Is Renal Osteodystrophy a Neglected Entity?
Ramesh Narula1, Yasir Salam2, Kusum Narula3
1 Associate Professor, Department of Orthopedics, Rohilkhand Medical College, Bareilly U.P-243006, India.
2 Assistant Professor, Department of Orthopedics, Rohilkhand Medical College, Bareilly U.P-243006, India.
3 Demonstrator, Department of Community Medicine, Rohilkhand Medical College, Bareilly U.P-243006, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ramesh Narula, Associate Professor, Department of Orthopedics, Rohilkhand Medical College, Bareilly U.P-243006, India.
Phone: 09719740866,
E-mail: rameshnarula55@gmail.com
Sir,
Renal Osteodystrophy (ROD) is the term given to the bone changes which accompany chronic renal failure [1].
We here by present a case of a middle aged female who was suffering from renal disease from more than eight years and was being treated for Ankylosing Spondylitis as co morbidity. Thirty two- year-old, female presented to our orthopedic outpatient department with chronic backache and stiffness of back and hip joints from eight years. She had many prescriptions of various physicians to show she is chronically ill. HLA-B27 report was negative. Her family history was not significant and menstrual history was normal. There was no history of trauma, fever, night sweats, night pains, loss of appetite, loss of weight, morning stiffness, involvement of smaller joints of hand and feet, bowel disturbances, recurrent UTI’s, jaundice, breathlessness, cough with haemoptysis.
On examination, all movements of her back were restricted, especially flexion. Both hips had fixed flexion deformity of 15 degrees and all movements were restricted. She was unable to sit cross legged and squat. Her cardiovascular, respiratory and abdominal examinations were normal. Subsequently she was admitted for evaluation.
Patient was investigated for–hemoglobin, total and differential leukocyte counts, ESR, random blood sugar, S.G.P.T., RA- Factor, C-reactive protein, serum uric acid, blood urea, serum creatinine, serum calcium, serum phosphorus, serum alkaline phosphatase, urine calcium and phosphorus estimation. She was found to have deranged renal function, as blood urea and serum creatinine were raised to 168 mg% and 4.0mg% .Her serum alkaline phosphatase was raised to 311 I.U. /LIT. Her serum calcium was low 7.0 mg% and phosphate normal 6.0 mg%.
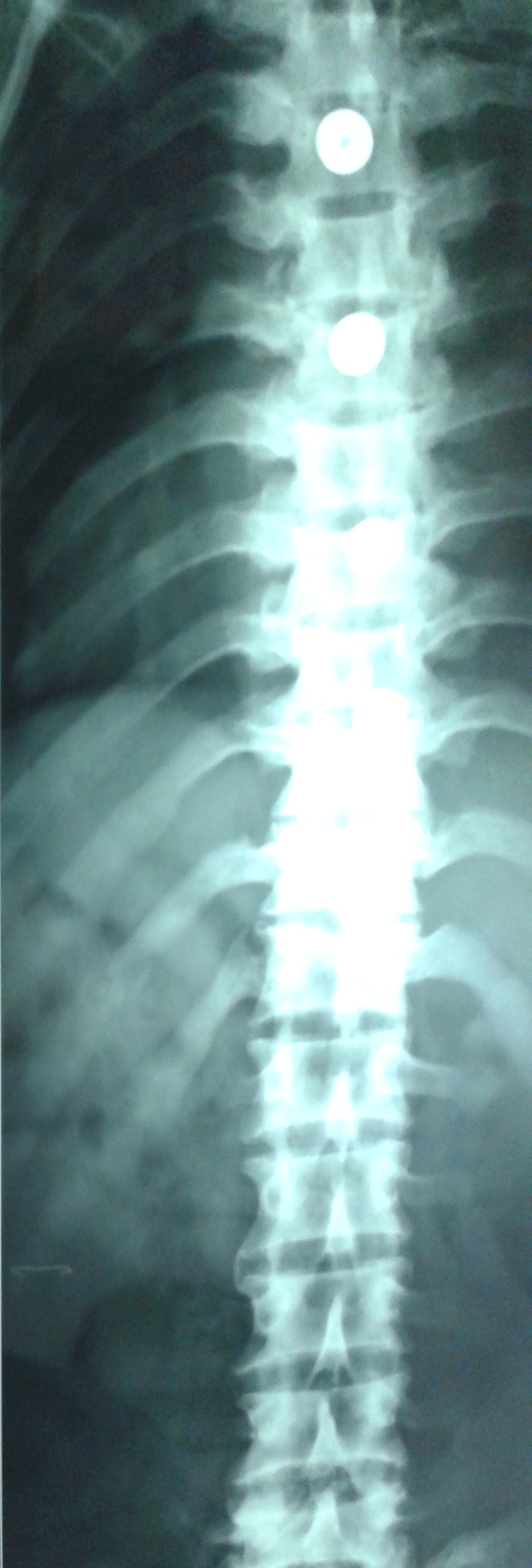
Her X-ray dorsolumbar spine AP/Lateral views revealed generalized increase in density (osteosclerosis) with calcification of anterior longitudinal ligament [Table/Fig-1]. X-ray Pelvis showed triradiate pelvis with protrusio acetabuli [Table/Fig-2]. Clinicoradiological diagnosis of Renal Osteodystrophy was made. Patient was then made to undergo ultrasound of KUB region which revealed conjoined kidneys.
X-ray Dorsolumbar spine AP and lateral views showing generalized increase in density with calcification of anterior longitudinal ligament

X-ray pelvis AP view showing triradiate pelvis with bilateral protrusio acetabuli
Moriniere P, et al., in their study on disappearance of aluminic bone disease in a long term asymptomatic dialysis population have stated that Osteomalacia is a common component of bone disease in patients with end stage renal disease, although its prevalence is decreasing [2]. The disorder is characterized by low rates of bone turnover, a mineralization defect, and an accumulation of unmineralized osteoid (bone matrix). The type of Osteomalacia differs from that caused by Vitamin D deficiency, and the role of 1, 25-dihydroxy-cholecalciferol deficiency in Osteomalacia associated with end stage renal disease is unclear [3]. X-ray pelvis AP view in our patient revealed triradiate pelvis with bilateral protrusio acetabuli changes which are commonly seen in Osteomalacia.
According to the study of Lewis C, et al., Osteoslerosis is seen in 20% of patients because the bony trabeculae look prominent in relation to decreased mineralization [4]. X-ray spine AP and lateral views of our patient revealed dense vertebrae.
ROD is classified as osteitis fibrosa, osteomalacia, or mixed, mild, or a dynamic disease; according to the histological features. The frequency at the start of therapy for end stage renal disease has been reported by Hutchison AJ, et al., [5]. On review we have placed our case in variety of mixed disease according to this classification as features of Osteitis fibrosa were coexisting with Osteomalacia.
In our opinion whenever there is a Chronic Renal Disease and the patient has positive radiological findings – should be referred to Orthopedician as they are more aware about ROD. In this case prescriptions revealed that HLA-B27 has also been done assuming Ankylosing Spondylitis.
[1]. Duthie RB, Atkins RM, Metabolic, hormonal and bone marrow diseasesMercer’s Orthopedic Surgery 2003 9th EditionNew DelhiJaypee Brothers Medical Publishers (P) Ltd:302-06. [Google Scholar]
[2]. Moriniere P, Cohen-Solal A, Belbrik S, Disappearance of aluminic bone disease in a long term asymptomatic dialysis population restricting AL(OH), intake: emergence of an idiopathic adynamic bone disease not related to aluminumNephron 1989 53:93-101. [Google Scholar]
[3]. Coburn JW, Slatopolsky E, Vitamin D, parathyroid hormone, and the renal osteodystrophiesThe Kidney 1991 volume 24th EditionPhildelphiaWB Saunders:2036-120. [Google Scholar]
[4]. Lewis C, Brewster M, Gadgil A, Dias R, Chronic renal failure presenting primarily with renal osteodystrophy: A case reportThe Internet Journal of Orthopedic Surgery 2005 2(2)doi:10.5580/2928. Assessed on- 20.03.13. http://archive.ispub.com/journal/the-internet-journal-of-orthopedic-surgery/volume-2-number-2/chronic-renal-failure-presenting-primarily-with-renal-osteodystrophy-a-case-report.html#sthash.HF1FyzDx.dpbs [Google Scholar]
[5]. Hutchison AJ, Whitehouse RW, Boultan HF, Correlation of bone histology with parathyroid hormone, vitamin D3, and radiology in end stage renal diseaseKidney Int 1933 44:1071-7. [Google Scholar]