Introduction
Dental caries has been known since times immemorial. Although there has been a substantial reduction of the prevalence of caries in industrialized countries, this disease continues to be widespread in the world. Once it has become installed, it is of fundamental importance to use conservative procedures that simultaneously prevent lesion progress and minimize healthy tooth structure wear [1]. The most serious problem encountered during caries removal is anxiety, fear and pain. Pressure and heat during mechanical preparation and the annoying noise from the handpiece are to blame. Furthermore, mechanical bur drilling often causes over preparation of sound healthy dentin, leading sometimes to pulp inflammation and even exposure.
System for caries removal and cavity preparation have been under strong pressure for development towards minimal invasive procedures and increased patient comfort. Conventional caries removal involved the use of a drill on a high-speed handpiece to gain access to the carious lesion and slow handpiece to remove carious dentine. This was perceived as unpleasant and painful by many patients, so local anaesthesia had to be administered to control pain [2]. The drill removes both infected and affected dentine, it may cause an unnecessary weakness of the tooth structure and also increases the possibilities of damaging the pulpal tissue [3]. During the last few decades, many alternative methods for cavity preparation and caries removal have been introduced, including atraumatic restorative treatment, air abrasion, Chemo-mechanical systems and most recently hard tissue lasers [4].
A new method based on chemicals to remove carious lesion has been launched, Chemo-mechanical Caries Removal method (CMCR). This procedure has gained inportance due to the selective removal of carious dentine and avoidance of painful and unnecessary removal of sound dentine. Restoration of cavities prepared by such technique requires materials such as composite resins or glass ionomer which bond to the dentine surface, rather than materials such as, amalgam which involves the cutting of cavity designed to mechanically retain the restoration [5].
With advent of newer technology of caries removal by Carisolv, this Review article enlightens the present knowledge on this new chemo-mechanical system of caries removal. It is claimed to reduce the need of anesthesia, to preserve the tooth structure, decrease the use of rotary instruments and to relieve anxiety efficiently [6]. This article will help the readers in gaining the knowledge on evolution of Carisolv; method of application, indications, advantages, disadvantages and various studies conducted in comparison to other techniques of caries removal. It will also augment the wisdom on the Chemo-mechanical caries removal system and the mechanism of action supplementing the clinical usage of the material in a routine practice.
Structure of collagen
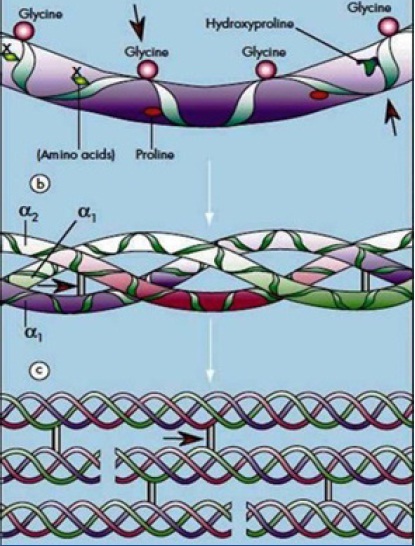
Dentine consists of (70% wt) inorganic portion, (10%wt) water and an (20%wt) organic matrix. Of this organic matrix, 18% are collagen and 2% non-collagenous compounds. Collagen is a protein containing large amount of proline. The polypeptide chains are coiled into triplet helices which are known as tropocollagen units; these tropocollagen units then re-orient side by side to form a fibril. Co-valent bonds between polypeptide chains and the tropocollagen units form cross-links and give the collagen fibrils stability. When caries occurs, dentinal tubules provide access for penetrating acids and subsequent invasion of bacteria. This results in a decrease in pH which further causes acid attack, demineralization and dissolution of inoranic and organic matter. CMCR reagent causes further degradation of this partially degraded collagen, by cleavage of the polypeptide chains in the triple helix and/or hydrolyzing the cross-linkages as [5] shown in [Table/Fig-1].
Structure of collagen and mode of action of Carisolv
a. Polypeptide chain – possible sites where CMCR will cause cleavage by acting on glycine and hydroxyproline
b. Triple helix structure- red arrows depicts the site for cleavage at intramolecular cross linking
c.Tropocollagen unit to form collagen fibril. Red arrows depicts the site for cleavage at intra- molecular cross linking as modified from Dow et al., 1996
Mechanism of action
The mechanism of action of NMG (N-monochloroglycine) and NMAB (N Monochloroaminobutyric acid) on collagen is still unclear and knowledge of the chemistry of chlorination of amino acids and their effects is still very limited. Originally, it was thought that the procedure involved in chlorination of the partially degraded collagen in the carious lesion and the conversion of hydroxyproline to pyrrole-2-carboxylic acid. More recent work suggests that cleavage by oxidation of glycine residues could also be involved. This cause disruption of collagen fibrils which become more friable and can then be removed.
Evolution of Caridex
The NMAB system was patented in the US in 1975, and further patented by National Patent Dental Corporation, New York in 1987. It received FDA approval for use in USA in 1984, and was marketed in 1980’s as Caridex.
GK 101 turned out to act slowly and additional efforts to speed up the procedure resulted in GK 101E. Based on GK 101E, a caries removal system called Caridex gained FDA acceptance in 1984. Research was carried out documenting clinical efficacy and safety. It consisted of two solutions which were mixed immediately before use, and was stable for only one hour [6]. A delivery system consisted of a reservoir for the solution, a heater and a pump which passed the liquid warmed to body temperature through a tube to a handpiece and an applicator tip available in various shapes and sizes [7]. Both the solutions in Caridex required immediate mixing followed by warming in the heater to the body temperature and pump used to pass to the hand piece.
Eventually shortcoming with Caridex became apparent [8]:
Efficacy and speed of caries removal needed improvement.
It was expensive.
Large quantities were required for intermittent use during excavation.
The solution had to be heated.
A large reservoir with pump was needed for application and the product was delivered in large containers.
The shelf-life of an opened container was short.
The hand instruments were not optimal.
The product was launched in an era when new dentine bonding agents were not considered reliable, instead mechanical undercuts created by drilling were needed for retention.
The shortcomings of the Caridex system were addressed in the development of Carisolv.
However, Mediteam in Sweden continued to work on the material and finally in 1998, Carisolv was marketed. Carisolv is available in a gel form which did not require any delivery system or heating [2].
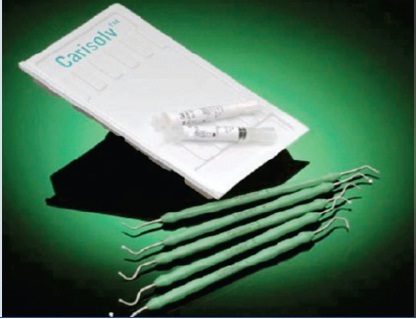
Presently, it is available in two forms, single mix and multi-mix as depicted in [Table/Fig-2,3]. In single mix, two syringes are available, one containing sodium hypochlorite solution and the other containing three aminoacids: lysine, leucine and glutamic acid with carboxymethyl cellulose, to make a viscous consistency. Recently, a multi-mix syringe has been introduced which contains the ingredients of both the syringes and dispenses the exact amount of required material.
Multi-mix Carisolv gel and instruments

Single mix Carisolv gel and instruments
Importance of Addition of urea
It was observed that Caridex was more effective in deciduous teeth compared to permanent. Thus, to improvise the efficacy of Caridex, an attempt was made by adding urea, which normally denatures protein by breaking down hydrogen bonding thereby, making them more soluble [5].
An in vitro study was carried out by Yip HK et al., in which it was observed, that after treatment with NMAB (N-Monochloroaminobutyric acid) or NMAB-urea, the surface appearance was very uneven with many undermined areas. The addition of urea to NMAB resulted in an improvement in the efficacy of caries removal. The performance was better in primary teeth [6].
H Yip, A Stevenson, J Beeley, executed an in vitro study which concluded that NMAB-urea was more effective than NMAB alone for complete caries removal while both reagents were more effective than a saline control which was statistically significant [9,10].
Hand Instruments
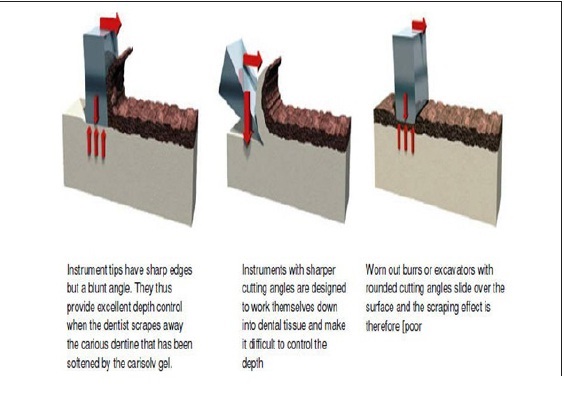
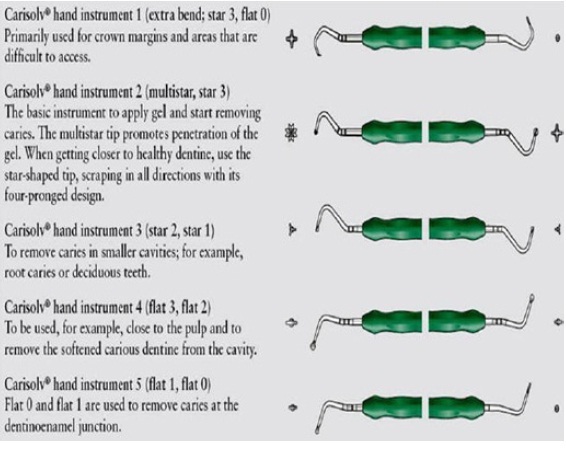
When the lesion has been accessed and the dentine been softened by the Carisolv gel; special hand instruments as shown in [Table/Fig-4] are used to remove the carious tissue layer by layer. The instruments are available with permanent or interchangeable tips designed to access different types of lesions. Most of the Carisolv instruments have a sharp edge and blunt cutting angles, resulting in a large area of support against the underlying surface coupled with controlled and effective cutting depth as demonstrated in [Table/Fig-5]. Other drills and excavators tend to work their way into materials in a non-precise manner due to their aggressive cutting angles and smaller support areas.
Mode of action of carisolv instruments
Different types of instruments used with Carisolv
Mix the two components thoroughly, according to the instructions, if using the single mix gel.
With an instrument carry the Carisolv gel to the carious tooth; if required a handpeice may be used to open up the cavity.
Wait for at least 30 seconds for the chemical process to soften caries till the gel appears cloudy.
Scrape off the softened carious dentine.
Keep the lesion soaked with gel and continue scraping.
When the cavity is free from caries, remove the gel and wipe the cavity with a moistened cotton pellet or rinse with luke warm water. Inspect with a sharp probe. If the tooth is not caries free apply again and continue scrapping.
Clinical Studies
Patient acceptance
Caries excavation has always been performed using rotary and hand instruments. There have been some drawbacks associated with caries removal. Often, due to lack of clinical parameters to judge how much caries to be removed unintentional pulp exposure takes place. This can also be attributed to lack of clinical knowledge of the clinician. Although, caries excavation is also associated with the discomfort caused due to vibration, noise, pain and the heat generation. The Chemo-mechanical caries removal method selectively removes carious dentine and avoids the painful and unnecessary removal of sound dentine. It facilitates delivery of atraumatic, bactericidal and bacteriostatic activity, while removing the least amount of tooth structure and not leaving behind any infected and untreatable dentin. It has been observed in various studies like Kavvadia K, Karagianni V, that the need of anesthesia is reduced in Carisolv compared to conventional methods, thus the co-operation of patient is sometimes more or at par to conventional methods. The co-operation of patients treated with Chemo-mechanical technique was similar to the patients treated with the conventional method. The results by various authors suggested that prolonged treatment time did not greatly influence behavior, at any age [12]. Kakaboura A, Masouras C also observed similar results [13]. Nadanovsky P et al., evaluated the efficacy and comfort of patients by hand excavation and Carisolv and stated that Carisolv was a successful material and observed a difference in certain level of comfort [14]. Thus, acceptance of Carisolv as an alternative to other techniques has a high level of acceptance.
Efficacy of caries removal
Efficacy of caries removal has been of utmost importance. Complete removal of caries is required for the success of the treatment. If caries remain in the cavity, secondary caries can develop. To evaluate the efficacy of caries removal a clinical parameter is required. Many studies were carried to evaluate the efficacy of caries removal. The efficacy of caries removal determined using Ericson et al., scale was the highest with Airotor, followed by almost comparable effectiveness by Carisolv method and the least by hand instruments. Pandit IK et al., compared the different methods of caries hand instruments, Airotor and Carisolv. The results showed that airotor was the most efficient method amongst all techniques, while Carisolv was the least painful and most time consuming method [15].
Banerjee A, Kidd EA and Watson TF, also evaluated the efficiency and effectiveness of caries excavation and observed that the Carisolv gel, air-abrasion and hand excavation methods were found to prepare the cavities of a similar extent when related to the AutoFlourescence signature of the lesion, whereas the bur technique tended to over prepare cavities and the Sono-abrasion tended to under prepare its cavities [16]. Hahn et al., performed a microcomputed tomographic assessment of caries removal by Carisolv which led to the result that density of dentine remaining after caries removal was 81.8% of sound dentine [17].
Root caries removal
Root carious lesions are mostly accessible without preceding drilling and therefore suited to the use of Carisolv. Thus, Fure S et al., conducted a study, with an objective to evaluate clinical efficiency, treatment time and patient perception of chemo-mechanical method of caries removal of primary root caries and conventional drilling. They found that in Carisolv group, none of the patients who did not use anaesthesia experienced any pain. No complication or adverse effects were reported during the follow-up year [18]. Carisolv is an efficacious method in root caries removal, though associated with longer duration of treatment.
Use in root canal treatment
The main goal in root canal treatment is to eliminate infection and substrate from the root canal and to prevent its recurrence. This procedure still proves to be complicated and has remained controversial for a number of reasons in the paediatric population. Mainly, the perceived difficulty of behavior management, uncertainty about the effects of root canal filling material and instrumentation on the succedaneous teeth, anatomic situations like the often complicated, curved and tortuous root canals and closeness of the advancing tooth buds, make the treatment more difficult. Despite the outstanding advancement reached in all fields of dental research, search for the ideal irrigant solution still challenges endodontics and therefore, great effort has been focused on assessing the potential of different substances for root canal irrigation. Conventional root canal treatment includes mechanical instrumentation in combination with antimicrobial and tissue solvent irrigation to dissolve and dislodge debris, and create a clean environment compatible with periapical health. In the case of deciduous teeth, extensive dentine removal is probably undesirable, placing greater emphasis on irrigants for cleansing. Sodium hypochlorite is the most widely recommended endodontic irrigant because of its excellent tissue solvent and antimicrobial properties in concentrations between 0.5 and 5.25%, but it is known to cause serious damage when allowed to enter periradicular tissues even in small amounts. Carisolv is a well-researched product which is advocated for chemo mechanical removal of infected carious dentine [19]. Kilani MG et al., ascertained that Carisolv is more effective than physiological saline in removing debris from the uninstrumented walls of root canals. Carisolv cleaned canals more effectively than Phosphate Buffer Saline but never reached the consistent high levels of cleanliness achieved with strong sodium hypochlorite, even after long incubation times and ultrasonic agitation [20].
Comparison with other methods of Caries removal
Conventioninal drilling causes a lot of noise and vibration which leads to irritation and anxiety amongst patients. Innovative techniques have been able to reduce the burden of fear of vibration while undergoing dental treatment to a great extent. Due to the shortcomings of the drill, alternative techniques like air abrasion, ultrasonic instrumentation, lasers and Chemo-mechanical approach to caries removal were developed. Amongst these, air abrasion, sonoabrasion, ultrasonic instrumentation and lasers are costly and tooth-sensitive methods and therefore less frequently used. Therefore, Carisolv is an adept method to reduce the pateient discomfort.
CMCR has been claimed to be advantageous over Airotor and Convention drill due to reduction in noise and vibration [4]. Carisolv also overcomes the diasadvantage of overpreparation of the cavity by conventional drilling as only degraded collagenous dentin is removed. Selective removal of caries by CMCR claims to eliminate the symptom of pain and is a preffered treatment compared to convention drill [3]. The need of anaesthesia is also observed to be less in Carisolv. It can be argued that Carisolv system is effective in the removal of caries and causes minimum pain episode. Compared to hand excavation, Carisolv system seems to be a promising restorative approach to remove occlusal caries [21]. Laser, air abrasion and sonoabrasion techniques also have additive benefits but they do not selectively remove the dental caries. Thus, Carisolv has a edge over the other minimally invasive techniques of caries removal.
With the advent of recent concepts in minimal invasive dentistry, Papain has also been a Chemo-mechanical caries removal agent. On comparison with Carisolv, it has been observed by Kumar J, Nayak M, Prasad K L, Gupta N that the time for caries removal with Carisolv and Papacarie were, 11.67 ± 3.25 minutes and 10.48 ± 2.96 minutes (p>.05) respectively. The mean volume of carious tissue removed with Papacarie (135.99 ± 66.43 mm 3) was higher than that with Carisolv (126.33 ± 53.56 mm 3); however, the difference was not significant [22].
Caries removal in children has always been challenging. Any technique in this regard which is efficacious and reduces the pain and anxiety has always been desired. It has been postulated by Bohari MR and associates [23], that the techniques like CMCR and laser irradiation have been established to be minimally invasive methods and less painful. Airotor, Carisolv, Papacarie and Er:YAG laser were compared to evaluate the efficacy and efficiency of caries removal. It was ascertained that Airotor and laser were more effective and efficient method in removal of caries, whereas laser and CMCR methods were observed to be more comfortable methods. Kochhar GK and colleagues [24] also corroborated that Chemo-mechanical removal of caries with Papacarie and Carisolv were found to be effective measures of caries removal and could be considered as viable alternatives to painful procedures like Airotor in management of dental caries especially in children. Though associated with longer duration of treatment, it can be disadvantageous in paediatric patients when it is difficult to intend to show co-operation for a prolonged duration. While the anxiety is reduced when no drilling is carried out.
Effect on pulp
Caries may sometimes approach pulp. Any method used in caries removal should not cause any deleterious effect on pulp leading to pulpal inflammation, as this may result in severe pain or infection. This was eventually proved by Dammaschk T and colleagues, as they concluded that the pulpal and predentin fibrils, as well as, the dentin fibrils appeared to be intact and did not differ from the controls [25]. In another study by Dammaschke T and fellows, it was observed that pulp reaction was essentially the same as those reported in the past being typical for the effect of calcium hydroxide as a direct pulp capping agent. Thus, it was concluded that compared to Ca(OH)2,Carisolv did not cause any different or additional pulp reaction in healthy teeth [26].
Effect on bond strength
In the operative treatment of carious lesions in dentin, the morphology and nature of the prepared dentin, influences the bonding of adhesive restorative materials. Strong durable bond between dental biomaterials and tooth substrate are essential, not only from a mechanical stand point, but also from biological and esthetic perspectives. For successful bonding between the dentin and restoration, initial emphasis was placed upon the penetration of material into dentin tubules to provide retention via resin tags, but now it is understood that resin penetration into the three dimensional network of collagen found in the intertubular, demineralized matrix will also provide significant levels of bonding. As modern dentin adhesives demonstrate remarkable differences in treatment of the smear layer, substrate surface alterations after Chemo-mechanical caries removal or even the application of these chemical solutions on sound dentin possibly influence the adhesion of resin composites to these surfaces. With respect to changes in the dentine, the work by Dammaschke et al., demonstrated that Carisolv can cause damage to odontoblast processes but leaves the dentinal collagen intact. Therefore, this should not cause any problems when bonding to dentine [27]. Burrow et al., stated that there was no significant difference in the bond strengths, although each group treated with the Carisolv had a slightly lower bond strength [28]. An increase in surface energy with higher wettability and a reduced mineral content of the dentin surface have been observed after Chemo-mechanical caries removal. The Carisolv reagent selectively removes carious dentin, leaving a surface with many overhangs and undercuts, with dentinal tubules both patent and occluded, and is claimed to disrupt the collagen fibers that have been alterated by the carious process. Bond formed with this surface and glass ionomer has been shown to be stronger than with a conventional smear layer. The influence of Carisolv on resin adhesion to sound human primary and young permanent dentin has been reported by Hosoya et al., who reported that dentin treated with Carisolv before application of adhesive systems and resin composite significantly increased Shear Bond Strength (SBS) to permanent dentin but did not significantly increase SBS to primary dentin.
Bactericidal properties
Among the cariogenic micro-organisms, Streptococcus mutans and Lactobacillus species are detected in significant quantities in carious dentine. Further studies are needed to evaluate new methods of removing carious tissue which removes the cariogenic bacteria with a minimally invasive method. Gisele Quariguasi Tobias et al., evaluated the influence of Chemo-mechanical (Carisolv) and mechanical (low speed drills and conventional dentinal curettes) methods on the reduction of the number of S. mutans and Lactobacillus [29].
Cost
The application of Carisolv in clinical practice might be limited because of the material cost. This limitation can be overlooked by the advantages associated with Carisolv, such as reduced pain and anxiety associated with the drill while removing the carious lesion.
Disadvantages of Carisolv
Time-consuming
Unpleasant smell
Unpleasant taste
Costly
Due to prolonged time the patient may become un-cooperative
Limited shelf life
Wastage of material while re-application
Conclusion
Wherever possible, tissue should be preserved; invasive treatment should be kept to a minimum and natural tissue should be replaced with artificial substitutes only when it is absolutely unavoidable. The best way to ensure maximum life for the natural tooth is to respect the sound tissue and protect it from damage by using minimally invasive techniques in restorative dentistry. Chemo-mechanical caries removal agent has been proved to be an efficient method of caries removal. Though it takes more time for caries removal but it reduces the anxiety, need of anesthesia, pain and removes only infected dentin. Thereby, preserving tooth tissue, combined with a patient-friendly approach. Thus, it can bring promising results in children, old patients, anxious patients and special care need children.
[1]. Correa FN, Rocha RO, Filho LER, Chemical versus conventional caries removal techniques in primary teeth: A microhardness studyJournal of paediatric dentistry 2007 31(3):187-92. [Google Scholar]
[2]. Ericson D, The efficacy of a new gel for chemo-mechanical caries removal (abstract 360)Journal of Dental Research 1998 77(5):1252 [Google Scholar]
[3]. Chourio MAZ, Zambrano O, Clinical randomized controlled trial of Chemo-mechanical caries removalInternational journal of paediatric dentistry 2006 16:161-67. [Google Scholar]
[4]. Kakaboura A, Masouras C, A comparative clinical study on the Carisolv caries removal methodQuintessence international 2003 34:269-71. [Google Scholar]
[5]. Beeley A, Yip HK, Stevenson AG, Chemo-mechanical caries removal: a review of the techniques and latest developmentsBritish dental journal 2000 188(8):427-30. [Google Scholar]
[6]. Erricson D, Zimmermen M, Raber H, Clinical evaluation of efficacy and safety of a new method for chemo-mechanical removal of cariesCaries research 1999 33:171-77. [Google Scholar]
[7]. Ganesh M, Parikh D, Chemo-mechanical caries removal (CMCR) agents: Review and clinical application in primary teethJournal of Dentistry and oral hygiene 2011 3(3):34-45. [Google Scholar]
[8]. Raju HG, New trends in treatment of dental caries in outreach programme – CarisolvAnnals and essence of Dentistry 2011 3:1.4.6 [Google Scholar]
[9]. Yip HK, Stevenson AG, Beeley JA, An improved reagent for Chemo-mechanical caries removal in permanent and deciduous teeth: an in vitro studyJ Dent 1995 Aug 23(4):197-204. [Google Scholar]
[10]. Yip HK, Stevenson AG, Beeley JA, Chemo-mechanical removal of dental caries in deciduous teeth: further studies in vitroBritish dental journal 1999 :186179-82. [Google Scholar]
[11]. Mediteam. New Carisolv gel for faster treatment.[cited on 1999 Dec 4]. Available from: http://www.mediteam.com/gelinst/pdf. [last accessed on] 24th July 2013 [Google Scholar]
[12]. Kavvadia K, Karagianni V, Primary teeth caries removal using the Carisolv Chemo-mechanical method: A Clinical trialPaediatric dentistry 2004 26(1):23-28. [Google Scholar]
[13]. Kakaboura A, Masouras C, A comparative clinical study on the Carisolv caries removal methodQuintessence international 2003 34:269-71. [Google Scholar]
[14]. Nadanovsky P, Removal of caries using only hand instruments: A comparison of mechanical and chemo-mechanical methodsCaries Research 2001 35:384-89. [Google Scholar]
[15]. Pandit IK, Srivastava N, Gugani N, Gupta M, Verma L, various methods of caries removal in children: A comparative clinical studyJ Indian Soc Pedo Prev Dent June 2007 :93-97. [Google Scholar]
[16]. Banerjee A, Kidd EAM, Watson TF, In vitro evaluation of five alternative methods of carious dentine excavationCaries research 2000 34:144-150. [Google Scholar]
[17]. Hahn SK, Kim JW, Lee SH, Microcomputed tomographic assessment of Chemo-mechanical caries removalCaries research 2004 38:75-78. [Google Scholar]
[18]. Fure S, Lingstorm P, Birkhed D, Evaluation of Carisolv for the Chemo-mechanical removal of primary root caries in vivoCaries research 2000 34:275-280. [Google Scholar]
[19]. Singhal P, Das UM, Vishwanathan D, Singhal A, Carisolv as an endodontic irrigant in deciduous teeth: An SEM studyIndian J Dent Res 2012 23:120-1. [Google Scholar]
[20]. Kilani MG, Whitworth JM, Dummer PMH, Preliminary in vitro evaluation of Carisolv as a root canal irrigantInternational endodontic journal 2003 36:433-440. [Google Scholar]
[21]. Kirzioglu Z, Gurbur T, Yilmaz Y, Clinical evaluation of Chemo-mechanical and mechanical caries removal: status of the restorations at 3,6,9 and 12 monthsClinical Oral Investig 2007 11(1):69-76. [Google Scholar]
[22]. Kumar J, Nayak M, Prasad K L, Gupta N, A comparative study of the clinical efficiency of Chemo-mechanical caries removal using Carisolv and Papacarie - A papain gelIndian J Dent Res 2012 23:697 [Google Scholar]
[23]. Bohari MR, Chunawalla YK, Ahmed BM, Clinical evaluation of caries removal in primary teeth using conventional, Chemo-mechanical and laser technique: an in vivo studyJ Contemp Dent Pract 2012 Jan 1 13(1):40-7. [Google Scholar]
[24]. Kochhar GK, Srivastava N, Pandit IK, Gugnani N, Gupta M, An evaluation of different caries removal techniques in primary teeth: a comparitive clinical studyJ Clin Pediatr Dent 2011 36(1):5-9. [Google Scholar]
[25]. Dammaschk T, Stratmann U, Mokrys K, Kaup M, Ott KH, Histocytological evaluation of reaction of rat pulp tissue to CarisolvJournal of Dentistry 2001 May 29(4):283-290. [Google Scholar]
[26]. Erhardt In vitro influence of Carisolv on shear bond strength of dentin bonding agentsQuintessence international 2004 35(10):801-07. [Google Scholar]
[27]. Dammaschke T, Stratmann U, Danesh G, Schäfer E, Ott K, H. R. Reaction of rat pulp tissue to Carisolv “new gel’—-A histocytological evaluationAustralian Dental Journal 2006 51(1):57-63. [Google Scholar]
[28]. Burrow MF, Bokas J, Tanumiharja M, Tyas MJ, Microtensile bond strengths to caries-affected dentine treated with CarisolvAustralian dental journal 2003 48(2):110-114. [Google Scholar]
[29]. Gisele Quariguasi Tobias, Comparision of Chemo-mechanical and mechanical method of caries removal in the reduction of streptococcus mutans and lactobacillus spp in carious denine of primary teethJournal of applied oral science 2005 13(4):399-405. [Google Scholar]