Iatrogenic Subcutaneous Emphysema of Endodontic Origin – Case Report with Literature Review
Lora Mishra1, Swarnav Patnaik2, Sangram Patro3, Nitai Debnath4, Satyaranjan Mishra5
1Assistant Professor, Department of Conservative Dentistry & Endodontics,Institute of Dental Sciences, S’O’ A University, Bhubaneswar, Odisha, India.
2Assistant Professor, Department of Oral v Maxillofacial Surgery,Hitech Dental College, Bhubaneswar, Odisha, India.
3Assistant Professor, Department of Oral & Maxillofacial Surgery,Hitech Dental College, Bhubaneswar, Odisha, India.
4Assistant Professor, Department of Prosthodontics,College of Dental Sciences and Hospital, Indore, India.
5Associate Professor, Department of Oral Medicine and Radiology,Institute of Dental Sciences, S’O’ A University, Bhubaneswar, Odisha, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lora Mishra, Assistant Professor, Department of Conservative Dentistry & Endodontics, Institute of Dental Sciences. K-8, Ghatikia, Bhubaneswar, Odisha-751003, India.
Phone: +918895266363,
E-mail: loraprankster@yahoo.co.in,misspranky@gmail.com
Surgical emphysema is well known and many case reports have been published on this. Many authors have reported this as a complication post dentoalveolar treatment. Diffusion of air into facial planes and periorbital area during endodontic procedures has been rarely reported. The use of three way air syringe and forceful irrigation of root canal can lead to surgical emphysema of subcutaneous tissue planes in and around the teeth which are involved. This case report highlights one such complication seen during endodontic treatment, discusses aetiology, complications and conservative management of this dental office emergency.
Diffusion, Iatrogenic diseases, High pressure air instruments, Root canal therapy
Case Report
A local dentist referred a 53–year–old female patient with swelling and redness below her left eye, to our hospital. She had developed swelling below her left eye, 10 minutes after conventional endodontic treatment (with sodium hypochlorite and EDTA) of left maxillary central incision. She also complained of persistent and severe sensitivity at the same tooth region and face [Table/Fig-1]. The local dentist, when consulted, admitted that compressed air from three way syringe had been used to dry the canal.
On examination, she was found to have soft swelling with obvious unilateral crepitus below the suborbital region. The swelling was diffuse. The extent of swelling was superiorly from lower eyelid to 3 cm from inferior border of mandible inferiorly. Medially, the extent of swelling was 1cm from bridge of nose to the outer canthus of eye laterally. Eye on same side appeared smaller and it was reddish in colour [Table/Fig-1].
The patient was prescribed tab Augmentin Duo 625mg B.D. for five days. Over the next 7 days, the subcutaneous emphysema resolved progressively and she became asymptomatic [Table/Fig-2] The fascia under the eye also appeared normal [Table/Fig-2and3].
Discussion
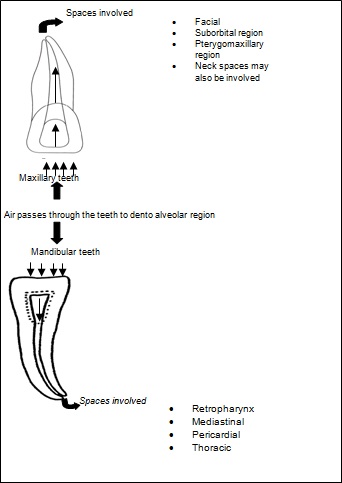
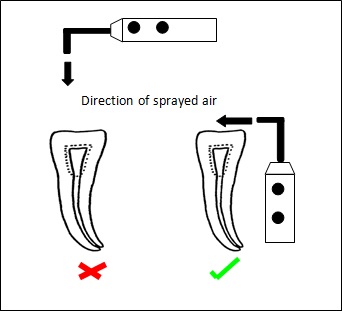
The word emphysema is derived from Greek word, ‘whick’, which means ‘to blow in’ [1]. The use of air syringe for drying the canal during root canal procedure is common practice of most of the clinicians [Table/Fig-4]. Air/ gas can be introduced to soft tissue spaces through either root canal or dentoalveolar membrane [Table/Fig-5] [2]. Two procedures in endodontics, if carried out improperly, have the potential to cause a problem. Firstly, during canal preparation, a blast of air to dry the canal, and secondly, during apical surgery, air from a high-speed drill, can lead to air emphysema. In our case, the air entrapment in sub–orbital space was caused by air blown through air syringe into the root canal. Air syringe operates at 20-25 PSI, this might result in air embolism during root canal therapy [3]. Air can escape into many adjacent spaces [Table/Fig-5]. This might lead to complications [Table/Fig-6]. Differential diagnosis of this complication, that may also produce volume increase, are haematomas, allergic reactions or angio-oedema [4]. The main characteristic signs and symptoms of subcutaneous emphysema are diffuse swelling and characteristic palpable crepitus. Hayduk S et al., reported that crepitus was a pathognomonic sign of tissue space emphysema and that therefore, it could be easily distinguished from angio-oedema [Table/Fig-7] [5]. Radiographs can also be more definitive diagnostic clue for identification of surgical emphysema [Table/Fig-8] [6-25]. These facial and suborbital planes consist of loose connective tissue containing potential spaces between layers of muscles, organs and other structures. Once air enters the deep soft tissue under pressure, as is the case when air–water cooled handpieces or air–water syringes are used, it will follow the path of least resistance through the connective tissue, along the facial planes, spreading to distant spaces [26]. Most patients who develop subcutaneous emphysema after dental procedures have only moderate local swellings [27]. Root canal treatment induced emphysema resolves in few days, administration of prophylactic antibiotics and analgesics can prevent complications because dissemination of oral flora microorganisms along the emphysematous tracts may be responsible for soft tissue infections (e.g. deep neck infection and mediastinitis) and sepsis [28]. This case which has been presented here is unique, as there was only suborbital emphysema with slight redness of the eye [Table/Fig-9]. Pressure drying of any canal seems very unwise and especially so, where the apex is size 25 or larger. In addition to the larger diameter, air flow is probably aided, as the instruments smooth irregularities of the canal walls [29]. Low pressure and side vent needles have been suggested to lessen the danger. But study done by Bradford CE et al., stated that there was no way to ensure complete safety when canals were dried with pressurized air instead use of vacuum. Rather, air under pressure, may be a superior means for canal drying [30]. If at all air syringe had to be used, Jerome suggested that the horizontal 280use of air syringe, in other words, Venturi effect could aid canal drying [Table/Fig-5] Air should be blown across the canal opening to aid drying, and a hand-piece should be employed, that exhausts the spent air out the back of the hand-piece rather than into the operating field [Table/Fig-5] [31].
Various events in the peri–operative period, including endotracheal intubation and positive pressure ventilation, which have also been reported in association with subcutaneous emphysema, can be prevented by following the manufacturer’s recommendations, as to the proper use and maintenance of the air-driven turbine. The usage of rubber dam during dental procedure can also reduce the risk of surgical emphysema. After a dental or surgical procedure, postoperative instructions should include avoidance of coughing, smoking, blowing the nose, using straws, vomiting, or any other activity that may increase pressure in the oral cavity. Excessive inspiratory pressures and volumes should be avoided in cases requiring endotracheal intubation and care should be taken to decrease injury to the tracheal mucosa[Table/Fig-10].
Swelling in left suborbital space

Post 1 week after antibiotic and analigesics administeration

Root canal treated and post 2 week the facia under theleft eye appers normal

Subcutaneous spaces that may get involved if forced air passes through access cavity
Depicting the direction of air syringe used during drying of root canal
Equipment and procedure that can lead to surgical emphysema during endodontic procedure
| Air water cooled syringe | High speed drill | Forceful irrigation of root canal |
Case Reports on Endodontic treatment induced surgical emphysema Also add etiology, treatment and complication if any in this table. it seems incomplete in present state
| Ref no. | Author | Year | Area involved |
| [6] | Shovelton DS | 1957 | Facial, suborbital region & neck |
| [7] | Sumita M et al., | 1970 | Facial subcutaneous tissue |
| [8] | Walker JE | 1975 | Facial subcutaneous tissue |
| [9] | Vasileva M | 1977 | Face and neck subcutaneous tissue |
| [10] | Kaufman AY | 1981 | Facial subcutaneous tissue |
| [11] | Hirschmann PN and Walker RT | 1983 | Facial subcutaneous tissue |
| [12] | Falomo OO | 1984 | Facial subcutaneous tissue |
| [13] | Bottinelli G et al., | 1986 | Facial subcutaneous tissue |
| [14] | Nahlieli O and Neder A | 1991 | Pneumomediastinum |
| [15] | Wright KJ et al., | 1991 | Facial subcutaneous tissue |
| [16] | Penna KJ and Neshat K | 2001 | Cervicofacial |
| [17] | Smatt Y et al., | 2004 | Pneumomediastinum and facial subcutaneous tissue |
| [18] | Sujeet K and Shankar S | 2007 | Prevertebral region. |
| [19] | de Sermeño RF et al., | 2009 | Facial subcutaneous tissue |
| [20] | Parkar A et al., | 2009 | Neck and periorbital region |
| [21] | Kim Y et al., | 2010 | Cervicofacial & Pneumomediastinum |
| [22] | Coulier J and Deprez FC | 2011 | Facial and below the eye subcutaneous tissue |
| [23] | Uyank LO et al., | 2011 | Periorbital area |
| [24] | Hsu HL et al., | 2011 | Facial subcutaneous tissue and eye |
| [25] | Durukan P et al., | 2012 | Cervicofacial emphysema and pneumomediastinum |
Complications of Subcutaneous emphysema
| Early Complication | Delayed complications |
| Involve retropharyngeal, mediastinal and peritoneal spaces which may lead to cardiopulmonary distress. | Secondary infections The secondary infection of the necrotic infraorbital tissues by S. aureus and mortality from sepsis and air embolism |
Clinical features of cervicofacial emphysema
| Immediate | Subsequent |
| Local swelling | Diffuse swelling |
| Crepitus | Local erythema |
| Local discomfort | Pyrexia and Pain |
Severe subcutaneous emphysema the above mentioned radiographs can revel the involvement and spread of emphysema in subcutaneous spaces
| Diagnostic clues |
| Soft tissue radiograph of neck |
| Anteroposterior chest radiograph |
| Lateral chest radiograph |
| CT scan |
Conclusion
Iatrogenic subcutaneous emphysema can have serious and potentially life-threatening effects. When subcutaneous emphysema does arise, it must be quickly diagnosed, understood, and effectively managed, to reduce the incidence of further complications.
[1]. E Kaufman, E Leviner, D Galli, AA Garfunkl, Subcutaneous air emphysema - A rare conditionJ Oral Med 1984 39:47-50. [Google Scholar]
[2]. DE Battrum, JL Gutmann, Implications, prevention and management of subcutaneous emphysema during endodontic treatmentEndod Dent Traumatol 1995 11:109-14. [Google Scholar]
[3]. Trummer Max J, Fosburg Richard G, Mediastinal emphysema following the use of a high-speed.Ann Thorac Surg 1970 9:378-81. [Google Scholar]
[4]. CA Gamboa Vidal, CA Vega Pizarro, A Almeida Arriagada, Subcutaneous emphysema secondary to dental treatment: Case ReportMed Oral Patol Oral Cir Bucal 2007 12:E76-8. [Google Scholar]
[5]. S Hayduk, Subcutaneous emphysema after operative dentistry: report of a case.Am Dent Assoc 1970 80(1362) [Google Scholar]
[6]. DS Shoveton, Surgical emphysema complications of dental operationsBrt Dental J. Feb 19, 1957 :102-25. [Google Scholar]
[7]. M Sumita, S Suzuki, K Fujii, Three cases of accidental occurrence of the facial subcutaneous emphysema following root canal treatmentAichi Gakuin Daigaku Shigakkai Shi. 1970 8(2):106-12. [Google Scholar]
[8]. JE Walker, Emphysema of soft tissues complicating endodontic treatment using hydrogen peroxide: a case report.Br J Oral Surg 1975 13(1):98-99. [Google Scholar]
[9]. M Vasileva, Face and neck subcutaneous emphysema in root canal therapyStomatologiia (Sofiia) 1977 59(2):119-21. [Google Scholar]
[10]. AY Kaufman, Facial emphysema caused by hydrogen peroxide irrigation: report of a caseJ Endod 1981 7(10):470-72. [Google Scholar]
[11]. PN Hirschmann, RT Walker, Facial emphysema during endodontic treatment – two case reports.Int Endod J 1983 16(3):130-32. [Google Scholar]
[12]. OO Falomo, Surgical emphysema following root canal therapy. Report of a case.Oral Surg Oral Med Oral Pathol 1984 58(1):101-2. [Google Scholar]
[13]. G Bottinelli, C Arrigoni, G Flecchia, Description of a case of subcutaneous emphysema as a consequence of endodontic treatmentAnn Osp Maria Vittoria Torino 1986 29(1-6):43-9. [Google Scholar]
[14]. O Nahlieli, A Neder, Iatrogenic pneumomediastinum after endodontic therapy.Oral Surg Oral Med Oral Pathol 1991 71(5):618-9. [Google Scholar]
[15]. KJ Wright, GD Derkson, KH Riding, Tissue-space emphysema, tissue necrosis, and infection following use of compressed air during pulp therapy: case report.Pediatr Dent 1991 13(2):110-3. [Google Scholar]
[16]. KJ Penna, K Neshat, Cervicofacial subcutaneous emphysema after lower root canal therapyN Y State Dent J 2001 67(5):28-29. [Google Scholar]
[17]. Y Smatt, H Browaeys, A Genay, G Raoul, J Ferri, Iatrogenic pneumomediastinum and facial emphysema after endodontic treatmentBr J Oral Maxillofac Surg 2004 42(2):160-62. [Google Scholar]
[18]. K Sujeet, S Shankar, Images in clinical medicine. Prevertebral emphysema after a dental procedureN Engl J Med 2007 356(2):173 [Google Scholar]
[19]. RF de Sermeño, LA da Silva, H Herrera, RA Silva, MR Leonardo, Tissue damage after sodium hypochlorite extrusion during root canal treatment.Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009 108(1):e46-9. [Google Scholar]
[20]. A Parkar, C Medhurst, M Irbash, C Philpott, Periorbital oedema and surgical emphysema, an unusual complication of a dental procedure: a case reportCases J 2009 2(8108) [Google Scholar]
[21]. Y Kim, MR Kim, SJ Kim, Iatrogenic pneumomediastinum with extensive subcutaneous emphysema after endodontic treatment: report of 2 casesOral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 109(2) [Google Scholar]
[22]. J Coulier, FC Deprez, Iatrogenic Facial subcutaneous emphysema after endodontic treatment.JBR-BTR 2011 94(1):38 [Google Scholar]
[23]. LO Uyanık, M Aydın, O Buhara, A Ayalı, Kalender A. Periorbital emphysema during dental treatment: a case reportOral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011 112(6):e94-6. [Google Scholar]
[24]. HL Hsu, CC Chang, KL Liu, Subcutaneous emphysema after dental procedure.QJM 2011 104(6):545 [Google Scholar]
[25]. P Durukan, O Salt, S Ozkan, B Durukan, Cervicofacial emphysema and pneumomediastinum after a high-speed air drill endodontic treatment procedureAm J Emerg Med 2012 30(9):2095 [Google Scholar]
[26]. Andrew Mather J, Andrew Stoykewych A, Cervocofacial and Mediastinal emphysema complicating a dental procedure.J Can Dent Assoc 2006 72(6):565-6.8. [Google Scholar]
[27]. J Frühauf, R Weinke, U Pilger, H Kerl, Müllegger RR Soft tissue cervicofacial emphysema after dental treatment: report of 2 cases with emphasis on the differential diagnosis of angioedema.Arch Dermatol 2005 141(11):1437-40. [Google Scholar]
[28]. Hülsmann Hahn Complications during canal irrigationInternational Endodontic Journal. 2000 33:186-93. [Google Scholar]
[29]. Eleazer Paul D, Eleazer Kristen R, Air pressures developed beyond the apex from drying root canals with pressurized airJournal of Endodontics 1998 24(12):833-36. [Google Scholar]
[30]. CE Bradford, PD Eleazer, KE Downs, JP Scheetz, Apical pressures developed by needles for canal irrigation.J Endod 2002 28(4):1437-40. [Google Scholar]
[31]. Ingle John I, K Bakland Leif, Endodontics 1994 86th Edition:215-34. [Google Scholar]