Clavicular injury is common in active and younger age-group with male preponderance (male female ratio is 2:1). It accounts for 2.5 to 5 percent of all trauma. These fractures are mostly displaced and middle one-third is the most common type (80%) of all clavicular fractures [1,2].
Time-honored treatment of fracture midshaft clavicle has been in the form of a simple sling, figure of eight clavicular brace, crepe bandage as a figure of eight, etc. But most of the conservative treatments need regular adjustment, are cumbersome and inconvenient to the patients.
Purpose of this study was to analyze the outcome of surgically treated displaced fracture midshaft clavicular fracture using Intra-medullary fixation by titanium elastic nail.
Materials and Methods
It is a prospective study carried out between 2006 to 2012, after approval from institutional ethics committee. We present a series of seventy nine enrolled cases of midshaft clavicular fracture who were subjected to Intra-medullary fixation with the average nail diameter of 2.5 to 3 mm titanium elastic nail system by the closed/open reduction method under Image intensifier control. Male to female ratio was 68:11. Right to left side involvement was 48:31 in which right-sided injury involved 41 males and 7 females, while left-sided injury included 27 males and 4 females.
Ten patients (12.6%) sustained injury in sport activity, 28 patients (35.4%) got road traffic accident and rest 41 (51.8%) fell on the ground and injured indirectly. Mean age was 48 years (SD = 7.2) (Range of 26-50 years).
Our study included all midshaft displaced clavicular traumatic fracture type A (simple fracture two segment) and B (fracture with bending wedge) according to Orthopaedic Trauma Association (OTA) classification. With age-group between 16 years to 60 years and who desired for early return to work, healing with no loss of length or strength, with no contraindication to general anaesthesia, impending open fracture due to tenting of skin, polytraumatic patient, floating shoulder, and cosmetic-oriented individuals were included. We excluded open fracture, pathological fracture and those patients who were not ready for operative procedure. We did not include fracture of more than three weeks and midshaft clavicular fracture type C. In communited (Type-C) fracture telescoping and shortening is a major problem and in these fracture thinner diameter’s unlocked nail lacks to control axial length and rotation. So, Type C fracture is not suitable candidate for nailing. All patients informed for usual surgical risks and additional incision for open reduction. Injury surgery interval was on average 5 days (range: 2-11 days). Fifty seven patients categorised as type A and twenty two cases classified as type B fracture.
Technique: Under general anaesthesia, patients positioned in supine beach chair position with folded towel over medial border of affected shoulder. Entry portal was made by awl at medial end of clavicle at inferior border under image intensifier. Titanium nail was bent at tip about 15 degree to facilitate insertion. T- Handle was used to push and rotate the nail into the medullary cavity under fluoroscopic control until it reaches the fracture site. A closed reduction was tried directly or by holding both ends by small clamps or by using unicortically placed joy sticks (schanz pin). If fails then a small nick incision was made to just facilitate nail in the distal end of clavicle. After adequate engagement in lateral segment, nail cut after little bent on medial side and buried under skin.
Post-operatively patient’s limb kept in sling, allowed to move his/her limb as much they could tolerate and next day all patients got discharged. Up to four-weeks forward flexion more than 90 degree (causes rotation) and overhead movements were not permitted, then all restrictions abolished. While we gave post-operatively sling for four-weeks to our patients, they were able to do little work, and it did not include regular adjustment and much discomfort (especially in females) like conservative management.
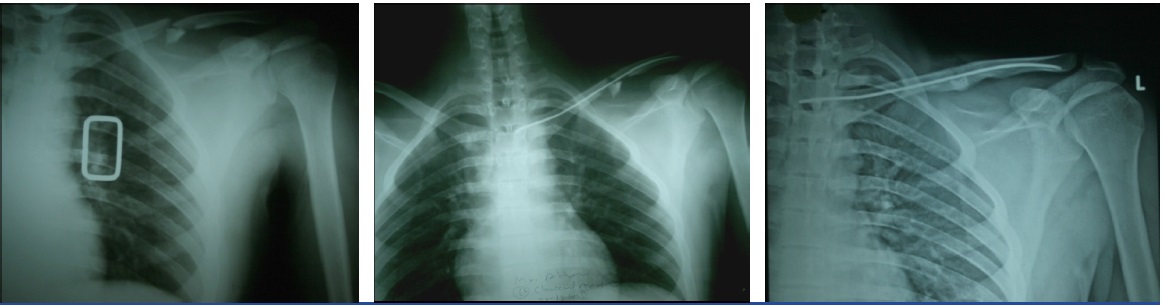
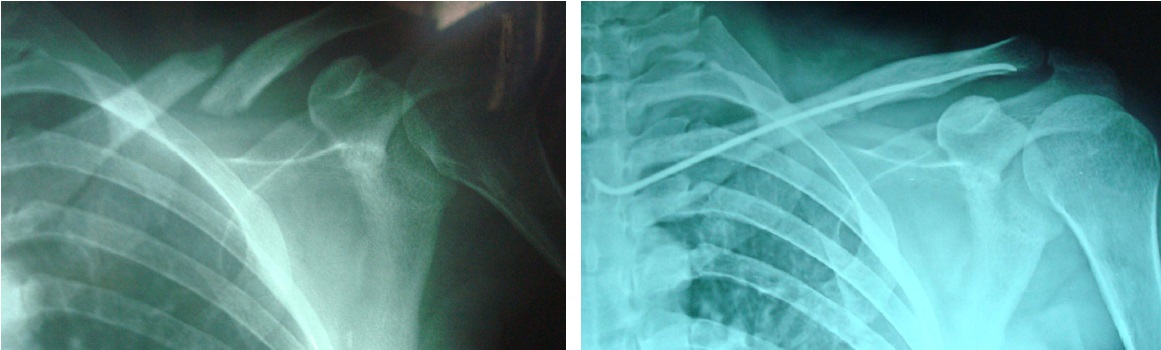
Patients called up for follow-up at four, eight and twelve weeks then onwards accordingly. After clinical and radiological union, they were called up after sixth, ninth and at 12 months. Radiographic course of a displaced midshaft clavicular fracture is depicted in the [Table/Fig-1 and 2].
Radiological course of titanium elastic nail in OTA type B fracture of displaced midshaftclavicular fracture
Radiological course of titanium elastic nail in another case of displaced midshaftclavicular fracture
Assessment of the patient’s outcomes were done by clinico-radiological evaluation, evaluation of shoulder function by Constant-Murley-Score (CMS) and evaluation of period of disability [3].
Results
The procedure not only allowed the clavicle to regain length and stability, but also allowed the patients to return to work at the earliest possible with quick relief from pain, after a shorter hospital stay.
Since six patients out of 79 patients could not be followed, our results are based on 73 patients. In 55 patients, (75%) we could achieve closed reduction and internal fixation under fluoroscopic control. In 18 patients, (25%) we achieved reduction by open reduction and holding the fracture fragments together while passing the nail.
Overall fifteen patients (20.5%) encountered minor complications. We faced delayed union in three cases (4.1%). In two cases (2.7%) iatrogenic perforation of lateral cortex occurred but nailing completed successfully in these cases. Seven patients (9.5%) complained for skin irritation and three patients (4.1%) had a wound (superficial infection) at the medial end of clavicle at the nail insertion site and after nail removal (done earlier after three month of full union), healed by secondary intention. There were no major complications noted i.e. non union or revision surgery. The nail was removed by a single nick under local anaesthesia at average of six months (after achieving full clinico-radiological union).
Average time taken for full clinical and radiological union was nine weeks (with minimum six weeks to maximum eleven weeks). Since nail was in-situ, no pain and callus formation (without breaching) was taken as criteria for union. Time taken for fully functional recovery (time of functional disability) was 35±7 days in all patients except in two cases of floating shoulder and one case of a poly-traumatic patient, in which it was 50 days. Follow-up period ranged between 9 months and 24 months with an average of 18 months. Average Constant-Murley-Score after assessment of shoulder function was 96.8. Statistical detail of Constant-Murley-Score is Max=100, Min=92, SD=2.3, Sample variance=5.67, Standard error= 0.27, Skewness= -0.58 and the study was considered significant
(p= < 0.05).
Discussion
First report of conservative management of clavicular fracture goes to Egypt, 17th century B.C. [4]. Since long time in orthopaedics, there has been a “benign neglect” approach for this fracture.
Classical indications of using surgical measure in fracture clavicle are confined to open fracture, impending open fracture, neurovascular compromise, floating shoulder, polytraumatic patients and symptomatic nonunion. Conservatively treated fracture clavicle most of the time heals successfully, but in true sense achieving patient’s satisfaction is genuine goal of treatment.
Traditionally (since Hippocrates), midshaft clavicular fracture have been managed conservatively with this assumption that it does not hamper shoulder function [5] and even malunion has only radiographic means, but now it is apparent that, it has an impact on orthopaedic, neurologic, and cosmetic aspect too. Study of Nowak et al., [6], which was carried out over 208 patients and followed-up to ten years for sequelae, found that 46% patients were symptomatic. Displacement and comminution are the strongest predictor, angulations have no effect on cosmetic defect and outcome is not influenced by location and shortening (it only influenced cosmetic defect) [6]. Another prospective cohort study carried out in Malaysia to know the clinical outcome on non-surgically treated clavicle after six month of follow-up concluded that displacement more than 21 mm, shortening of more than 15 mm, nonunion and malunited fracture are indication of surgical intervention [7]. Ledger et al., [8], also emphasized that short malunion limits the shoulder function so recommended open reduction and/ internal fixation to prevent shortening. Shortening (≥15 mm) increases 10.7 degree at sternoclavicular joint angulations and 6.1 degree improvement in scapular version, so tethering affect occur over scapula leading to shoulder dysfunctions [8]. By using Biodex isokinetic assessment with constant and Murley scoring system for Allman type 1 conservatively treated clavicle, Flavin et al., found that after three years of follow-up there was 74% malunion, 3% nonunion, average angulation 13.9 degree and shortening of 15 mm which hampered the shoulder’s isokinetic function significantly and led patients symptomatic [9].
Anatomically aligned united midshaft fracture clavicle has shown superiority over conservatively treated clavicle, but it needs mulling over repercussion of surgical intervention. Various surgical treatment options are mentioned in literature for displaced midshaft clavicle, but plate and Intra-medullary nail osteosynthesis are more discussed and preferred modality of treatment.
Plate osteosynthesis is most discussed and its long-term experience in literature is mentioned. Biomechanically verdict is that, it is a rigid fixation so early rehabilitation, technically less demanding but practically even while it is most exercised, complications are still more than nail fixation. Infection, nonunion, plate breakage, plate loosening, refracture are the well-documented pitfalls in 23% of cases in the study done by Bostman et al., [10]. Incisional numbness, cosmetic unhappiness, scar related pain, metal causing discomfort were encountered drawbacks of plate osteosynthesis in retrospective comparative study of Thyagarajan et al., [11].
Original technique of intra-medullary fixation given by Boehme et al., was open reduction and internal fixation in nonunion of clavicle by Hagie pin and autogenous bone grafting and concluded several advantage over other treatments [12]. Threaded Steinmann pin, Rush pin, Kirschner wire, cancellous screw etc. had also been reported over time as an intra-medullary fixation device with relative pros and cons [13–16].
Every modality of surgical intervention has own pros and cons. Irrespective of the surgical treatment (plate versus intra-medullary fixation) the studies of Ferran et al., and Liu et al., could not draw significant difference in functional outcome [17,18]. But in the aspect of complications, titanium elastic nail showed superiority over plating. Wijdicks et al., in their study found that plating is associated with higher refracture, major revision surgery and implant failure in comparison to elastic stable nail [19].
In study of Wu et al., union rate, among surgically treated nonunion of clavicle, is better by intra-medullary fixation 89%, in comparison to plating which is 81% [20]. In our series we did not face the problem of nonunion, which strengthens the fact that nonunion can be avoided by intra-medullary nailing. Titanium elastic intra-medullary nailing is a promising surgery with excellent functional outcome. [Table/Fig-3] showing comparative results of different studies in term of shoulder function [21–23], reliability, safer percutaneous minimal invasive procedure with rapid healing tendency and fewer complications in contrast to plate osteosynthesis.
Showing comparisons of result of titanium elastic nail for fracture mid shaft clavicle in contest of shoulder function.
| S. No | Study | Shoulder Function In Term of Constant-Murley-Score |
|---|
| 1 | F. Hartmann et al., [21] | CONSTANT-MURLEY-SCORE was 95.3 ± 3.9. |
| 2 | Yun-feng Chen et al., [22] | CONSTANT-MURLEY-SCORE was 95.2 (range 86.5–97.0). |
| 3 | Zhang W et al., [23] | CONSTANT-MURLEY-SCORE was (97.0 +/- 4.2). |
| 4 | Our study. | CONSTANT-MURLEY-SCORE 96.8. (Max=100, Min=92). |
Repercussion of clavicle surgery also is implant removal, so the necessity of second operation. In case of intra-medullary fixation it is the standard protocol to remove implants. Imaginary complications have been documented due to implant migration like Kirschner wire used to fix midshaft clavicular fracture have been found in opposite orbit causing exophthalmos and steinman pin have been found in expectoration of patients [24,25].
Due to three point bony fixation, titanium elastic nail circumvents these problems and gives rotational stability, even then, it is advised to remove it timely. In contrast to it, plate fixation needs less implant removal but patients discomfort have been reported. Neither is it an out patients department procedure, nor can it be done under local anaesthesia and it may also need abstinence from sport activities. In our series result of Shoulder function (as assessed by Constant-Murley-Score) was better in comparison to conservatively managed, displaced fracture of clavicle [11,26].
Conclusion
Even inadequate and noncompliant treatment protocol, sometimes, unites clavicle fracture uneventfully. But, most crucial part of the treatment is patient’s counselling for the expected result in perspective of displaced midshaft clavicular fracture.
Our patients displayed pleasing attitude, bereft of pain and weakness, and were cosmetically satisfied. In severely comminuted fracture where chances are of significant shortening and telescoping, plating is preferred. The author feels that this method is promising and avoids the complication listed in studies of other method of internal fixations of clavicle. We are satisfied with intra-medullary fixation due to affordability, load sharing property, shorter hospital stay, quick pain relief, early return to work and easy implant removal under local anaesthesia as an out patient department procedure.
Consent
Consent of the patient has been taken, that his photo and detail can be published in case report.
Author’s Contributions
Pankaj K Mishra wrote the manuscript, maintained the patient’s record, and did surgery. Anuj Gupta reviewed the manuscript and assisted in surgery. Suresh Chandra Gaur is the main surgeon who was present in every surgery and guided us at every aspect.