Multiple Giant Cell Tumours of Tendon Sheath: A Rare Occurrence
Smita Charandas Pathade1, Ramkumar Kurpad2, Mohammed Tauheed3
1 Assistant Professor, Department of Pathology, DM WIMS, Wayanad, Kerala, India.
2 Professor and Head, Department of Pathology, DM WIMS, Wayanad, Kerala, India.
3 Assistant Professor, Department of Orthopaedics, DM WIMS, Wayanad, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Smita Charandas Pathade, Assistant Professor, Department of Pathology, DM WIMS, Nassera Nagar, Meppadi (P.O), Wayanad, Kerala,India-673577
Phone: 8111881085,
E-mail: dr.smitajadhav2005@yahoo.com
Giant Cell Tumours Of Tendon Sheath (GCTTS) are the second most frequent soft tissue tumours affecting the hand with an overall incidence of 1 in 50,000 individuals. These tumours are usually localized and solitary, with multiple GCTTS occurring rarely. Multi-centric origin is considered unusual and very few cases of multiple GCTTS have been reported till date. Here, we report a rare case of a 26-year-old female who presented with multiple painless swellings on palmar aspect of little finger of right hand since six months. Clinical diagnosis of Dupuytren’s contracture was given. Intraoperative examination revealed multiple separate nodules, firmly attached to the flexor tendon synovial sheath. Histopathology showed features of GCTTS.
Giant cell tumour, Colony stimulating factor, Dupuytren’s contracture
Case Report
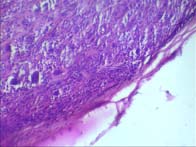
A 26-year-old female, presented with history of multiple painless swellings on palmar aspect of right hand, progressively increasing in size since last 6 months. There was no history of preceding trauma. On examination, there were 5 different swellings on palmar aspect of right hand. There were three firm nodules 1x1 cm each, first at region of distal phalanx, second near middle phalanx and third near proximal phalanx of little finger. Apart from these, there was a 2x2 cm nodule at 5th metacarpal head region and a 3x3 cm multinodular swelling occupying mid palm. Clinical diagnosis of Dupuytren’s contracture was given and patient was posted for surgery. Under local anesthesia, nodules were excised by giving multiple incisions. All nodules were separate without any connection between them and were seen tightly attached to the synovial sheath of the flexor tendons. We received the specimen in histopathology section in the form of multiple - about 14, round to oval, firm to hard tissue bits ranging in size from 1.5x0.5x0.5 cm to 2x0.8x0.7 cm. Cut-sections showed mottled whitish and yellowish areas [Table/Fig-1]. Histopathological sections [Table/Fig-2,3&4] from the tumour showed an encapsulated lesion comprising of spindle cells in whorls, admixed with giant cells. Focal infiltration by foamy macrophages and areas of hyalinization were also seen. Mitotic figures and apoptotic figures were absent. Diagnosis of multiple GCTTS was given. Postoperatively and on follow-up visit, patient had full range of movements of all fingers.
Gross appearance of the tumour in the form of multiple nodules

H&E stained sections showing, encapsulated tumour with giant cells
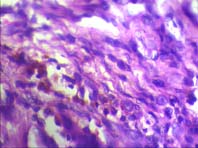
H&E stained sections showing spindle cells with pigment laden macrophages and few lymphocytes.
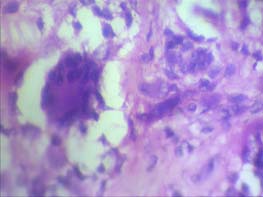
H&E stained sections showing giant cell with surrounding hypocellular area.
Discussion
GCTTS is a slowly progressive benign tumour arising from synovial cells of tendon sheaths. Chassaignac first described the soft tissue mass in 1852, as fibrous xanthoma. This tumour usually occurs as a palpable, subcutaneous, solitary, slow-growing, localized and painless mass in the hand. Multiple lesions are extremely rare [1,2]. Present case report highlights the occurrence of multiple GCTTS in the hand of a 26-year-old female.
GCTTS is classified into localized nodular type and diffuse type. Diffuse form, even though uncommon in hand, needs to be differentiated from multiple GCTTS. Diffuse form is hypercellular with few giant cells, while localized form is relatively hypocellular with numerous giant cells. Another new classification of GCTTS includes classifying lesions into Type I (single tumour, which is round and multi-lobulated) and Type II (two or more distinct Tumours which are not joined together). This classification helps in predicting recurrence as satellite lesions are missed often in Type II, if microscopic excision is not done [2,3]. The nature of the lesion is still controversial. Multiple theories have been suggested for the explanation of etiopathogenesis which include inflammatory process, localized lipid metabolism disturbance, osteoclastic proliferation, trauma, infection, vascular disturbances, etc. [4]. Recent studies have raised the idea of GCTTS being a neoplastic process, a hypothesis supported by the presence in the lesion of clonal chromosomal translocation, t(1;2)(p13;q37), which fuses colony stimulating factor (CSF1) coding sequences to the promoter of the collagen type VI alpha-3 gene. As a result, the tumour cells overexpress CSF1, a chemoattractant for macrophages, which infiltrate the tumour in large numbers [5]. Mutation of gene nm23 is supposed to be associated with increased rate of recurrence. Few cases of malignant GCTTS have also been documented [1,3].
A majority of GCTTS are found in patients in 3rd and 4th decade of their life. The female to male ratio is 3:2. GCTTS most commonly presents in a digit of the hand. However, it may also be rarely present in the palm, wrist, foot, knee, ankle, elbow or hip. This tumour usually occurs as a solitary mass in a finger, simultaneous multiple lesions in hand are very rare [1,6,7]. A few case reports and reviews have identified the presence of multiple GCTTS. Park JW, et al., reported a case in a 33-year-old male with 2 separate GCTTS that developed simultaneously in the same thumb [6]. Similarly Talvinder Singh et al., reported multifocal GCTTS at different sites in a finger [7]. Case series conducted by different authors have reported multiple GCTTS in, 1/207 (0.4%), 1/118 (0.8%) and 3/56 (5.3%) patients [1]. Multiple bilaterally symmetrical, as well as, asymmetrical GCTTS are described in literature [1,2]. Very few cases of multiple GCTTS have been reported from India.
Conclusion
GCTTS, even though uncommon, should be considered in the differential diagnosis of multi-focal subcutaneous tumours. In view of recurrence of GCTTS and a possible propensity for malignancy, a high index of suspicion should be rendered while dealing with multiple swellings of hand, so that a pre-operative diagnosis facilitates planning of surgery in a better way.
[1]. Altaykan A, Yildiz K, Hapa O, Cukur S, Multifocal giant cell tumour of the tendon sheath occurring at different localizations of the same tendon of a finger: a case report and review of the literatureEklem Hastalik Cerrahisi 2009 20(2):119-23. [Google Scholar]
[2]. Akisue T, Yamomoto T, Kawamoto T, Hitora T, Marui T, Nakatani T, et al. Multicentric localized giant cell tumour of tendon sheath. SICOT online report E059. Available at: http://www.sicot.org/resources/File/IO_reports/05-2004/E059.pdf [Google Scholar]
[3]. Suresh SS, Zaki H, Giant cell tumour of tendon sheath: Case series and review of literatureJ Hand Microsurg 2010 2(2):67-71. [Google Scholar]
[4]. Kadi AA, Salati SA, Arkoubi AY, Giant cell tumour of tendon sheath: a reviewNigerian Journal of Plastic Surgery 2012 8(1):19-25. [Google Scholar]
[5]. Rosenberg AE, Bones, joints and soft tissue Tumours. In: Vinay K, Abul KA, Nelson, Jon CA, EditorsRobbins and Cotran pathologic basis of disease 2012 PhiladelphiaElsevier:1247 [Google Scholar]
[6]. Jong WP, Multiple separated giant cell Tumours of the tendon sheath in a thumbJournal of the American Academy of Dermatology 2006 54(3):540-42. [Google Scholar]
[7]. Talvinder S, Saqib N, Adrian WS, Multiple localized giant cell tumour of the tendon sheath affecting a single tendon: a very rare case report and review of recent casesHand Surgery 2011 16(3):367-69. [Google Scholar]