Study of the Effect of Stress on Skeletal Muscle Function in Geriatrics
K.N. Poornima1, N. Karthick2, R. Sitalakshmi3
1 Tutor, Department of Physiology, SRM Medical College, Potheri, Kanchipuramdistrict, Tamilnadu, India.
2 Tutor, Department of Physiology, SRM Medical College, Potheri, Kanchipuramdistrict, Tamilnadu, India.
3 Assistant Professor, Department of Physiology, Sree Balaji Medical College and Hospital, Chromepet, Chennai, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Mrs. K.N. Poornima, Tutor, Department of Physiology, SRM Medical College Hospital & Research Center, Potheri-603 203, Tamilnadu, India.
Phone: 9840044803,
E-mail: karthicpoornima@gmail.com
Background: Old age is associated with weakness of skeletal muscles and decrease in muscle functions. Usually in old-age, people undergo wasting of muscles, so they are more prone for fall and fracture. It has been stated that stress and cognition has an impact on muscle functions. This study was intended to demonstrate the effect of stress in muscle function in geriatrics.
Methods: This was a cross sectional study done at a charitable home in Chennai sub urban. The geriatric males and females in the old age home were included in this study. Sixty-four subjects were included and the persons with previous history of musculo skeletal and neurological disorders were excluded. Anthropometric parameters were recorded Maximum Voluntary Contraction (MVC) and Endurance Time (ET) were measured by hand grip dynamometer. Perceived stress score was measured by perceived stress scale questionnaire. Muscle function parameters and stress score was compared.
Results: Sixty-four subjects were included in this study and it was found out that there is a negative correlation between MVC & stress which was statistically significant. (r = -0.0675, P = 0.000). Age with MVC & ET showed a mild negative correlation but it was not significant.
Conclusion: Hormones released during stress have a negative metabolic effect in skeletal muscle. Stress can induce earlier decline in muscle strength which will eventually lead to fall and fracture. Therefore, stress should be viewed as an independent risk factor for disability and other co morbid conditions.
Hand grip, Geriatrics, Stress
Introduction
India has acquired the label of “an ageing nation” with 7.7% of its population being more than 60 years old [1]. It is shown that among the population over 60 years of age, 10% suffer from impaired physical mobility and 10% are hospitalized at any given time, both proportions rising with increasing age [2]. Skeletal muscle which is primarily involved in body movement [3] in addition to its contractile function is also involved in adaptations to starvation, disease and injury over a longer term [4]. There is a progressive decrease in skeletal muscle strength in ageing. The decline in muscle strength with age has often been attributed to declining muscle mass in older subjects. There is a selective loss of type II muscle fibers in old age [5]. Reduced muscle strength is associated with frequent falls which eventually results in fractures. Stress which has an impact throughout the body has its deleterious effect on skeletal muscle and its strength. In this study we have compared the muscle function and stress among geriatric individuals. Assessment and management of stress in geriatric individuals can reduce the risk of disability and falls.
Materials and Methods
This cross-sectional study was performed in Dec. 2009 at a charitable home for elderly in Chennai. Randomly selected 64 subjects (29 males and 33 females) were included in this study. The subjects who were between 61-91 years (who were divided into 3 groups, Group I- 61-70 years; Group II- 71-80 years; Group III- 81-90 years), of both sexes and who were physically active (ambulant), were included in the study. Those with History ofsmoking/alcohol/diabetes/hypertension/neuromuscular disorders were excluded.Written informed consents were taken from them. A detailed musculoskeletal history was taken and a clinical examination was done. A Perceived Stress Scale - questionnaire which contained both positive and negative statements was administered [6] to find out the stress level. Muscle function parameters namely MVC and ET were measured using hand grip dynamometer. MVC is done by asking the subject to hold the hand grip dynamometer in the dominant hand and to perform a maximum contraction. Three readings were taken, and between each reading one minute rest was given to the subject. Best of Three readings were taken. It is measured in kilograms. The time taken by the subject to hold 50% of MVC is called ET. It is measured in seconds. Stop watch was used to calculate the time period of ET. The muscle power was graded in to two groups. Group I - < 20 kgs of MVC and Group II - ≥ 20 kgs of MVC. Anthropometric measures like Height & Weight were measured by inch tape and weighing machine respectively. The data was expressed as mean±S.D.The statistical analysis was performed by using the SPSS software. The independent ‘t’ test was used to compare the variables. A P value of < 0.05 was taken as statistically significant. The stress questionnaire contained both positive and negative statements where 0= no stress and 4 = maximum stress. (Scores of 0-10 = no stress, scores of 11-20 = mild stress, scores of 21- 30 = moderate stress and scores of >30 = severe stress). The study protocol was approved by the ethical committee of our institute.
Results
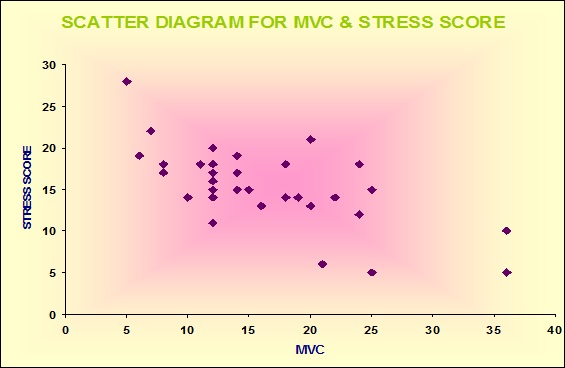
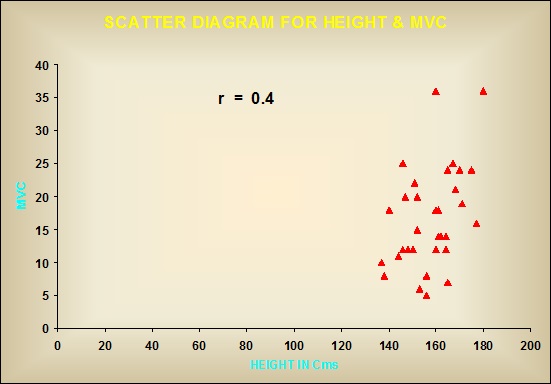
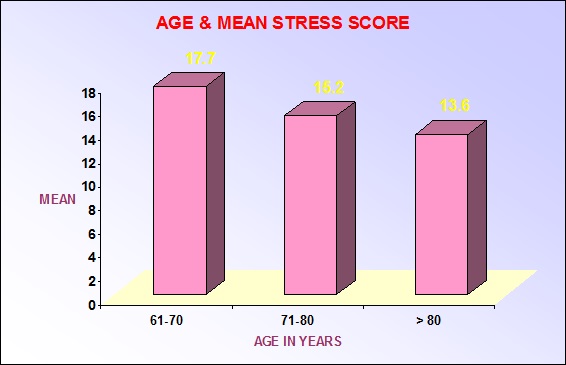
In our study, we found that the Group I subjects between 61-70 years had maximal stress ( mean stress score – 17.7), Group II subjects between ‘71-80 years had mild stress (mean stress score – 15.2 ), Group III > 80 years had minimal stress (mean stress score – 13.6 ). This was assessed by Fischer’s test and it was statistically significant P = 0.03. It was found out that there is a negative correlation between MVC & stress. This was statistically significant (r= -0.0675, P = 0.000). Among the anthropometric measures height was best correlated with MVC than weight or BMI. Weight & Height with ET though positively correlated but it is not significant. Age with MVC & ET was showed a mild negative correlation but it is not significant [Table/Fig-1,2&3].
Correlation of Maximum voluntary contraction and stress
Correlation of height and maximum voluntary contraction
Age and mean stress score
Discussion
Skeletal muscle which is primarily involved in body movement undergo various changes in ageing. There is a fall in total muscle mass and a selective loss of type II muscle fibers in old age [5]. MVC assessed by hand grip dynamometer is used as a parameter of muscle strength [7]. It can be easily assessed at the bed side of the patient [8]. Handgrip strength is an important predictor of functional limitations and disability [9]. Handgrip strength has been found to correlate with strength of other muscle groups and is thus a good indicator of overall strength [10]. The functional integrity and quality of skeletal muscle is maintained by continuous turnover of proteins. This important remodeling process is regulated by hormones. Anabolic hormones like growth hormone, insulin-like growth factor and testosterone increases the rate of protein synthesis and decreases the breakdown of protein. Stress hormones causes catabolism of muscle proteins, thereby decreasing the muscle strength [11]. Further stress hormones induces oxidative damage in the skeletal muscle and thereby interferes with it quality and fuction [12]. Our study showed significant changes in muscle strength in geriatric with stress. MVC decreases as the stress level increases and it was found to be statistically significant. A study done in healthy volunteers have shown that infusion of stress hormones causes decreased concentration of ribosomes and decrease in the relative proportion of polyribosomes in skeletal muscle [13]. Another study done by Allen DL et al., has proved that acute daily psychological stress induces atrophic gene expression and loss of muscle mass [14]. An important concept which arises from this discussion is, as the stress hormones increases it causes catabolism of proteins in the skeletal muscle and thereby reducing the muscle strength. Our study also reported a positive correlation of weight and height with ET but it is not statistically significant. Studies have shown that the Reduction in perceived stress levels results in lesser negative feelings of anxiety, depression and improved sense of well-being, better sensory-motor performance and hand grip endurance [15].
Conclusion
Hormones released during stress have a negative metabolic effect in skeletal muscle. In our study, we found significant negative correlation between MVC and stress level. This study highlights the effect of stress in skeletal muscle in geriatrics. In geriatrics already the muscle strength is reduced by wasting of muscles during ageing and this is further aggravates by stress. Stress can induce earlier decline in muscle strength which will eventually leads to increased frequency of falls and fractures. Therefore, stress should be viewed as an important risk factor in geriatrics and should be managed efficiently through counseling, yoga or meditation to prevent further muscle loss which will cause disability and other co morbid conditions
[1]. Irudaya Rajan S, Demography of ageing. In: Dey AB, editorAgeing in India, Situational analysis and planning for the future 2003 New DelhiRakmo Press [Google Scholar]
[2]. Reddy PH, The health of the aged in IndiaHealth Transit Rev 1996 6:233-44. [Google Scholar]
[3]. Forbes GB, “Human body composition”In: Growth, aging, nutrition and activityNew yorkSpringer Verlag [Google Scholar]
[4]. Rennie PJ, Fuller MF, Nicholson BA, Muscle protein turnover and the muscle wasting due to injury and diseaseBr Med Bul 1985 41:257-64. [Google Scholar]
[5]. Larsson L, Morphological and functional characteristics of ageing skeletal muscle in manActa. Physiol. Scand 1978 457:1-36. [Google Scholar]
[6]. Cole Stephen R, Assessment of differential item functioning in the Perceived Stress Scale-10J Epidemiol Community Health 1999 53:319-20. [Google Scholar]
[7]. Klidjian AM, Archer TJ, Foster KJ, Detection of dangerous malnutritionJ. Parenteral and Enteral Nutrition 1982 6:119-21. [Google Scholar]
[8]. Jeejeebhoy KN, Nutritional assessmentGastr Clin North America 1988 27:347-69. [Google Scholar]
[9]. Rantanen Taina, Midlife hand grip strength as a predictor of old age disabilityJAMA 1999 281(6):558-60. [Google Scholar]
[10]. Rantanen T, Era P, Kauppinen M, Heikkinen E, Maximal isometric muscle strength and socio- economic status, health and physical activity in 75 year old personsJ Aging Phys Activity 1994 2:206-20. [Google Scholar]
[11]. Rooyackers Olav E, Nair K Sreekumaran, Hormonal regulation of human muscle protein metabolismAnnual Review of Nutrition 1997 17:457-85. [Google Scholar]
[12]. Li Q, Zhang M, Chen YJ, Wang YJ, Huang F, Liu J, Oxidative damage and HSP70 expression in masseter muscle induced by psychological stress in ratsPhysiol Behav 2011 104(3):365-72. [Google Scholar]
[13]. Wernerman Jan, Stress hormones given to healthy volunteers alter the concentration and configuration of ribosomes in skeletal muscle, reflecting changes in protein synthesisClinSci (Lond) 1989 77(6):611-6. [Google Scholar]
[14]. Allen DL, McCall GE, Loh AS, Madden MC, Mehan RS, Acute daily psychological stress causes increased atrophic gene expression and myostatin-dependent muscle atrophyAm J Physiol RegulIntegr Comp Physiol 2010 299(3):R889-98. [Google Scholar]
[15]. Friedman BH, Thayer JF, Autonomic balance revisited: panic anxiety and heart rate variabilityJ Psychosom Res 1998 44:133-51. [Google Scholar]