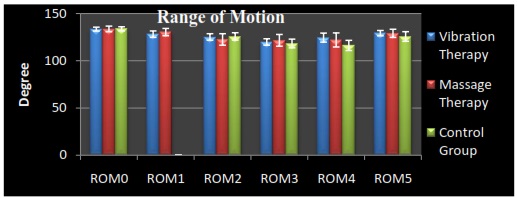
Range of Motion (ROM)
No significant difference in pre exercise ROM (p=0.9322) was found between experimental and control group. Both experimental and control group did not show any significant difference immediate (p=0.1458), 24 hours (p=0.1892) of post-exercise. In 48 hours (p=0.0016) and 72 hours (p=0.0463) significant recovery shown by experimental groups [Table/Fig-3].
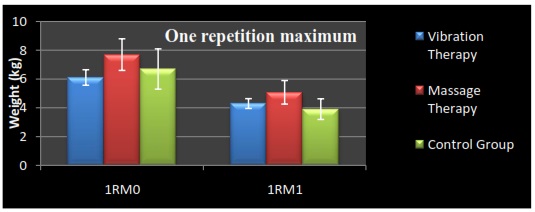
1RM
No significant difference in pre (p=0.314) and 48 hours (p=0.342) post exercise in vibration and control group. Vibration group shows significant difference in pre (p=0.001) and 48 hours (p=0.008) post exercise compare to massage group. Massage therapy shows significant recovery (p=0.000) compare to control group [Table/Fig-4].
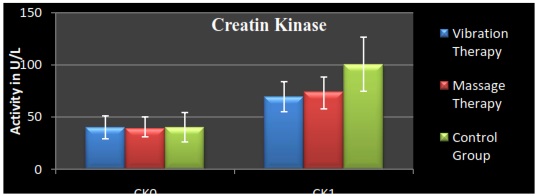
Creatin Kinase (CK)
No significant difference in pre exercise CK level (p=1.000) was found between both experimental (vibration and massage) and control group. After 48 hours of post exercise vibration group (p=0.000) and massage group showed (p=0.002) significan difference compare to control group. No significant difference found in experimental groups (vibration and massage) at 48 hours (p=1.000) post exercise [Table/Fig-6].
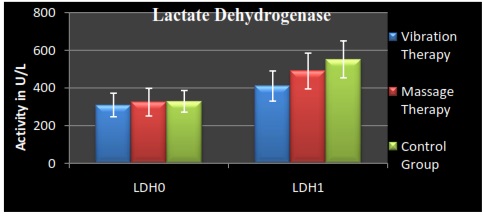
Lactate Dehydrogenase (LDH)
No significant difference in pre exercise LDH (p=1.000) was found between both experimental (vibration and massage) and control group. Vibration therapy showed significantly lesser LDH level (p=0.000) 48 hours of post exercise compare to control group [Table/Fig-6].
Discussion
DOMS is caused due to microscopic muscle fibre tears and is commonly observed after unfamiliar high-force muscular work [3].
Effect of Interventions on Muscle Soreness
Vibration provides stimulation to muscle spindles and increases its afferent activities. Vibration and TENS both reduce the perception of pain through same mechanism of pain gait theory [22]. This lead to increase in background tension and motor unit activity synchronization in the vibrated muscles [23,24] that prevent sarcoma disruption or damage to excitation–contraction coupling [25] which occurs due to eccentric exercise. This preparatory effect leads to less damage to the muscle resulting in less pain perception in post exercise duration [12,13,17,26].
Massage reduces mechanical overload on sarcomeres during lengthening actions (eccentric exercise) and prevent sarcoplasmic reticulum ruptures which decreases intracellular calcium and trigger calcium-sensitive degradative pathways and leads consequentially to less ultrastructural damage [14]. In this way massage is effective to reduce pain in DOMS. Massage minimizes negative-performance factors such as muscle and connective tissue dysfunction, restricted ROM, and pain and anxiety. Therefore it may enhance performance and prevent injury resulting in less pain perception [14,27,28].
Maximal Isometric Force (MIF)
Lactate Dehydrogenase (LDH)
Effect of Interventions on ROM
Vibration training could increase ROM in the shoulder of male gymnastic [29]. On application of vibration, the motor neuron may become synchronized and result in more force production of the muscle group [30,31]. Vibration may causes motor unit activation, synchronization between muscle spindles, reflexive recruitment of previously inactive motor units which leads to more force production for the exercise [12]. Consequently, distribution of exercise load (contractile stress) over a larger number of active fibers, this prevent muscle damage or less reduction of ROM [17].
Massage generates mechanical pressure on the muscle tissue in order to decrease tissue adhesion. Mobilizing and elongating shortened or adhered connective tissue may increase muscle-tendon compliance. Improved muscle compliance results in a less stiff muscle-tendon unit [14,32,33]. These effects help to restore muscle flexibility in post exercise period or restoration of ROM.
Effect of Interventions on Maximal Isometric Force
Strength decrement following eccentric exercise muscle action was due to soreness (mechanical reflex inhibition [34]) which prevents subjects to fully activate their muscles [35]. Other researchers have different beliefs such as calcium deficiency in the sarcoplasmic reticulum, it could be postulated that there would be insufficient calcium to support the continuous cross bridge cycling needed for complete muscle fiber shortening [36]. Majority of researchers believe that strength reduction is because of myofibrillar damage involving Z-band and sarcomere disruption caused by performing eccentric contractions [1–3, 37,38].
Many research scholar have shown that post exercise vibration [39,40] and massage [7,41,42] therapy have no significant impact on MIF restoration in case of eccentric exercise. Our result is in contrast with the result of some researches [12,26] who show significant difference in MVC in VT and non VT groups [12,26].
Effect of Intervention on Cretain Kinase
CK is the primary enzyme regulating anaerobic metabolism and has been used as an indirect marker of DOMS in healthy individuals [43]. There is a strong relationship between CK and the clinical signs of DOMS [44,45]. CK is released in case of damage to muscle tissues and change in the myocyte membrane permeability. The myocyte membrane permeability of muscles which undergo unfamiliar exercise changes and hence CK is released. Thus, CK release was higher in control group as opposed to experimental group where the effect was mitigated by the preparatory massage and vibration therapy.
Application of 50 Hz vibration before exercise causes less damage to muscle tissues and there may be less changes in the myocyte membrane permeability, resulting in less releases of CK in blood compared to control group after 48 hours of post exercise. Many research scholar have shown that post exercise vibration [12,17] and massage [20,15] therapy have significant impact on CK level in post-eccentric exercise duration.
Effect of Interventions on LDH
Vibration therapy leads to increase of skin temperature and blood flow [46] leading to decreased accumulation of lactic acid in the blood. Therefore, Lower LDH activity level was found in vibration group compared to control group 48 hours post exercise. However, massage group has not shown this significant difference with the control group pointing to the fact that massage may not be an effective intervention to reduce LDH activity in the blood.
Effect of Intervention on 1RM
Massage provides the better preparatory and warm up effect in the muscle this results in less reduction and early restoration of isotonic muscle strength (1RM). Rodenburg et al., (1994) reported increased maximal isotonic force in post–exercise massage group compared to control [15]. In present study, vibration therapy failed to show any significant difference in 1 RM restoration. Some studies are reported that vibration therapy was not effective in recovery of muscle strength [39,40].
Conclusion
The result of this study indicates that vibration therapy and massage therapy both are equally effective in prevention of DOMS. Massage is more effective in restoration of concentric strength (1 RM), yet vibration therapy shows clinically early reduction of pain and is effective in decrease the level of LDH in 48 hours post exercise periods. They can be used as an alternative to each other depending on the requirement and condition. But the difference in time taken for the execution of the treatment can play a pivotal role. Situations where time is the essence, vibration can be used and in other the concerned therapist’s skill and choice may decide the interventions.