Hodgkins Lymphoma of Bone - A Rare Case Report
Mangala gouri S R1, Saraswathi G Rao2, Sundaresh D.C3
1Professor, Department of Pathology,M.S. Ramaiah Medical College, Bangalore - 94, India.
2Senior Professor, Special officer GEF, Department of Pathology, Bangalore - 94, India.
3Senior Professor, President,MSRALC, Bangalore - 94, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr Mangala Gouri S.R., #12, 1st main road, 13thcross road, Hanumaiah layout, Sanjaynagar, Bangalore - 94, India.
Phone: 9449352987,
E-mail: mangalagouri22@yahoo.com
Primary Hodgkins lymphoma presenting as a lytic bone lesion is very rare. A 27-year-old male presented with deformity and pain in lower back region from past 1 year. X-ray and CT scan revealed T12 and L1 vertebral destruction and an osteolytic lesion with destruction of the Right Ilium. Clinically a diagnosis of giant cell tumour was made. However histopathology & Immunohistochemical evaluation helped in diagnosing the case as a classical Hodgkin’s disease of the bone.
Bone tumour, Hodgkins disease of bone, Primary Hodgkins lymphoma
Case Report
A 27-year-old male, presented to the out patient department with complaints of deformity and pain in lower back region from past one year. He was treated with anti tubercular treatment for four months elsewhere before presenting to us.
On examination gibbus deformity was noted at the lower thoracic and upper lumbar level with mild tenderness. No neurological deficits were detected. Patient also had generalized lymphadenopathy (multiple axillary and inguinal lymphadenopathy) and mild hepatosplenomegaly. There was a mild anemia and an increased ESR, while other parameters were unremarkable.
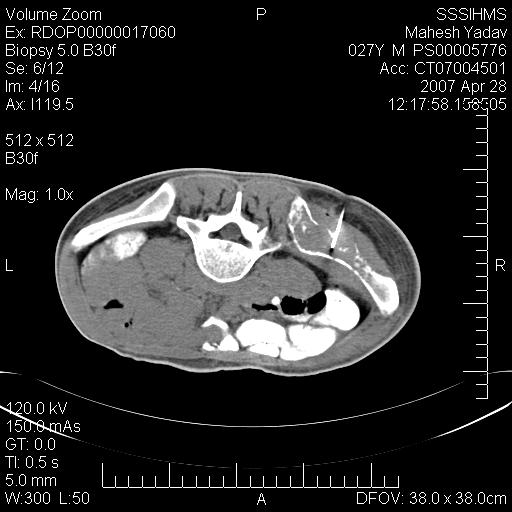
X-ray & CT scan showed destruction of T12 and L1 vertebral bodies with reduced intervertebral disc space. Osteolytic lesion with destruction of right iliac bone was seen. No lymph node masses were seen in the abdominal region close to T12 & L1 or near the Ilium on CT scan [Table/Fig-1]. Magnetic resonance imaging (MRI) scan showed lytic lesion in right ilium with destruction of T12, L1 and infiltration into neural structures at that level. Biopsy of axillary lymph node revealed changes of reactive hyperplasia.
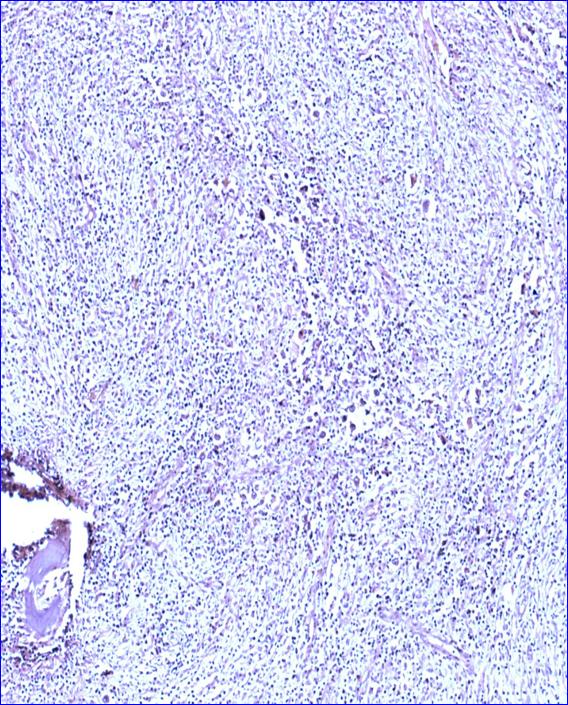
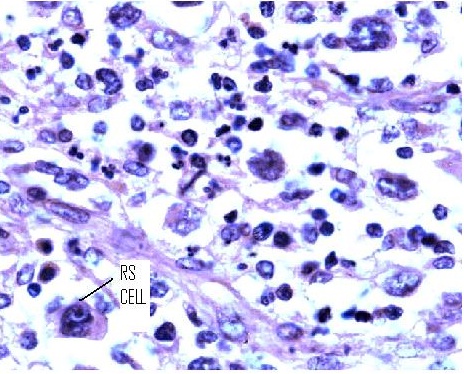
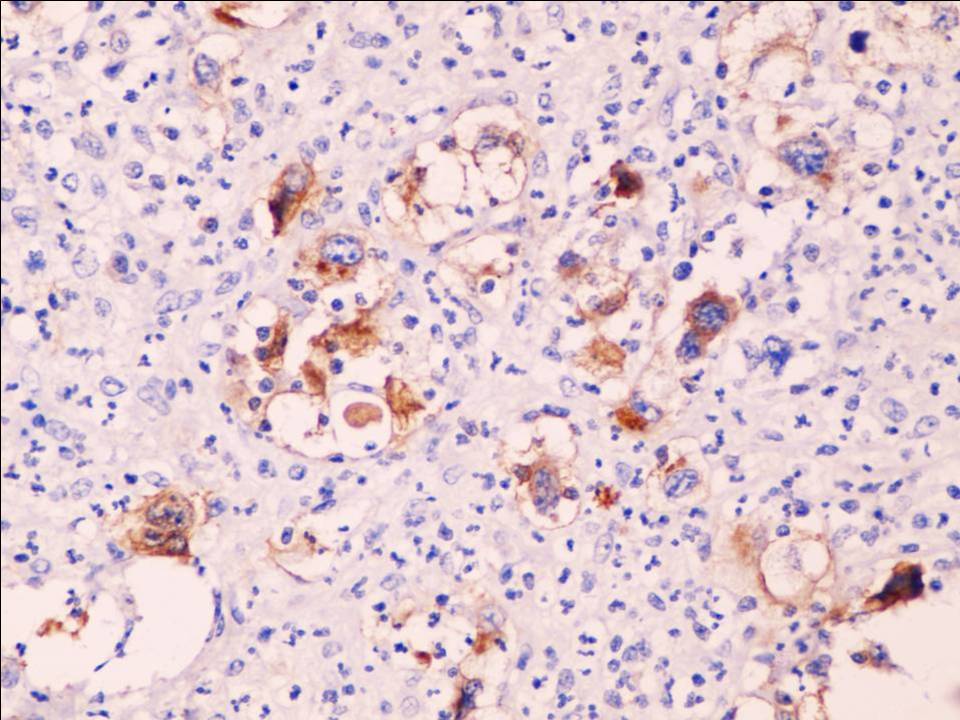
A clinical diagnosis of giant cell tumor was made. Excised tumor was sent for histopathological workup. Specimen consisted of an irregular grey white to grey brown bony mass with attached soft tissue measuring 8.5x2x1cms. Representative areas were sampled. Microscopy revealed a destructive bony lesion with extensive areas of fibrosis, scattered macrophages, lacunar mononuclear cells and a few binucleated cells in a polymorphous inflammatory background [Table/Fig-2-3]. A differential diagnosis of Hodgkin’s lymphoma, malignant fibrous histiocytoma of bone and fibrohistiocytic variant of osteosarcoma was offered, with an advice for immunohistochemistry. The Immunohistochemistry revealed RS-cells which expressed CD30 [Table/Fig-4] and were immunonegative for LCA, CD15, CD20, alk-1 & CD3. The final diagnosis was Classical Hodgkin’s disease (nodular sclerosis type).
CT Scan: Osteolytic lesion with destruction of left ilium
Bony spicule with adjacent tumour (10X)
Tumour with RS cells, large mononuclear cells and mixed inflammatory infiltrate. (400X)
IHC – CD 30 positive RS cells
Discussion
Hodgkin’s disease is type of lymphoma involving the lymphoreticular system. Hodgkin’s Disease (HD) rarely presents as a solitary bone tumor [1]. The bone involvement in later stages of HD is an expected phenomenon ,but it is very rare in early stages of the disease [2].
Lytic lesions of bone includes a variety of conditions ranging from solitary bone cyst, aneurysmal bone cyst, giant cell tumor to malignant neoplasm like multiple myeloma and Hodgkins lymphoma. It is very important to identify the lesions by various modalities such as clinical history, X ray findings and histopathology. When giant cells are seen in a lytic lesion, one of the rare differential is Hodgkins disease and hence Immunohistochemstry is important for definitive diagnosis. Reed Sternberg cells are CD 15/CD 30 positive but giant cells in giant cell tumour will be multinucleated arranged in the centre and IHC will be positive for MITF, alpha 1 antitrypsin and alpha 1 antichymotrypsin. Langerhans histiocytosis can also show large cells with lobulated nuclei accompanied by variable admixture of eosinophils ,giant cells, neutrophils and fibrosis with Immunohistochemstry positivity for S100 protein, CD1a and Langerin CD207.
Fibrous histiocytic type of Osteosarcoma is indistinguishable from that of malignant fibrous histiocytoma(MFH),however tumour osteoid may be focally present . Osteosarcoma cells are positive for osteonectin, osteocalcin,osteopontin bone morphogenetic protein, and bone GLA protein where as malignant fibrous histiocytoma tumours show reactivity to vimentin , alpha1 antitrypsin and alpha1 antichymotrypsin,KP-1(CD68),Factor Xllla, ferritin etc [3]. Hence HD of bone is a rare presentation and should be considered as a differential diagnosis to lytic lesions of bone.
Approximately 3% of primary malignant bone tumors are lymphomas. Non Hodgkin’s lymphoma of large B cell type are the most common type of lymphomas [4]. Bone involvement in Hodgkin’s disease occurs in 9% to 35% of the cases. The bone involvement is seen particularly in the later stages, but very rarely at the time of presentation [2].
Dogan et al., [2] have extensively reviewed the literature, describing 49 cases of Hodgkin’s disease with bone involvement were reported at the time of initial diagnosis The majority of these cases also had lymph nodes and other organ involvement with bone lesions at staging workup. Twenty-six (53%) of the cases were male and 23 (47%) were female. The bones most involved at the initial diagnosis were vertebrae, pelvic bones, femur, humerus, sternum, tibia, scapula, mandible and rib [2]. In our case both Right ilium and lumbar vertebrae were involved.
Surendra Kumar et al., [5] have reported a child previously diagnosed as Hodgkin’s disease and successfully treated, who later presented with solitary bone tumor in the upper part of right humerus. The radiograph showed lytic lesions over the right upper humerus. On microscopic examination the smears revealed good cellularity with plasma cells in lymphoid background. There were classical binuclear and mononuclear Reed-Sternberg cells and a few eosinophils, neutrophils and histiocytes. A diagnosis of Hodgkin’s disease was made and confirmed subsequently by histopathological examination and Immunohistochemical analysis revealed staining of the atypical cells for CD15 and CD30. The cells were negative for S-100, Keratin, CD-45, CD3, CD4 and CD4sRO. The tumor was excised and recurrent Hodgkin’s lymphoma was confirmed by histopathological examination subsequently [5].
Li Y et al., [6] have reported a case of primary Hodgkin’s lymphoma in rib of a middle aged female. CT scan, like in our case also revealed osteolytic lesion. RS and Lacunar cells were positive for CD 15 and CD30 with typical membrane and paranuclear dot – like staining pattern [6]. Our case presented with lytic lesion of right ilium. The patient was put on chemotherapy as well as radiotherapy but lost for further follow up. In our case the immunohistochemical pattern was of classical Hodgkin’s disease (Nodular sclerosis type).
Conclusion
In our experience Hodgkin’s disease should be considered in the differential diagnosis of solitary lytic bone lesions particularly if patient has generalized lymphadenopathy and radiological findings are indicative as usually lytic and rarely sclerotic to mixed reaction. FNAC or biopsy is advised to arrive at a diagnosis and immunohistochemistry will help in confirming the diagnosis. Differentiating Hodgkin’s disease of bone from the list of other tumours like giant cell tumor and Langerhans cell histiocytosis is important and it can be sorted out with immunohistochemistry.
[1]. M Ozdermirli, HJ Mankin, AC Aisenberg, NL Harris, Hodgkin’s disease presenting as a solitary bone tumor. A report of four cases and review of the literature.Cancer 1996 77:79-88. [Google Scholar]
[2]. R Dogan Koseoglu, Senayli Atilla, Bicakci Unal, Onerk-Filiz Nupur, Sezer Taner, Celkan Tiraje, Osseous presentation of Hodgkin’s disease –A case report and review of the literatureThe Turkish journal of pediatrics 2007 (49):218-32. [Google Scholar]
[3]. Rosai Rosai J, Ackerman’s Surgical pathologyHand 2011 210th EditionMissouri, USAElsevier:2028-54. [Google Scholar]
[4]. ML Ostrowski, KK Unni, PM Banks, TC Shives, RG Evans, MJ Connell, Malignant lymphoma of boneCancer 1986 58:2646-55. [Google Scholar]
[5]. Kumar Surendra, Ferns Sunitha J, B Visnnu Bhat, DK Patro, Hodgkin’s disease in Relapse presenting as bone tumour.Indian Pediatrics 2003 40:56-59. [Google Scholar]
[6]. Y Li, XB Wang, XY Tian, B Li, Z LI, Unusual primary osseous Hodgkins lymphoma in rib with associated soft tissue mass: a case report and review of literature.Diag Pathol 2012 7:64-66. [Google Scholar]