Multiple Ileal Perforations Following Dilatation and Evacuation (D&E) for Missed Abortion
Haritha Sagili1, Verghese Yeldho2, Dasari Papa3
1 Assistant Professor, Department of Obstetrics and Gynaecology, JIPMER, Pondicherry, India.
2 Senior Resident, Department of Surgery, JIPMER, Pondicherry, India.
3 Professor, Department of Obstetrics and Gynaecology, JIPMER, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Haritha Sagili, 12, 1st Cross, Saradambal Nagar, Pondicherry-605005, India.
Phone: 9489390630,
E-mail: harithasagili@gmail.com
Abortion, Dilatation and Evacuation (D&E), Bowel injury
Sir,
Miscarriage has traditionally been treated by surgical evacuation, on the assumption that any retained tissue increases the risk of infection and haemorrhage. One of the serious risks of surgical evacuation is uterine perforation (upto 5 in 1,000 women) [1]. Over the last decade, the management of abortion has become medical to reduce the life threatening complications associated with surgical techniques. But still medical management is not being followed by every practising obstetrician or surgeon. A 25-year-old married lady presented to our hospital with fever, abdominal pain and vomiting for two days following dilatation and evacuation for missed abortion at eight weeks of gestation at a private hospital. Abdomen was tender and guarding was present. On laparotomy, there was a 5mm perforation on the anterior wall of the uterus near the fundus [Table/Fig-1] and multiple (6) ilealperforations measuring 0.5-1cm each [Table/Fig-2].
5mm perforation on the anterior wall of the uterus near the fundus on laparotomy
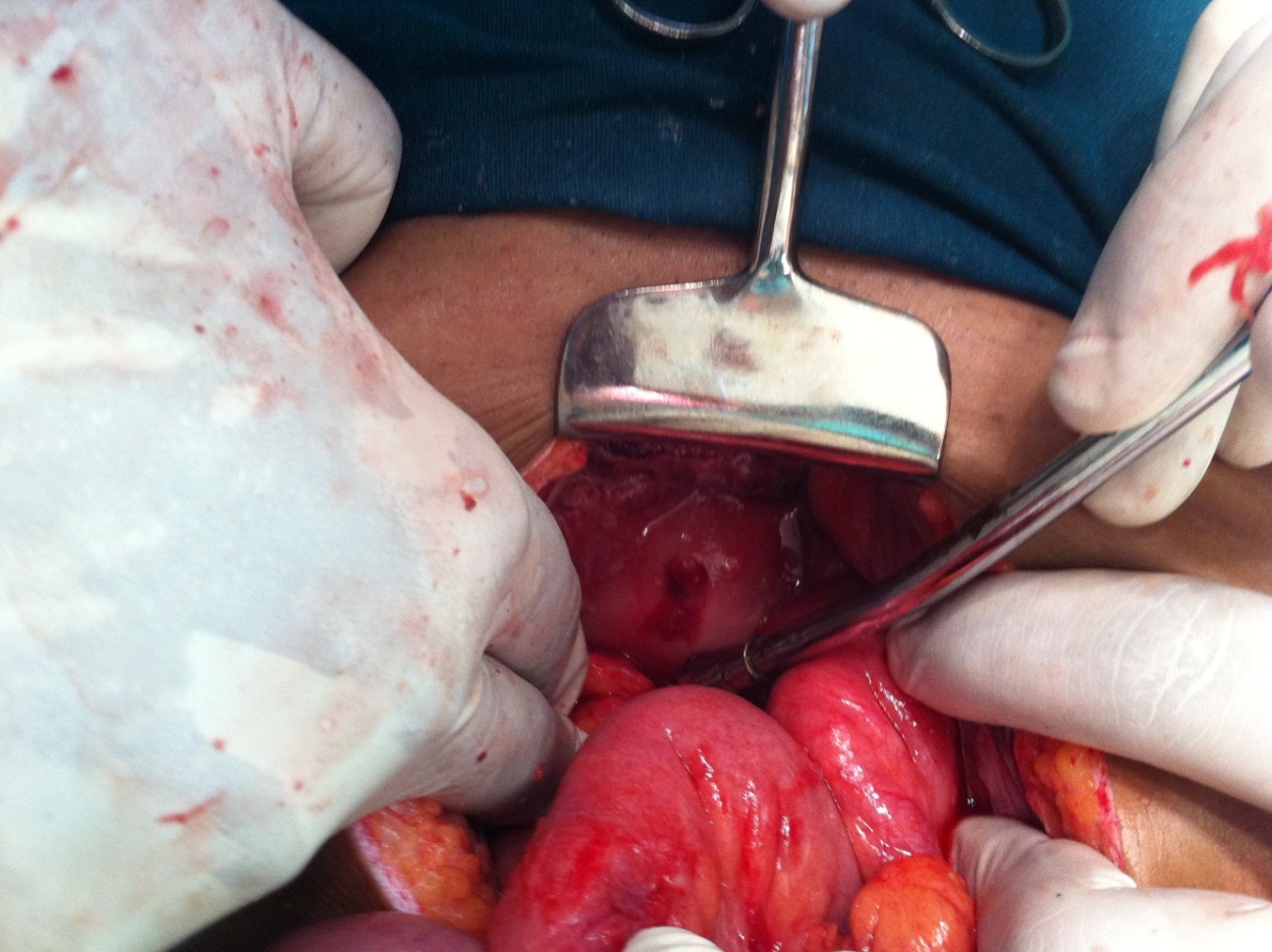
Multiple (6) ilealperforations measuring 0.5-1cm each on laparotomy

Uterine perforation was freshened and approximated with vicryl. Segmental resection and anastomosis of 8 cm of the ileum was performed. Post-operatively she had febrile spikes which subsided on the 4th day; peritoneal fluid aspirate culture showed E.Coli which resolved with appropriate antibiotics. On 10th day post-operation, she was discharged home. She continued to have pain in the abdomen which was managed as acid peptic disease on outpatient basis. She required admission once when she presented to casualty 46 days after discharge from hospital with upper abdominal pain and vomiting and a provisional diagnosis of adhesive intestinal obstruction was made. Her symptoms subsided with conservative treatment. The present day treatment of abortion is medical management [2]. Surgery has a limited role. The aim of the surgical procedure should be to treat an incomplete or missed miscarriage, or retained placental tissue not responsive to timely medical management.
[1]. Royal college of Obstetricians and Gynaecologists (RCOG). Surgical Evacuation of the Uterus for Early Pregnancy Loss (Consent Advice 10). June 2010 [Google Scholar]
[2]. National Institute of Clinical Excellence (NICE). Ectopic pregnancy and miscarriage (CG154). December 2012 [Google Scholar]