Background: Incidence of prostate cancer in India is relatively low compared to the western countries. Nevertheless, an increase by 1% yearly has been recorded in the last three years, thereby making early diagnosis of prostate cancer crucial for controlling its incidence. Differentiating between benign and malignant lesions has been a diagnostic dilemma, especially in prostate pathology. This is compounded by unavailability of modern tests in certain regions of developing nations.
Methods: A cohort of one hundred seventy six prostatomegaly patients used in the current study was obtained both retrospectively and prospectively at the Jawaharlal Nehru Medical College, Sawangi, Wardha, Maharashtra, India. Details of the patients were recorded which included their age. The samples were then cut into 5 sections, each of 5micron thickness. One section was preserved and the other 4 sections were subjected to Hematoxylin and Eosin (H and E), Periodic Acid-Schiff (PAS), Alcian Blue and AgNOR stains. Degree of differentiation was estimated and correlated with the Gleason score and the outcome of the stainings.
Results: Majority of benign prostatic hyperplasia and all primary carcinoma patients were in their sixth to eighth decade of life. While all the benign lesions were negative, 6 out of 9 primary prostate carcinomas were positive for Alcian Blue stain. Majority of both benign and malignant lesions were positive for Periodic Acid Schiff (PAS) stain. In terms of Argyrophilic Nucleolar Organiser Region (AgNOR) count per nucleus, the value in benign lesions was observed to be half the count observed in malignant lesions per nucleus.
Conclusion: Although the potential use of the orthodox stains individually may not serve the purpose to differentiate between benign and malignant lesions, together they may have the potential to identify relatively more malignant cases. This may be helpful especially in low socio-economic countries and rural areas where molecular based tests may not yet be available.
Benign Prostatic Hyperplasia (BPH), Prostate Cancer, Alcian blue, Argyrophilic Nucleolar Organiser Region (AgNOR)
Introduction
Various prerequisites for transforming a normal human cell to a cancer cell without viral oncoproteins have been outlined previously [1]. However, mechanistic insights into the regulation and molecular targets of these important requisites is still emerging [2–7]. Interestingly, several of these requisites or hallmarks of cancer [8] are common with the biology of aging [9] wherein with advancing age the changes of senile atrophy are predominant. Paradoxically, the prostate gland undergoes hypertrophy and enlargement (prostatomegaly). Prostatomegaly includes a spectrum of lesions like acute prostatitis, chronic prostatitis , granulomatous prostatitis, benign prostatic hyperplasia (BPH), prostatic intraepithelial neoplasia (PIN), atypical adenomatous hyperplasia (AAH) and prostate carcinoma (PCa). Behind this spectrum of prostatic lesions lies its characteristic histo-morphology. Histologically, the prostate is a compound tubule-alveolar organ which presents as small to fairly large glandular spaces lined by epithelium. Characteristically the glands are lined by two layers of cells ; a basal layer of low cuboidal epithelium covered by a second layer of columnar secretory cells [10]. Notably, this basal layer is continuous in humans in comparison to the mouse prostate [10]. These glands have a distinct basement membrane and are separated by abundant fibro muscular stroma. Molecularly, the basal cells have high expression of markers like CD44, cytokeratins 5 and 14 [11–13]. Notably, cells with stem cell like function are positive for CD44 and CD133 markers in addition to low expression of Androgen Receptor (AR) and high expression of α2β1-integrins [14,15]. Whereas, the secretory layer cells are positive for cytokeratins 8,18 and CD57 cell surface marker [11], in addition to being androgen-dependent [10].
Prostatic enlargement is related to the action of androgens. Intra prostatic Dihydrotestosterone (DTH), a metabolite of testosterone, is suggested to be the drive of prostatic growth. It is synthesized in the prostate from circulating testosterone by the action of the enzyme 5-alpha Reductase. Therefore inhibitors of this enzyme have been developed for prevention and treatment of BPH and prevention of primary prostate cancer [16]. In the initial stages, when the cancer is limited to the sub capsular region, it is resect able and curable. However, when the tumor is missed or diagnosed to be benign, the tumor becomes lethal and metastasizes to bone and other parts [17–19]. This makes differentiating benign from cancerous lesions very vital. Several studies have shown that understanding the histomorphology with the Gleason’s grading system, suggested to be the single most important prognostic factor, has resolved the dilemma to a great extend [20–22]. Although markers like Prostatic Specific Antigen (PSA) and Prostatic Acid Phosphatase (PAP) are currently being used for diagnosis of prostatic carcinoma, the non-specificity is still an issue [23,24]. Therefore, histo and cyto-morphology are still indispensable for the diagnosis, especially in low socioeconomic areas. The histochemistry for the mucins of the prostate has proved to be immensely helpful, especially in demonstration of somewhat cancer specific acid mucin [25,26]. Histochemistry is analyzable on the formalin-fixed and paraffin embedded tissue, which facilitates it’s wide usage. In this study, we explore the potential of three different stains, namely Periodic Acid Schiff’s (PAS), Alcian Blue at pH 2.5 and Argyrophilic Nucleolar Organiser Region (AgNOR) Stain, in the differentiating benign from malignant lesions.
Materials and Methods
Collection and preparation of patient samples
The samples from patients for the study were collected both retrospectively and prospectively at Jawaharlal Nehru Medical College, Sawangi, Wardha, Maharashtra, India. A cohort of 176 prostatomegaly patients underwent basic procedures (Department of surgery) and hospital data for name, age, registration number, ward and treating surgeon was collected after taking informed consent. Case records of retrospective cases were curated and pertinent findings in relation to age, size of prostatomegaly and type of operation for removal of prostate were noted in structured proforma. In prospective cases, their case papers were referred (from department of surgery to department of pathology) and pertinent findings were recorded. The prostatic tissue obtained during the surgical procedure and the specimens of transurethral resection of prostate (TURP) were processed in the following way: Tissues were fixed in formalin, dehydrated in graded alcohols, cleared in xylene and embedded in paraffin wax. Blocks were then prepared and 5 sections of 5micron thickness from each block were cut. One section was preserved and the other 4 sections were subjected to the following stains: Hematoxylin & eosin, Periodic Acid-Schiff (PAS) stain, Alcian blue stain, AgNOR stain. The histo-morphological assessment on H&E stained sections was performed. The cases of adenocarcinoma prostate were further evaluated for the Gleason’s grade and score. This study was approved by the ethics committee of Jawaharlal Nehru Medical College, Sawangi, Wardha, Maharashtra, India.
Hematoxylin & Eosin (H&E) Staining
Sections were de-waxed, hydrated by graded alcohols and water treatment. Fixation pigments if required were removed, followed by staining in alum hematoxylin for the stated period. Then the sections were washed in running tap water until they turned “blue”. Then dehydrate in 1 percent acid alcohol for 5-10 seconds. The samples were again washed with tap water until sections are again ‘blue’ (10-15 minutes). Then sections were stained with 1 percent Eosin Y for 10 minutes. Again they were washed with tap water for 1-5 minutes. Finally, the sections were dehydrated through graded alcohols, cleared and mounted. As a result, nuclei were observed to be blue/black, cytoplasm in varying shades of pink, muscle tissue and fibrin deep pink and RBCs as red in color.
Alcian blue Staining
Staining with Alcian blue was carried out at pH 2.5 and bluish black nuclei along with the blue colored acid mucin were observed.
Periodic Acid Schiff (PAS) Staining
Staining with PAS was carried out at pH 2.5 and bluish black nuclei along with red colored glycogen and other periodate-reactive carbohydrates were observed.
Argyrophilic Nucleolar Organiser Region (AgNOR) staining
The staining was performed using the silver nitrate method. Solution A (50% silver nitrate solution) and Solution B (gelatin solution) were prepared. 2 parts of solution A was mixed with 1 part of solution B to form the working solution. Sections were de-waxed in xylene and dehydrated with alcohol and water. After washing with distilled water, sections were incubated in freshly prepared working solution for 45 minutes in darkness and at room temperature. Then sections were washed with distilled water for 1 minute and dehydrated, cleared and mounted in DPX. The AgNOR sites were seen as intranuclear black dots and the background is observed to be pale yellow.
Counting of AgNOR positive sites
Each slide was considered as a single unit in which 100 nuclei are counted for the presence of black appearing AgNOR dots in the nucleolar region by using oil immersion lens. AgNOR dots from each nuclei (total 100 nuclei) was analyzed and mean AgNOR count for each slide was calculated [27]. The histomorphological features in the group of benign and malignant conditions were recorded.
Statistical Analysis
Statistical analysis was performed using the Chi-square test and p-values of less than 0.05 were considered statistically significant.
Results
Distribution of patient samples based on age and diagnosis with Haematoxylin and Eosin (H and E) stainings
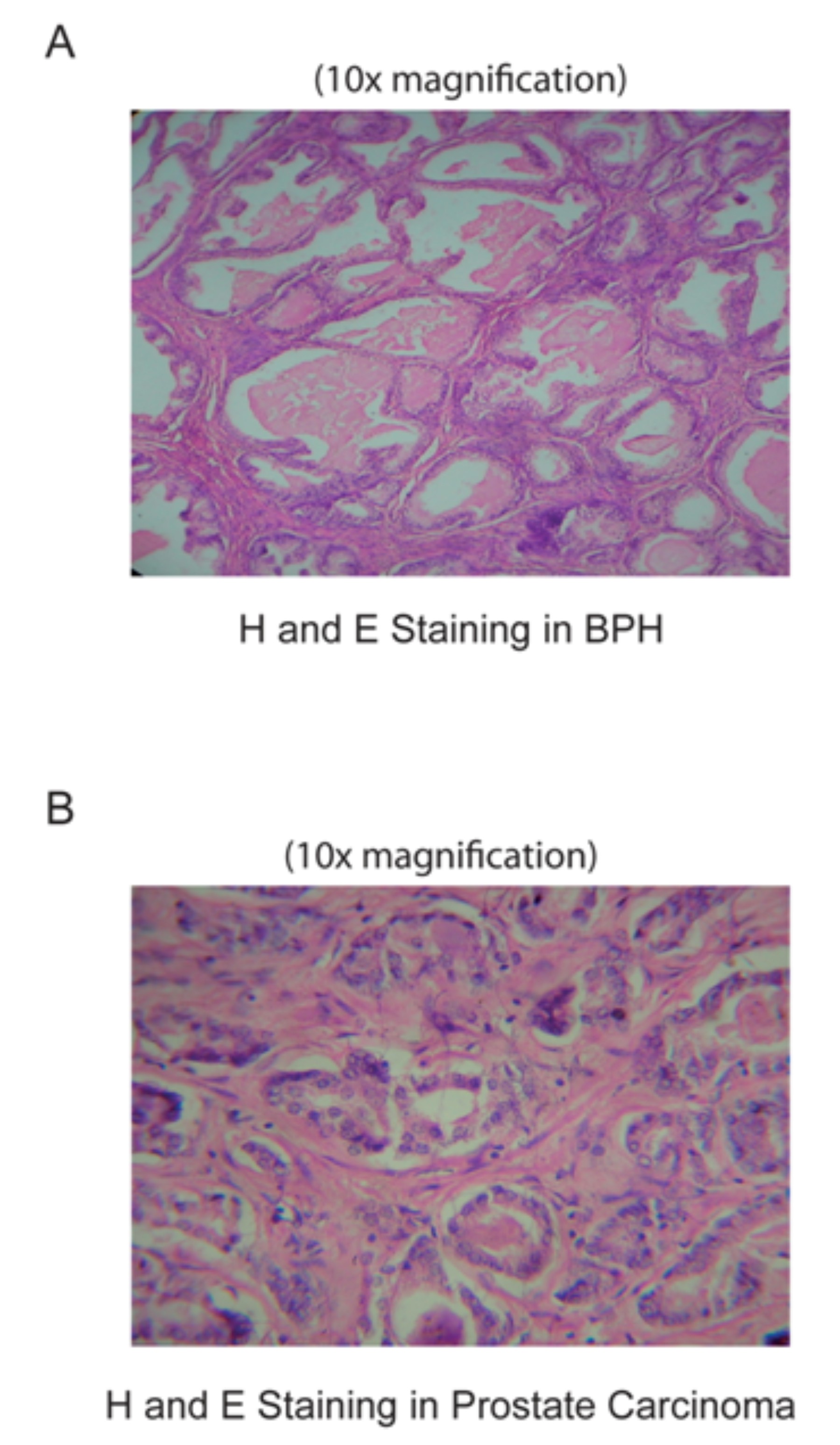
The study was carried on 176 patient samples of prostatic lesions comprising of 167 (94.89%) patients diagnosed for benign prostatic hyperplasia (BPH) and 9 (5.11%) of primary carcinoma of the prostate (PCa). Haematoxylin and Eosin (H and E) stainings for the BPH and PCa samples were done and representative images are shown in [Table/Fig-1]. Amongst the benign prostatic hyperplasia, 43.11% of cases were in the age group of 71-80 years (8th decade) followed by 38.32%, 13.77% cases in the age group of 61-70 years (7th decade) and 51-60 years (6th decade) respectively. Minimum of 4.79% of cases were in the age group of 41-50 years (5th decade). Thus more than three fourth of the benign prostatic hyperplasia cases and all the prostate cancer cases were seen in their sixth to eighth decade of life. The age of the youngest person in the study was 48 years old and the eldest patient in the study was 78 years old. None of the patients with malignant tumor were below 60 years of age. This could be attributed to the clinical presentation by the patient for which prostectomy was performed.
H and E stainings of the patient cohort of prostatomegaly patients. (A) Haematoxylin and Eosin (H and E) staining of BPH samples. Shown is the 10x magnification of the section. (B) Haematoxylin aand Eosin (H and E) staining of Primary Prostate Adenocarcinoma (PCa). Shown is the 10x magnification of the section
Alcian Blue staining
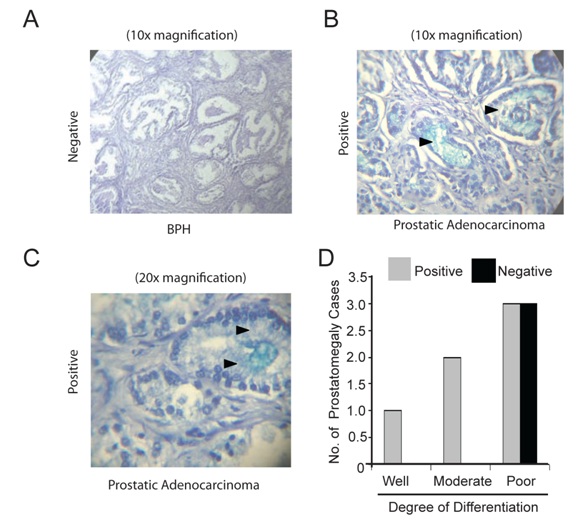
In our patient cohort of 176 patients, none of BPH cases were positive for Alcian blue staining [Table/Fig-2A]. Meanwhile, Alcian blue positivity [Table/Fig-2B] for acidic mucin was observed in 66.67% of adenocarcinomas of the prostate. The intensity of positive reaction of the Alcian blue varied from deep blue near the mucinous areas and light blue in areas without the mucinous differentiation [Table/Fig-2B]. In addition, positive staining was observed in both luminal [Table/Fig-2B] and intra-cytoplasmic compartments [Table/Fig-2C]. Finally, the degree of differentiation in the prostate carcinoma cases was tabulated against outcome of the Alcian blue staining shown in [Table/Fig-2D]. With respect to the Gleason score, the three well to moderately differentiated tumors had a Gleason score of <= 3, while the three poorly differentiated PCa cases had a Gleason Score >=4.
Alcian Blue staining of the patient cohort. (A) Negative Alcian Blue staining for acid mucin in benign prostatic hyperplasia (BPH). Shown is the 10x magnification of the section. (B) Positive Alcian Blue staining in primary prostate cancer. The black triangles point towards intra-luminal positivity. Shown is the 10x magnification of the section. (C) Positive Alcian Blue staining in primary prostate cancer. The black triangles point towards intra-cytoplasmic positivity. Shown is the 20x magnification of the section. (D) Negative and positive Alcian Blue staining in varied degree of differentiation of primary prostate cancers used in the study
Periodic Acid Schiff’s (PAS) staining
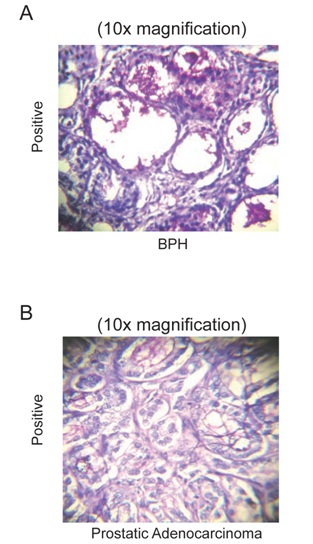
The Periodic Acid Schiff’s stain is mainly used for identification or staining of neutral mucin. PAS staining was performed on all the specimens, i.e., on BPH [Table/Fig-3A] and PCa [Table/Fig-3B]. The results for PAS staining in our patient cohort demonstrates positivity in 89.82% of BPH cases. Similarly, 66.67% of carcinoma cases were also positive for the stain. Interestingly, the three PCa cases that were negative for the PAS stain, were poorly differentiated and had a Gleason score 4, 4 and 5 respectively.
Periodic Acid Schiff (PAS) staining of the patient cohort. (A) Positive PAS staining for neutral mucin in benign prostatic hyperplasia (BPH). Shown is the 10x magnification of the section. (B) Positive PAS staining in primary prostate cancers cases. Shown is the 10x magnification of the section
Argyrophilic Nucleolar Organiser Region (AgNOR) staining
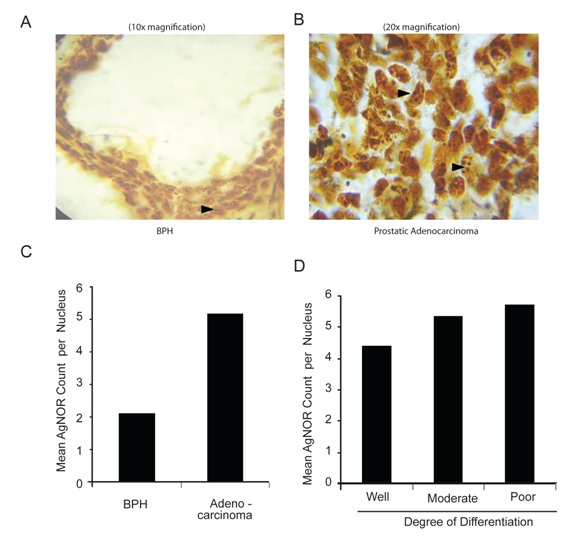
As the name suggests, the stain highlights the nucleolar regions. On an average, the number of silver stained nucleolar regions, i.e., the AgNOR Count per nucleus, was observed to be 2.1 in BPH samples [Table/Fig-4A and 4C]. The lowest value was 1.2 while the highest was 3.0 in BPH samples. On the contrary, the average AgNOR count per nucleus, in malignant specimens was found to be 5.15 [Table/Fig-4B and 4C]. The lowest value was found to be 3.8, while the highest value was found to be 7.1. Importantly, the average AgNOR count per nucleus was observed to be highest in poorly differentiated PCa specimens [Table/Fig-4D].
Argyrophilic Nucleolar Organiser Region (AgNOR) staining of the patient cohort. (A) AgNOR staining in benign prostatic hyperplasia (BPH). Shown is the 10x magnification of the section. (B) AgNOR staining in primary prostate cancers. Shown is the 20x magnification of the section. (C) Mean AgNOR count per nucleus for BPH and primary prostate cancers. (D) Mean AgNOR count per nucleus in varied degree of differentiation of primary prostate cancers.
Discussion
The current study attempts to excavate the combined potential of different histomorphological stains in prostatomegaly patients. The age demography of the patient cohort observed in this study is quite similar to the trend seen in previous studies [10]. The PAS staining of the patient samples didn’t differentiate between benign and malignant cases, as samples from both groups were observed to be PAS positive. In addition, the Gleason scoring didn’t correlate with the results from PAS staining, as three out of nine primary carcinomas were PAS negative even though they had a Gleason score which was relatively higher than the other six carcinoma samples. The Alcian blue stain was found to be relatively more specific to differentiate between benign and malignant lesions. Unlike weak positivity observed in non-neoplastic samples in previous studies, our BPH samples did not show any positivity [26, 28]. Moreover, acid mucin positivity has been reported in atypical adenomatous hyperplasia (AAH) and PIN due to histological similarities between AAH, PIN and PCa. Therefore, it may be a possibility that weak positivity seen in previous studies could be due to the presence of some pre-malignant cells. Since the patient cohort in this study had no cases of AAH or PIN, we could not verify these findings.
With respect to Alcian blue staining in prostate cancer samples, the findings from this study are in line with previous reports, which demonstrate the presence of acid mucin secretions to be more frequent in malignant versus benign prostate lesions [29]. However, the secretory capacity of synthesizing acid mucin is lost subsequently by malignant cells with higher grade, i.e., with higher degree of anaplasia. Previously, few studies [30,31] have observed the Alcian blue positivity due to staining of corpora amylacea and other substances that also take a slate blue hue of alcian blue staining. However, in the current study no such problem surfaced as corpora amylacea was distinguished from acid mucin due to its distinct location and slate gray appearance of the staining. However, it would be interesting to try Alcian Blue staining at different pH to differentiate the different types of mucin.
In the current study there is a statistically significant difference between AgNOR count per nucleus observed between benign and malignant lesions. Few studies in the past have demonstrated an overlap in the count with benign and malignant lesions [32,33] and found no prognostic role of AgNOR in prostate cancer [34]. Conversely, some studies have demonstrated AgNOR number to have a role in differentiating between benign, PIN and cancerous lesions [35,36]. Therefore, AgNOR count may act as an adjuvant to the other diagnostic markers and may provide a significant cell kinetic evaluation of prostatic lesions especially PIN with a parameter to provide a better definition. Unfortunately, no case of PIN was part of the cohort used in the current study to verify these observations.
Altogether, the results from the stains highlight individualistic potential of each stain, which fails to be of any diagnostic value on its own. However, if we combine the potential of all three stains together, there may be a possibility to turn the odds for a more accurate diagnosis of the prostatomegaly cases, especially the cases which lie in the grey zone and the pathologist finds it difficult to differentiate under the microscope.
[1]. Boehm JS, Hession MT, Bulmer SE, Hahn WC, Transformation of human and murine fibroblasts without viral oncoproteinsMol Cell Biol 2005 25(15):6464-74.PubMed PMID: 16024784. Pubmed Central PMCID: 1190359. Epub 2005/07/19 [Google Scholar]
[2]. Khanna A, Okkeri J, Bilgen T, Tiirikka T, Vihinen M, Visakorpi T, ETS1 mediates MEK1/2-dependent overexpression of cancerous inhibitor of protein phosphatase 2A (CIP2A) in human cancer cellsPLoS One 2011 6(3):e17979PubMed PMID: 21445343. Pubmed Central PMCID: 3062549. Epub 2011/03/30 [Google Scholar]
[3]. Khanna A, Bockelman C, Hemmes A, Junttila MR, Wiksten JP, Lundin M, MYC-dependent regulation and prognostic role of CIP2A in gastric cancerJ Natl Cancer Inst 2009 101(11):793-805.PubMed PMID: 19470954. Epub 2009/05/28 [Google Scholar]
[4]. Laine A, Sihto H, Come C, Rosenfeldt MT, Zwolinska A, Niemela M, Senescence sensitivity of breast cancer cells is defined by positive feedback loop between CIP2A and E2F1Cancer Discov 2013 3(2):182-97.PubMed PMID: 23306062. Pubmed Central PMCID: 3572190. Epub 2013/01/12 [Google Scholar]
[5]. Mathiasen DP, Egebjerg C, Andersen SH, Rafn B, Puustinen P, Khanna A, Identification of a c-Jun N-terminal kinase-2-dependent signal amplification cascade that regulates c-Myc levels in ras transformationOncogene 2012 31(3):390-401.PubMed PMID: 21706057. Epub 2011/06/28 [Google Scholar]
[6]. Khanna A, Regulation of Cancerous inhibitor of PP2A (CIP2A) by small molecule inhibitor for c-Jun NH2-Terminal Kinases (JNKs), SP600125, in Human Fibrosarcoma (HT1080) cellsF1000Research 2013 2013(2):174Epub 14 AUGUST 2013 [Google Scholar]
[7]. Khanna A, Bückelman C, Laine A, Ristimäki A, Visakorpi T, Westermarck J, 859 Constitutive DNA-damage signaling promotes cancer cell proliferation through Chk1-CIP2A pathwayEjc Supplements 2010 8(5):217-17. [Google Scholar]
[8]. Hanahan D, Weinberg RA, Hallmarks of cancer: the next generationCell 2011 144(5):646-74.PubMed PMID: 21376230. Epub 2011/03/08 [Google Scholar]
[9]. Finkel T, Serrano M, Blasco MA, The common biology of cancer and ageingNature 2007 16(448 (7155)):767-74.PubMed PMID: 17700693. Epub 2007/08/19 [Google Scholar]
[10]. Abate-Shen C, Shen MM, Molecular genetics of prostate cancerGenes Dev 2000 1 14(19):2410-34.PubMed PMID: 11018010. Epub 2000/10/06 [Google Scholar]
[11]. Brawer MK, Peehl DM, Stamey TA, Bostwick DG, Keratin immunoreactivity in the benign and neoplastic human prostateCancer Res 1985 45(8):3663-7.PubMed PMID: 2410099. Epub 1985/08/01 [Google Scholar]
[12]. Brewster SF, Oxley JD, Trivella M, Abbott CD, Gillatt DA, Preoperative p53, bcl-2, CD44 and E-cadherin immunohistochemistry as predictors of biochemical relapse after radical prostatectomyJ Urol 1999 161(4):1238-43.PubMed PMID: 10081877. Epub 1999/03/19 [Google Scholar]
[13]. Sherwood ER, Berg LA, Mitchell NJ, McNeal JE, Kozlowski JM, Lee C, Differential cytokeratin expression in normal, hyperplastic and malignant epithelial cells from human prostateJ Urol 1990 143(1):167-71.PubMed PMID: 1688457. Epub 1990/01/01 [Google Scholar]
[14]. Bui M, Reiter RE, Stem cell genes in androgen-independent prostate cancerCancer Metastasis Rev 1998 17(4):391-9.PubMed PMID: 10453283. Epub 1999/08/24 [Google Scholar]
[15]. Maitland NJ, Collins AT, Prostate cancer stem cells: a new target for therapy. Journal of clinical oncologyJournal of the American Society of Clinical Oncology 2008 Jun 10 26(17):2862-70.PubMed PMID: 18539965 [Google Scholar]
[16]. Tindall DJ, Rittmaster RS, The rationale for inhibiting 5alpha-reductase isoenzymes in the prevention and treatment of prostate cancerJ Urol 2008r 179(4):1235-42.PubMed PMID: 18280514. Pubmed Central PMCID: 2667246. Epub 2008/02/19 [Google Scholar]
[17]. Canil CM, Tannock IF, Should bisphosphonates be used routinely in patients with prostate cancer metastatic to bone?J Natl Cancer Inst 2002 94(19):1422-3.PubMed PMID: 12359844. Epub 2002/10/03 [Google Scholar]
[18]. Nemeth JA, Yousif R, Herzog M, Che M, Upadhyay J, Shekarriz B, Matrix metalloproteinase activity, bone matrix turnover, and tumor cell proliferation in prostate cancer bone metastasisJ Natl Cancer Inst 2002 94(1):17-25.PubMed PMID: 11773278. Epub 2002/01/05 [Google Scholar]
[19]. Bissell MJ, Le Beyec J, Anderson RL, Prostate cancer in bone: importance of context for inhibition of matrix metalloproteinasesJ Natl Cancer Inst 2002 94(1):4-5.PubMed PMID: 11773268. Pubmed Central PMCID: 3027556. Epub 2002/01/05 [Google Scholar]
[20]. Khurd P, Bahlmann C, Maday P, Kamen A, Gibbs-Strauss S, Genega EM, Computer-Aided Gleason Grading of Prostate Cancer Histopathological Images Using Texton ForestsProc IEEE Int Symp Biomed Imaging 2010 :636-9.PubMed PMID: 21221421. Pubmed Central PMCID: 3017375. Epub 2011/01/12 [Google Scholar]
[21]. Gleason DF, Mellinger GT, Prediction of prognosis for prostatic adenocarcinoma by combined histological grading and clinical stagingJ Urol 1974 (111)(1):58-64.PubMed PMID: 4813554. Epub 1974/01/01 [Google Scholar]
[22]. Gaeta JF, Englander LC, Murphy GP, Comparative evaluation of National Prostatic Cancer Treatment Group and Gleason systems for pathologic grading of primary prostatic cancerUrology 1986 27(4):306-8.PubMed PMID: 3962053. Epub 1986/04/01 [Google Scholar]
[23]. Thompson IM, Ankerst DP, Chi C, Lucia MS, Goodman PJ, Crowley JJ, Operating characteristics of prostate-specific antigen in men with an initial PSA level of 3.0 ng/ml or lowerJAMA 2005 294(1):66-70.PubMed PMID: 15998892. Epub 2005/07/07 [Google Scholar]
[24]. Presti JC, Jr., Hovey R, Carroll PR, Shinohara K, Prospective evaluation of prostate specific antigen and prostate specific antigen density in the detection of nonpalpable and stage T1C carcinoma of the prostateJ Urol 1996 156(5):1685-90.PubMed PMID: 8863571. Epub 1996/11/01 [Google Scholar]
[25]. Kufe DW, Mucins in cancer: function, prognosis and therapyNat Rev Cancer 2009 9(12):874-85.PubMed PMID: 19935676. Pubmed Central PMCID: 2951677. Epub 2009/11/26 [Google Scholar]
[26]. Mathur SK, Gupta S, Marwah N, Narula A, Singh S, Arora B, Significance of mucin stain in differentiating benign and malignant lesions of prostateIndian J Pathol Microbiol 2003 46(4):593-5.PubMed PMID: 15025351. Epub 2004/03/18 [Google Scholar]
[27]. Crocker J, Boldy DA, Egan MJ, How should we count AgNORS? Proposals for a standardized approachJ Pathol 1989 158(3):185-8.PubMed PMID: 2475599. Epub 1989/07/01 [Google Scholar]
[28]. Grignon DJ, O’Malley FP, Mucinous metaplasia in the prostate glandAm J Surg Pathol 1993 17(3):287-90.PubMed PMID: 7679558. Epub 1993/03/01 [Google Scholar]
[29]. Mathur SK, Gupta S, Marwah N, Narula A, Singh S, Arora B, Significance of mucin stain in differentiating benign and malignant lesions of prostateIndian Journal of Pathology & Microbiology 2003 46(4):593-5.PubMed PMID: 15025351. Epub 2004/03/18 [Google Scholar]
[30]. Franks LM, O’Shea JD, Thomson AE, Mucin in the Prostate: A Histochemical Study in Normal Glands, Latent, Clinical, and Colloid CancersCancer 1964 17:983-91.PubMed PMID: 14202599. Epub 1964/08/01 [Google Scholar]
[31]. Hukill PB, Vidone RA, Histochemistry of mucus and other polysaccharides in tumors. II. Carcinoma of the prostateLab Invest 1967 16(3):395-406.PubMed PMID: 4225797. Epub 1967/03/01 [Google Scholar]
[32]. Lloyd SN, Johnson CP, Brown IL, Kirk D, Nucleolar organizer regions in benign and malignant prostatic diseaseHistopathology 1991 18(5):449-52.PubMed PMID: 1715842. Epub 1991/05/01 [Google Scholar]
[33]. Deschenes J, Weidner N, Nucleolar organizer regions (NOR) in hyperplastic and neoplastic prostate diseaseAm J Surg Pathol 1990 14(12):1148-55.PubMed PMID: 2252105. Epub 1990/12/01 [Google Scholar]
[34]. Contractor H, Ruschoff J, Hanisch T, Ulshofer B, Neumann K, Schultze-Seemann W, Silver-stained structures in prostatic carcinoma: evaluation of diagnostic and prognostic relevance by automated image analysisUrol Int 1991 46(1):9-14.PubMed PMID: 1708924. Epub 1991/01/01 [Google Scholar]
[35]. Kawase N, Shiokawa A, Ota H, Saitoh T, Yoshida H, Kazama K, Nucleolar organizer regions and PCNA expression in prostatic cancersPathol Int 1994 44(3)(213-22)PubMed PMID: 7517763. Epub 1994/03/01 [Google Scholar]
[36]. Nakae S, Nakamura T, Ikegawa R, Yoshioka H, Shirono J, Tabuchi Y, Evaluation of argyrophilic nucleolar organizer region and proliferating cell nuclear antigen in colorectal cancerJ Surg Oncol 1998 69(1):28-35.PubMed PMID: 9762888. Epub 1998/10/08 [Google Scholar]